
Abstract
Objective
The effect of patient age on the outcome of Sun’s procedure for acute type A aortic dissection (ATAAD) remains controversial. We retrospectively investigated the early outcomes of Sun’s procedure in elderly patients with ATAAD in our single center.
Methods
This study involved 106 patients who underwent Sun’s procedure. The patients were divided into the elderly group (≥70 years, n = 17) and younger group (<70 years). Baseline, intraoperative, and postoperative data were compared between the groups.
Results
The mean age in the elderly and younger groups was 75.7 and 50.7 years, respectively. The type of aortic root operations were not significantly different between the groups. Concomitant surgeries were more frequently performed in the elderly group, but without statistical significance. All intraoperative cardiopulmonary bypass variables as well as the in-hospital and 30-day mortality rates were similar between the groups. The incidences of most postoperative complications were also similar except for a higher incidence of sepsis in the elderly group.
Conclusions
Emergency performance of Sun’s procedure for patients with ATAAD characterized by dissection and/or entry tear in the aortic arch should not be denied on the basis of advanced age alone. Comparable early in-hospital outcomes can be achieved in elderly patients.
Keywords
Introduction
Acute aortic dissection (AAD) is characterized by rapid development of an intimal flap caused by blood flowing into the media and forcing the intima and adventitia apart. 1 The AAD-associated mortality rate can reach 33% within the first 24 hours, 50% by the first 48 hours, and 70% within 1 week if left untreated.2,3 The reported incidence of AAD is 3 to 5 cases per 100,000 people per year, which may be underestimated because many pre-admission deaths were not included in these statistics.4,5 Despite the development of diagnostic tools and advancements in therapeutic techniques, life-saving surgical treatment of acute type A aortic dissection (ATAAD) is still associated with an in-hospital mortality rate of 22%.6,7 For patients with ATAAD involving the ascending aorta, aortic arch, and descending aorta, Sun’s procedure is now becoming increasingly utilized worldwide. 8 However, Sun’s procedure is a complex operation that requires deep hypothermic circulatory arrest (DHCA) or low flow, selective cerebral perfusion, a long cardiopulmonary bypass (CPB) time, and a long operation time compared with other general cardiac surgeries. Thus, in elderly patients with ATAAD, Sun’s procedure may present challenges for the clinicians, patients, and patients’ families. Studies of the effect of patient age on the outcomes of ATAAD treated by Sun’s procedure have also produced conflicting results.9–11 In this single-center retrospective study, we investigated the early outcomes of Sun’s procedure in elderly patients with ATAAD.
Material and methods
Patient population
The reporting of this study conforms to the STROBE guidelines. 12 From October 2019 to September 2020, 166 patients underwent emergency treatment for ATAAD in our institution. Only patients treated with Sun’s procedure for dissection, significant hematoma, and/or entry tear in the aortic arch as diagnosed by preoperative computed tomography were included in this study. Patients who were older than 90 years; had been diagnosed with immune disease, chronic renal failure, end-stage liver disease, or infectious disease; had a history of malignant tumors; had heart failure with a left ventricular ejection fraction of <45%; or had incomplete records were excluded from this analysis. In total, 106 patients (64%) met all stated criteria, and their data were retrospectively analyzed. These patients were divided into two groups: those aged ≥70 years (elderly group) and those aged <70 years (younger group). The primary endpoint was in-hospital mortality. This study was approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University, and written informed consent was obtained from all patients for study participation and publication of the results.
Surgical technique
After induction of general anesthesia, invasive blood pressure was monitored via the left radial artery and dorsalis pedis artery. Ice bags were routinely packed around the head, and near-infrared spectroscopy sensors were placed on the forehead above the frontal lobes bilaterally to assess regional cerebral oxygenation. 13
All operations were performed through a standard median sternotomy approach under CPB. The right axillary artery was routinely exposed for arterial cannulation. Myocardial protection was carried out by retrograde modified del Nido cardioplegia via the coronary sinus. The diseased aortic root was reconstructed by ascending aorta replacement, the David procedure, or the Bentall procedure with a four-branched graft during the cooling process. When the nasopharyngeal temperature reached approximately 25°C, DHCA with selective cerebral perfusion through the right axillary artery and left carotid artery (5–10 mL/kg) was initiated. Further surgical details are described in a previous report. 8 If the pressure gradient between the upper and lower extremity was >40 mmHg, aortofemoral bypass was performed with an expanded polytetrafluoroethylene vascular prosthesis. If the right coronary ostium was involved in the dissection, coronary artery bypass grafting was performed using the greater saphenous vein.
Data collection
Clinical baseline data including sex, age, body mass index, laboratory parameters, and basic diseases were retrospectively collected. Hemodynamic instability was defined as a systolic blood pressure of <80 mmHg. Malperfusion syndrome included cerebral, renal, mesenteric, and extremity ischemia. Intraoperative variables including the aortic root procedure, concomitant aortofemoral bypass or coronary artery bypass surgery, DHCA time, aortic cross-clamping time, and CPB time were also collected. Postoperative laboratory test results (24 hours postoperatively), the application of continuous renal replacement therapy, the incidence of hypoxemia at 72 hours postoperatively (PaO2/FiO2 of <200 mmHg), length of intensive care unit stay, ventilation time, in-hospital death, and 30-day mortality were all reviewed.
Statistical analysis
IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA) was used for the statistical analysis. The presentation of data included values, percentages, and medians. Continuous data are presented as mean ± standard deviation. Categorical variables are presented as percentages. Categorical data were analyzed using the χ2 test or Fisher’s exact test. Continuous variables were compared between groups using Student’s t-test. A P value of <0.05 was considered statistically significant.
Results
All demographic data except age and clinical risk factors (hypertension, history of smoking and drinking, and diabetes mellitus) were similar between the two groups (Table 1). There was also no significant difference in preoperative malperfusion syndrome or hemodynamic instability. The patients in the elderly group were significantly older than those in the younger group (P < 0.001).
Patients’ baseline characteristics.

Data are presented as mean ± standard deviation or n (%).
M, male; F, female; BMI, body mass index.
Preoperative and postoperative laboratory test results were compared between the two groups. The preoperative albumin level was significantly lower in the elderly group than in the younger group (P = 0.03). The preoperative estimated glomerular filtration rate was significantly higher in the elderly group than in the younger group (P < 0.01). The postoperative platelet and fibrinogen levels were also significantly lower in the elderly group than in the younger group (P = 0.03 and P = 0.02, respectively). The postoperative myoglobin level was significantly higher in the elderly group than in the younger group (P = 0.01). There were no significant differences in liver function, renal function, the C-reactive protein level, the white blood cell count, or the red blood cell count (Table 2).
Comparison of preoperative and postoperative laboratory tests.
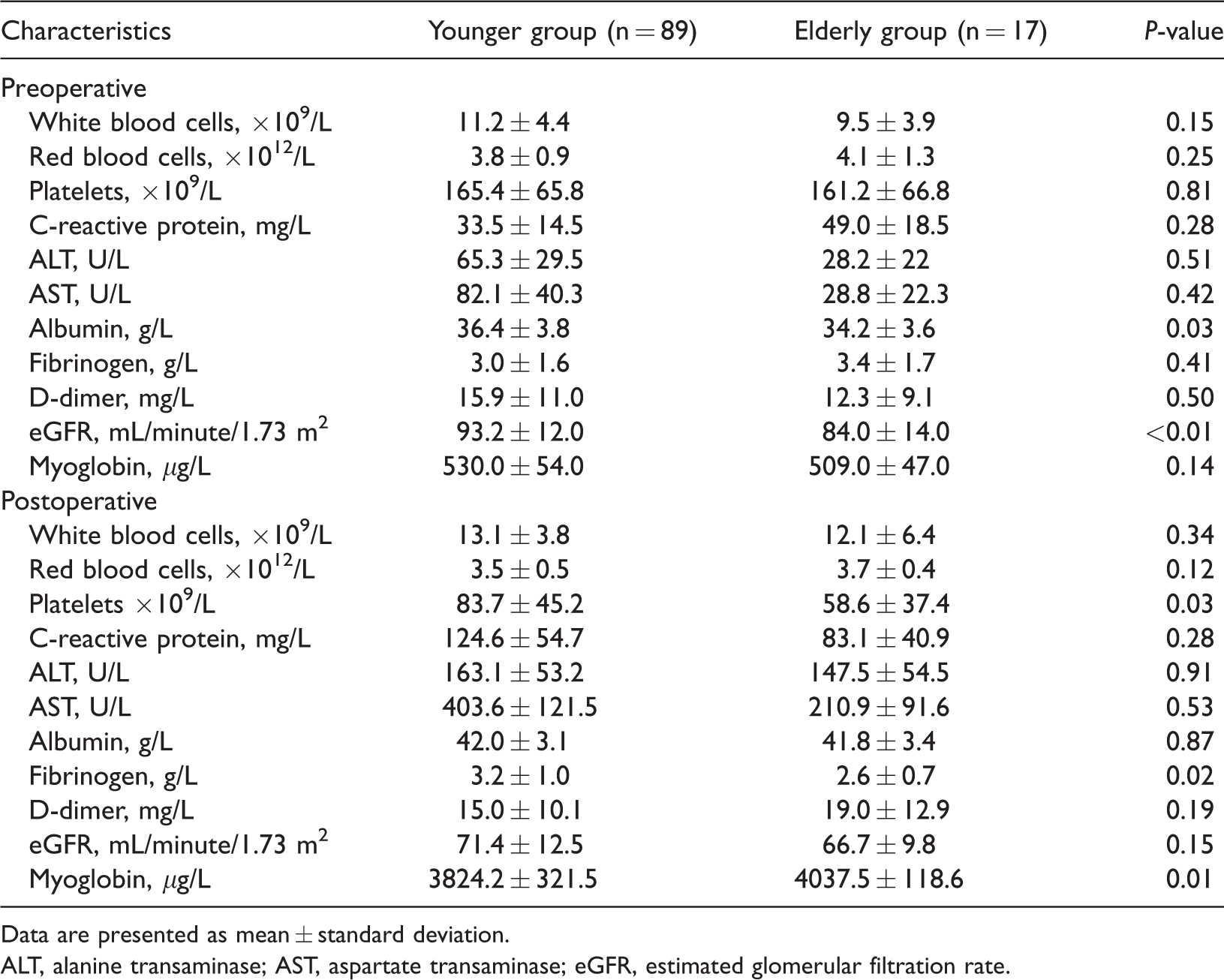
Data are presented as mean ± standard deviation.
ALT, alanine transaminase; AST, aspartate transaminase; eGFR, estimated glomerular filtration rate.
The aortic root operations included the Bentall procedure, David procedure, and ascending aorta replacement with no significant differences between the two groups. Concomitant surgeries, including right coronary artery bypass grafting and aortofemoral bypass, were more frequently performed in the elderly group but with no significant differences. Intraoperative blood loss was higher in the elderly group than in the younger group (337.3 ± 85.4 vs. 407.3 ± 77.4 mL, respectively; P = 0.002). The intraoperative CPB time, aortic cross-clamping time, and DHCA time were comparable between the two groups (Table 3).
Intraoperative data.
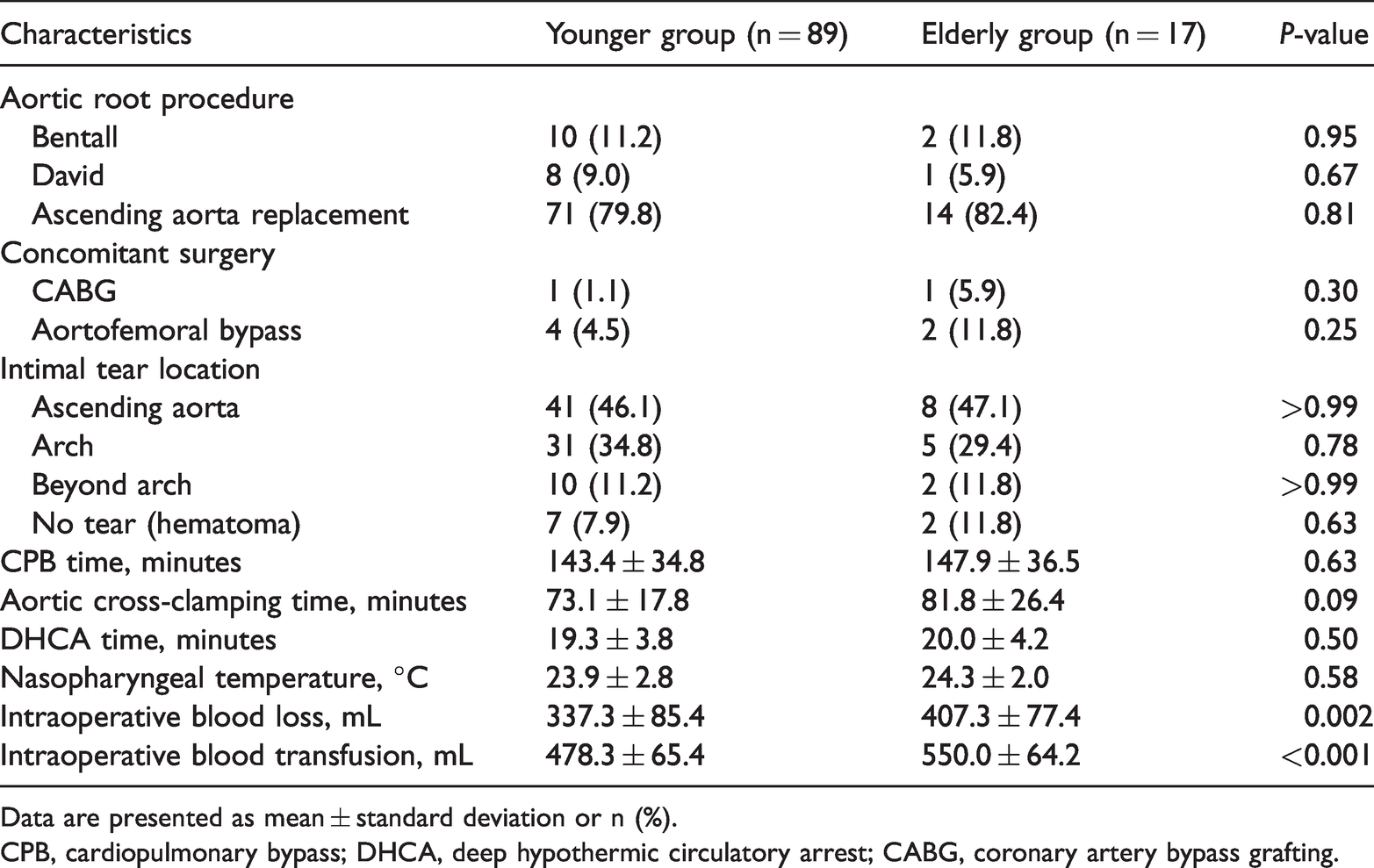
Data are presented as mean ± standard deviation or n (%).
CPB, cardiopulmonary bypass; DHCA, deep hypothermic circulatory arrest; CABG, coronary artery bypass grafting.
Postoperative recovery, including the length of hospital stay, ventilation time, and length of intensive care unit stay, was comparable between the two groups. No significant differences in postoperative complications were noted except for a higher incidence of sepsis in the elderly group (Table 4). The in-hospital mortality rate was satisfactory in the elderly group and only slightly higher than that in the younger group (17.6% vs. 15.7%, respectively). The 30-day mortality rate was also similar between the two groups.
Postoperative data and outcomes.

Data are presented as mean ± standard deviation or n (%).
ICU, intensive care unit; CRRT, continuous renal replacement therapy.
Discussion
Data from the German Registry for Acute Aortic Dissection Type A (GERAADA) and the International Registry of Acute Aortic Dissection (IRAD) showed that about 30% of patients were ≥70 years of age,14,15 whereas data from a Chinese registry (Sino-RAD) revealed that only 6.5% of the population was >70 years of age. One reason for this difference may be that in some rural places in China, patients died before admission or refused to accept surgery because of high surgical risks and financial problems. 16 Another important reason may be physicians’ attitudes, which was relatively conservative in terms of recommending surgery for elderly patients in the early stage of treating aortic dissection. Additionally, with the advanced aging of the population and increasing global life expectancy, cardiac surgeons are being faced with increasing numbers of elderly patients.
Emergency life-saving surgical intervention is still associated with high in-hospital mortality possibly because of surgical complexity and preoperative hemodynamic compromise. When confronted with an elderly patient with ATAAD, a cardiac surgeon may face an ethical dilemma regarding whether it is appropriate to deny offering life-saving surgery based solely on advanced age.9,17 Study results have been inconsistent with respect to the best surgical strategy for ATAAD in elderly patients.18–20 In the present study, we compared the postoperative outcomes of 106 consecutive patients with ATAAD who underwent an emergency Sun’s procedure, focusing on the role of age in the outcome of aggressive total arch replacement. No difference in in-hospital mortality or postoperative complications was found between the two groups.
Is surgical therapy justified in elderly patients with ATAAD?
Increased age has been shown to be a strong independent predictor of in-hospital mortality associated with cardiovascular treatments, including surgical and medical therapy.21,22 For elderly patients with ATAAD, the risks of surgery should outweigh the risk of death from medical treatment.
Trimarchi et al. 23 revealed that although surgical mortality increased with advancing age, patients treated surgically had significantly lower in-hospital mortality than patients treated medically (23.8% vs. 59.3%, respectively) in all age groups. The authors also concluded that an age of ≥70 years was an independent predictor of in-hospital mortality (38.2% vs. 26.0%). 23 Beckmann et al. 10 also found that among patients with ATAAD, the in-hospital mortality rate was 50% higher in those aged >70 years than in those aged <70 years. However, the surgical mortality rate was still lower in surgically treated patients aged >70 years than in medically treated patients (37.5% vs. 52.5%, respectively). Moreover, postoperative complications were similar in the two groups. Therefore, to improve survival, an aggressive surgical approach is not considered unreasonable in select elderly patients with ATAAD. In the present limited experience, we found no significant difference in in-hospital mortality between the younger and elderly groups (15.7% vs. 17.6%, respectively).
Based on the above findings, we are inclined to believe that age alone should not be used as a sole criterion by which to exclude patients from surgical treatment for ATAAD. Cardiovascular surgeons can be more active in recommending surgical options for elderly patients without contraindications.
Optimal treatment of the aortic arch: limited or total repair?
Management of the aortic arch in elderly patients with ATAAD has long been a topic of debate.24,25
Qin et al. 26 compared the short- and mid-term results between the limited aortic repair group (ascending and/or hemi-arch replacement) and extended-arch repair group (ascending arch and proximal descending aortic replacement) in ≥65-year-old patients with ATAAD. They found that the extended-arch repair group had higher in-hospital mortality than the limited aortic repair group, whereas there was no significant difference in the 5-year survival rate between the two groups. However, the authors considered that the results may have been compromised by the small number of patients in each group. Zhu et al. 27 analyzed their Stanford experience in the management of ATAAD with hemiarch and total arch replacement from 2000 to 2019 and found no difference in survival or distal aortic reoperation, which is consistent with previous studies. 28 The underlying rationale for total arch replacement is to avoid leaving any intimal tear in the aortic arch and to resolve malperfusion of arch branch vessels with the goal of preventing future rupture of the diseased aorta and stroke. Most aortic surgeons now agree that it is logical to recommend total arch replacement for patients with the highest theoretical benefit, such as younger patients and those with Marfan syndrome or other connective tissue disorders. However, more convincing evidence is needed to identify patients who will benefit the most from aggressive total arch replacement.
In our center, Sun’s procedure is indicated in patients with ATAAD with the primary entry located in the arch and descending aorta, in those with involvement of the arch vessels, and in those with Marfan syndrome. If the patient is not of advanced age (>90 years) and has no severe comorbidities, we are inclined to recommend surgery after a thorough discussion of all risks and benefits with the whole family. This is especially important in developing countries where medical insurance is ready for every patient. The DHCA time in Sun’s procedure is about 20 minutes, which is considered a safe period of circulatory arrest. Near-infrared reflectance spectroscopy is routinely used intraoperatively to monitor regional cerebral oxygenation.
In the present study, although intraoperative blood transfusion was more frequently performed in elderly patients than in younger patients possibly because of difficult hemostasis in elderly patients, there was no significant difference in early postoperative complications such as stroke, renal failure, or paraplegia. A multidisciplinary care team including respiratory therapists, physical therapists, and cardiac intensive care unit nurses is responsible for postoperative recovery. Our goal for each elderly patient with ATAAD is survival with good quality of life. Therefore, seasoned surgical judgment is of paramount importance and must be exercised before surgery.
This study had some limitations. It was a single-center retrospective review and was limited by the relatively small number of patients treated in just 1 year in our center. However, most aspects of our treatment protocol were standardized, and the results may be more convincing than those in previous studies. Selection bias was also present in our study, such as that arising from the exclusion of patients with end-stage liver disease and a low left ventricular ejection fraction, which might have resulted in the exclusion of some truly difficult cases. Furthermore, only early in-hospital outcomes were analyzed; investigation of long-term outcomes is needed in future studies.
In summary, emergency performance of Sun’s procedure for patients with ATAAD characterized by an entry tear in the aortic arch or involvement of the supra-aortic vessels should not be denied on the basis of advanced age alone. Compared with young patients, similar early in-hospital outcomes can be achieved in elderly patients by judicious preoperative selection and multidisciplinary postoperative care. Further research is needed to evaluate management strategies that would improve long-term survival in this high-risk patient subset.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221109377 - Supplemental material for Early outcomes of Sun’s procedure in elderly patients with acute aortic dissection: a single-center retrospective study
Supplemental material, sj-pdf-1-imr-10.1177_03000605221109377 for Early outcomes of Sun’s procedure in elderly patients with acute aortic dissection: a single-center retrospective study by Liang Zhong, Hongyan Xiong, Jing Li, Yong He and Heping Zhou in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Natural Science Basic Research Program of Shaanxi (No. 2022JM-573).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.