
Abstract
Objective
We aimed to evaluate the mid-term efficacy of tension-free vaginal mesh (TVM) for pelvic organ prolapse (POP), and observe the time course of lower urinary tract symptoms and sexual function.
Methods
In this retrospective study, we included 112 female patients who underwent TVM at a single center for stage 2 or higher POP, and replied to questionnaires before, and 2 and 4 years after TVM. We evaluated the anatomical cure rate, prolapse quality of life questionnaire scores, international prostate symptom scores, International Consultation on Incontinence Questionnaire-Short Form scores, and Female Sexual Function Index scores.
Results
The anatomical cure rate at 4 years was 89%. Voiding and storage symptoms improved in patients after TVM. We found that 25/112 patients had sexual intercourse before TVM, and among them, 15/25 (60%) continued sexual intercourse after TVM. Additionally, of the 87 patients who had no sexual intercourse before TVM, 13 resumed sexual intercourse after TVM.
Conclusion
Cases of TVM have decreased because of the Food and Drug Administration statements concerning mesh problems. However, this study showed relatively favorable mid-term results for lower urinary tract symptoms. Furthermore, sexual activity was restored in some patients, indicating the efficacy of TVM for sexual function.
Keywords
Introduction
The female pelvic floor consists of muscles, ligaments, connective tissues, and nerves that support the structure and function of the bladder, uterus, vagina, and rectum. Pelvic floor disorders are classified into the three main types of urinary incontinence, fecal incontinence, and pelvic organ prolapse (POP). According to studies using National Health and Nutrition Examination Survey data, approximately 25% of women in the USA have at least one pelvic floor disorder.1,2
POP is defined as pelvic organs moving out of place in the pelvis, resulting in their herniation through the vagina or anus. The etiology of POP is assumed to be a combination of genetic and environmental risk factors. POP is mainly caused by distinctive fascial defects that arise owing to vaginal childbirth or aging.2,3 In addition to vaginal discomfort, POP also causes urinary and sexual dysfunction.4,5 POP is generally not life-threatening, but it represents a considerable public health burden because it is associated with a decreased quality of life. 6 The incidence of POP increases with age, and the lifetime risk until 85 years when surgical treatment is required for POP is 20.5%. 7 POP often requires surgical treatment. 8 Tension-free vaginal mesh (TVM) surgery, involving the implantation of synthetic (polypropylene) mesh in areas of vesicovaginal and rectovaginal dissection, used to be relatively common. 9
We previously found favorable short-term results for TVM with concomitant mid-urethral slings for POP with stress urinary incontinence (SUI). 10 However, this study did not show any effects on sexual function. Furthermore, the Food and Drug Administration (FDA) issued safety notifications regarding vaginal mesh products in 2008 and 2010.
Since the FDA removed all transvaginal mesh products from the market, the number of new TVM cases has greatly decreased. However, there are still many mid- or long-term TVM cases. Therefore, evaluating the mid-term clinical results of TVM surgery is vital to determine the importance of follow-up in these cases. This study retrospectively studied lower urinary tract symptoms (LUTSs) and sexual function in patients with POP to evaluate the mid-term clinical efficacy of TVM surgery.
Materials and methods
The reporting of this study conforms to the STROBE guidelines. 11 This was a retrospective study that involved a cohort of patients with POP who were partly included in our previous report regarding the outcomes 1 year after TVM surgery. 10 Exclusion criteria included a previous history of POP treatment, an apparent neurogenic bladder, such as in cases with a history of diseases affecting the nervous system (e.g., diabetes or stroke), the presence of severe complications, urogenital malignancy, and dropout during follow-up. Patients with POP for ≥2 years who underwent TVM between March 2006 and February 2010 were eligible for and participated in the study. All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee at which the studies were conducted and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Institutional Review Board and Research Ethics Committee of Nihon University School of Medicine (RK-190611-3). Written informed consent was obtained from all individual participants included in the study.
The detailed surgical procedure has been described previously. 9 All patients had stage 2 or higher POP based on the POP quantification (POP-Q) system, 12 and there were 21, 54, and 37 patients with stages 2, 3, and 4, respectively (Table 1). Almost all patients (111/112) had cystocele, 12 had uterine prolapse, and 52 had rectocele. After obtaining written informed consent for surgery and participation in this study, anterior TVM repair was performed in 89 patients with cystocele, posterior TVM in 1 patient with rectocele, anterior/posterior TVM in 15 patients with prolapse of the apical compartment, and total TVM in 7 patients with vaginal vault prolapse. Ninety patients with concurrent SUI (80% of all cases) underwent concomitant transobturator tape or transvaginal tape sling procedures (Table 1). SUI was confirmed using the pad test or stress test.
Patients’ characteristics and preoperative assessments (n = 112).

SD, standard deviation; POP-Q, pelvic organ prolapse quantification; A, anterior; TVM, tension-free vaginal mesh; P, posterior; AP, anterior and posterior.
We evaluated the anatomical cure rate and the ratio of the number of patients with stage 0 prolapse on the basis of the POP-Q system, as previously described.9,13 To evaluate the prolapse quality of life (P-QOL) questionairre14,15 and LUTSs in POP cases, international prostate symptom scores (IPSSs), IPSS-quality of life (QOL) scores, International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) scores, 16 and the overactive bladder questionnaire (OAB-q) were analyzed as subjective parameters. The Female Sexual Function Index (FSFI) was used to evaluate sexual function. 17 The parameters of each patient were systematically assessed before, and at 2 and 4 years after TVM surgery.
To statistically analyze the results, we used a one-way analysis of variance with Dunnett’s multiple comparisons test to compare preoperative parameters. Statistical significance was set at p < 0.05. Analyses were performed using GraphPad Prism for Mac version 6 (GraphPad Software, Inc., La Jolla, CA, USA) and JMP® version 9 (SAS Institute Japan, Inc., Tokyo, Japan).
Results
We included 112 patients in the study. The patients’ characteristics are shown in Table 1. The anatomical cure rate (the number of cases with POP-Q stage 0 ÷ total cases) at approximately 4 years was 89%. Five patients had relapse and subsequent additional surgical treatment, four had mesh erosion, and two had considerable postoperative bleeding requiring readmission during this period. Notably, mesh-removal surgery due to mesh erosion was performed in three of four patients. All P-QOL score domains, including general health perception, the effect of prolapse, and social limitations, which comprised physical limitations, personal relationships, emotions, sleep/energy, and severity measures, were significantly improved 2 years after TVM surgery and were maintained at 4 years (all p < 0.0001, Figure 1).
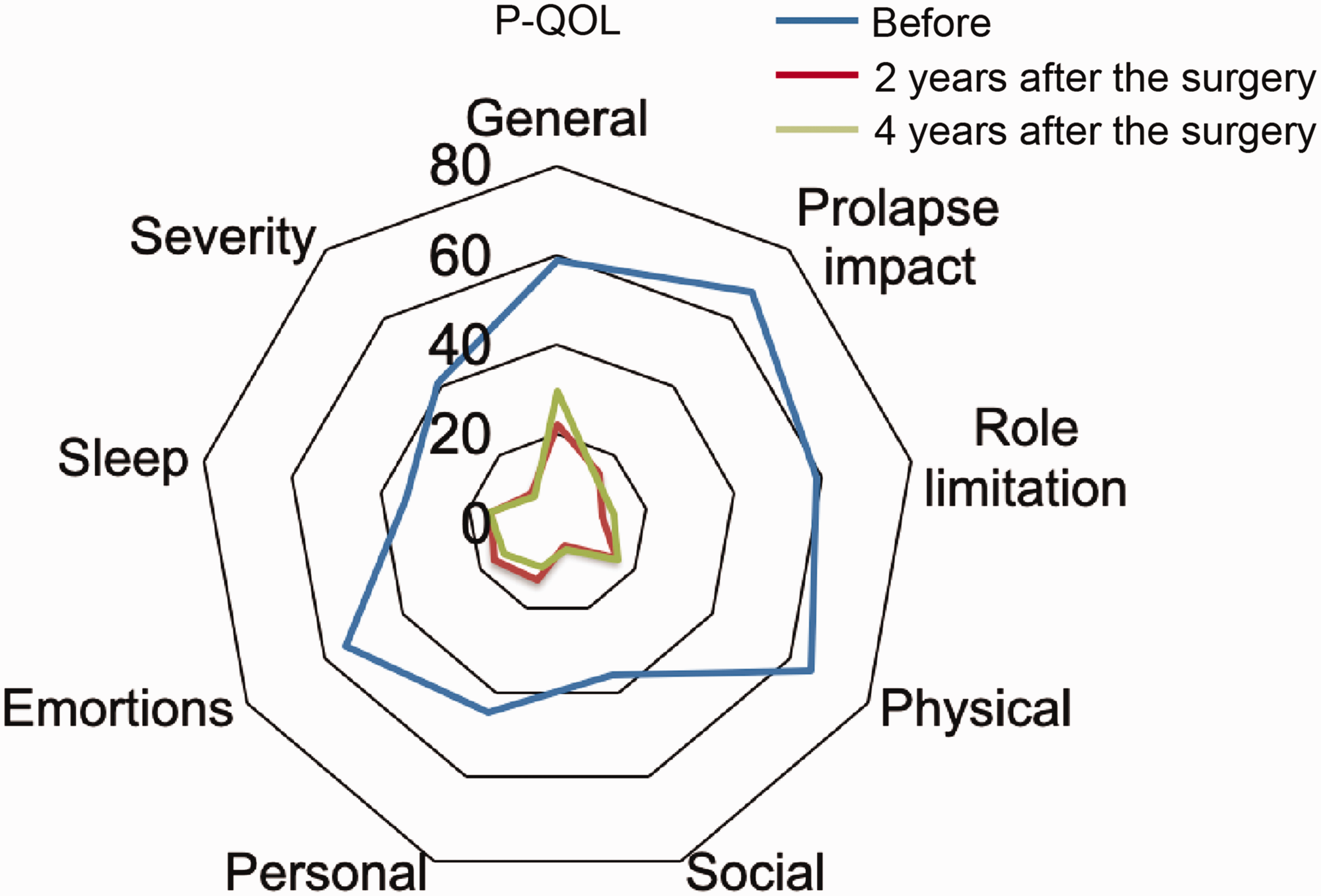
Evaluation of P-QOL questionnaire scores before and after tension-free vaginal mesh surgery (n = 112). All domains were significantly improved, and this improvement was maintained for 4 years (all domains; p < 0.0001).
Voiding and storage symptoms were measured using the IPSS. All IPSS sub-scores were significantly improved by 4 years following TVM surgery (Figure 2a and b, all p < 0.05 vs. before TVM surgery). Similar to the IPSS scores, all patients’ ICIQ-SF domains and OAB-q scores were significantly improved by 4 years (Figure 2d, all p < 0.0001). There were no significant changes in the FSFI domains between before and 2 years after TVM surgery. However, all domains, except for pain, were significantly deteriorated at 4 years (Figure 3, all p < 0.05 vs. the preoperative score). We found that 10/25 patients who were sexually active before TVM surgery stopped being sexually active postoperatively (stopped group). Additionally, 13 who were not sexually active before surgery became sexually active after the surgery (resumed group, Table 2). The number of patients with a younger age, lower POP stage, and no surgical complications, especially mesh erosion, was significantly higher in the resumed group than in the stopped group (Table 2, all p < 0.05).
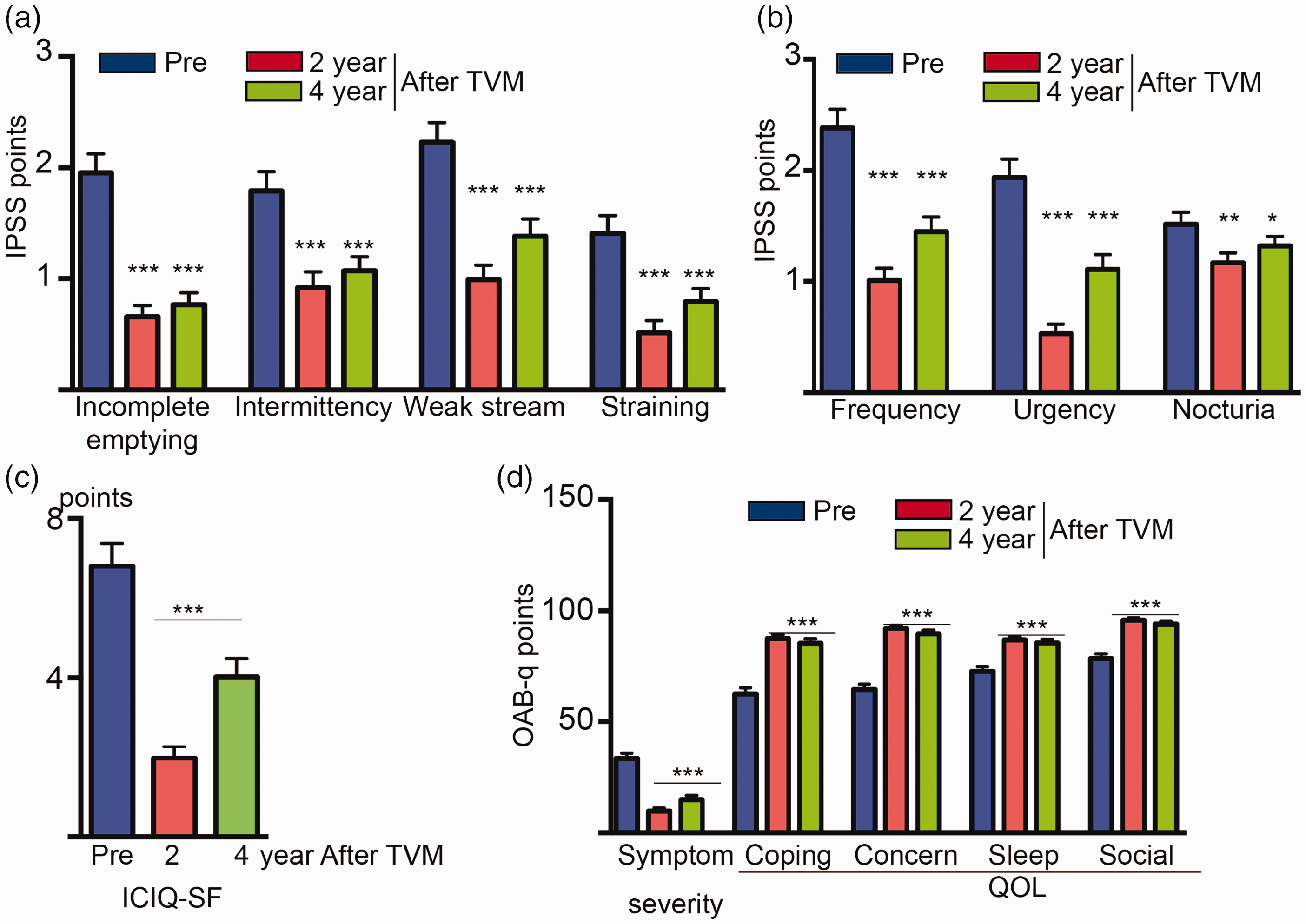
Changes in voiding (a) and storage symptoms (b) of IPSS domains after TVM surgery. All IPPS domains were significantly improved. (c) Changes in the ICIQ-SF score after TVM. Although the ICIQ-SF score was slightly deteriorated at 4 years, it significantly improved after TVM surgery and (d) All OAB-q domains were significantly improved at 4 years after TVM surgery. Only the symptom severity domain indicated that higher score values represented greater symptom severity or discomfort, and lower scores indicated minimal symptom severity.

FSFI scores were obtained from all patients before and after TVM surgery.
Comparison between patients who stopped and those who resumed sexual intercourse after surgery.

“Stopped” indicates patients who stopped having intercourse after TVM surgery.
POP-Q, pelvic organ prolapse quantification; A, anterior; TVM, tension-free vaginal mesh; AP, anterior and posterior; SUI, stress urinary incontinence.
Discussion
TVM surgery gained popularity in 2005 because of the low recurrence rate compared with traditional non-mesh repair surgery. While the recurrence rate for traditional anterior or posterior repair is 30%, TVM has a 10% recurrence rate.18–20 However, recent multicenter, randomized, controlled trials (PROSPECT) showed that >1/10 women with TVM had a mesh complication, and there was no difference in QOL-related outcomes between TVM and non-mesh repair after approximately 2 years. 21 PROSPECT was a rigorous study that provided strong clinically relevant evidence for the unfavorable effects of mesh surgery in terms of improving POP symptoms. However, some small studies showed that recurrence and complication rates of TVM were lower than those of PROSPECT.20,22 The observation periods in these studies were shorter than 3 years postoperatively, which indicates that a study with a longer follow-up period is required to further evaluate TVM.
This study evaluated urinary symptoms using the IPSS, OAB-q, and ICIQ-SF. Initially, the IPSS was used to evaluate LUTSs in men with benign prostatic hyperplasia. However, some reports, including our previous study, showed that this questionnaire was also useful for the evaluation of female LUTSs.10,23–25 Additionally, the IPSS has shown excellent internal consistency and good configural validity in the evaluation of female LUTSs. 23 We used the IPSS in this study because it is recommended as a tool to evaluate female LUTSs in the Clinical Guidelines for Female Lower Urinary Tract Symptoms.26 We found favorable results regarding urinary symptoms 4 years postoperatively. Notably, a recent report showed that the cure rate of transvaginal wall sling surgery for SUI significantly declined 5 years postoperatively. 27 However, this report was based on treatment outcomes for cases of SUI, and the effects of POP and TVM were not evaluated. In our study, 80% of patients were treated with TVM concomitant with the vaginal wall sling for SUI and POP. These data suggest the importance of further, longer-term evaluation of TVM concomitant with vaginal wall slings. Palma et al. recently reported the efficacy of TVM in a 2-year follow-up. 28 Although they showed a favorable anatomical cure rate and improvement in urinary incontinence after TVM surgery, they did not analyze voiding symptoms. In addition to our previous study, which showed that POP affected voiding and storage urinary symptoms, 10 the present study showed the mid-term efficacy of TVM in improving these symptoms using multiparametric questionnaires.
With regard to sexual function, we observed a slight improvement in the FSFI 2 years after TVM surgery, followed by a significant deterioration at 4 years, which might have been affected by aging-related factors. Ratner et al. reviewed the effect of aging on sexual activity, 29 and their findings are consistent with our study. They also found that the number of sexually inactive older women was twice that of sexually inactive men of the same age. 29 Additionally, racial factors may have affected this deterioration. There is only one report on sexual function in Japanese patients with POP. Recently, Kinjo et al. reported similar results to our study using the FSFI and P-QOL regarding the short-term efficacy of TVM. 15 They found that only 14% of Japanese patients with POP were sexually active, and FSFI scores did not change after TVM. 15 Although they did not evaluate the FSFI in healthy control cases, they found that Japanese women showed the lowest frequency of sexual intercourse among women from 41 Western and Asian countries. 15 They also found that six patients withdrew from sexual intercourse, but five patients resumed sexual activity 1 year postoperatively. 15 In this study, we found that 10 women stopped sexual intercourse and 13 resumed sexual intercourse (Table 2). We suggest that surgery-related complications, such as mesh erosion and bleeding, are important factors affecting sexual activity after TVM surgery.
Interestingly, most patients in the resumed group restarted sexual intercourse more than 2 years after TVM surgery (data not shown). These data suggested that although there was no significant overall improvement before and after TVM surgery, some patients in whom potential sexual activity was suppressed owing to POP were able to achieve long-term improvement with TVM.
In conclusion, TVM surgery improves LUTSs for at least 4 years. Mesh-related complications have a significant long-term effect on the deterioration of sexual function. Although we previously reported that the total cost of TVM surgery was significantly lower than that of laparoscopic sacrocolpopexy according to the Japanese national database, 30 long-term follow-up is required for TVM cases with mesh-related complications.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221106434 - Supplemental material for Tension-free vaginal mesh for patients with pelvic organ prolapse: mid-term functional outcomes
Supplemental material, sj-pdf-1-imr-10.1177_03000605221106434 for Tension-free vaginal mesh for patients with pelvic organ prolapse: mid-term functional outcomes by Daisuke Obinata, Kenya Yamaguchi, Sho Hashimoto, Tsuyoshi Yoshizawa, Junichi Mochida and Satoru Takahashi in Journal of International Medical Research
Footnotes
Acknowledgments
Author contributions
Conception: DO, KY, and ST; design of the study: DO; acquisition and analysis of data: JM, SH, and TY; interpretation of data: DO, KY, and ST; and writing the first draft of the manuscript: DO. All authors agreed with manuscript’s results and conclusions. All authors reviewed and approved the final manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.