
Abstract
Objective
May–Thurner syndrome (MTS) is an anatomic stenotic variation associated with deep vein thrombosis (DVT) of the left leg. The classical DVT treatment strategy is medical treatment without thrombus removal. This study was performed to assess the clinical outcomes of the combination of AngioJet™ rheolytic thrombectomy and stenting for treatment of MTS-related DVT.
Methods
We conducted a retrospective cohort study of patients treated for MTS-related DVT from January 2017 to June 2020 at a single institution.
Results
Fourteen patients (nine women) underwent AngioJet™ rheolytic thrombectomy for MTS-related DVT during the study period. The median DVT onset time was 8 days (interquartile range (IQR), 3–21 days). The median procedure time was 130 minutes (IQR, 91–189 minutes), and the median hospital stay was 7 days (IQR, 5–26 days). One patient had a residual thrombus and occluded iliac stent and underwent adjuvant catheter-directed thrombolysis for revascularization. The primary patency rate for the iliac stent was 92.9% at 12 months.
Conclusion
Concomitant AngioJet™ rheolytic thrombectomy and stenting of MTS-induced lesions may be beneficial for patients with MTS-related DVT.
Keywords
Introduction
May–Thurner syndrome (MTS), an anatomic stenotic variation first described by May and Thurner, 1 is characterized by symptoms in the left leg resulting from compression of the left common iliac vein (CIV) between the right common iliac artery (anteriorly) and the vertebral body of the fifth lumbar vertebra (posteriorly). 2 This anatomic variation is associated with the onset of symptomatic acute deep vein thrombosis (DVT) of the left leg. 3 Diagnosing and treating MTS is therefore important to prevent multiple DVT and ultimately post-thrombotic syndrome (PTS). 4
The standard classical treatment strategy for DVT is medical treatment with anticoagulant agents, the aim of which is to prevent the lethal complication of pulmonary embolism (PE) and recurrent DVT. 5 Anticoagulants are employed to prevent thrombosis progression rather than to remove the thrombosis. With the advent of minimally invasive surgery, endovascular treatments including catheter-direct thrombolysis (CDT) and stent placement have been applied to the treatment of MTS and DVT.4,6 Although thrombolysis increases the patency of veins and reduces the incidence of PTS, bleeding complications limit the treatment’s applicability. 5
AngioJet™ rheolytic thrombectomy combines thrombolytic drugs and mechanical thrombectomy, thereby reducing the dose of thrombolytic agents and the risk of bleeding. This study was performed to assess the clinical outcome of the combination of AngioJet™ rheolytic thrombectomy and stenting for the treatment of MTS-related DVT.
Materials and methods
Patients and study design
This retrospective cohort study was approved by the institutional review board of Chang Gung Memorial Hospital in Taoyuan, Taiwan (Approval No. 202001575B0). Because this was a retrospective cohort study, the need for individual informed consent was waived. The reporting of this study conforms to the STROBE guidelines. 7
We reviewed the electronic medical records, medical history, imaging findings, and laboratory data of consecutive patients with leg DVT treated with AngioJet™ rheolytic thrombectomy at our center from January 2017 to June 2020. All patient details were de-identified during data collection. We employed the ZelanteDVT™ catheter (AngioJet™ venous catheter) for the venous procedures in accordance with the manufacturer’s instructions. We confirmed the diagnosis of leg DVT by the clinical signs and symptoms and the duplex ultrasound or computed tomographic venography (CTV) images. The diagnostic criteria for MTS-related DVT were as follows: (1) >50% compression of the left CIV by the right common iliac artery and fifth lumbar vertebral body in the transverse view of computed tomography (Figure 1); (2) accumulation of thrombus burden from the distal part of the left leg (including the popliteal vein, superficial femoral vein, common femoral vein, external iliac vein, and CIV) to the impinged vein area (Figure 2); (3) multiplanar venography after AngioJet™ rheolytic thrombectomy showing a stenotic lesion at the MTS-impinged vein and focal left CIV stenosis with the collateral vein; and (4) balloon waist noted in pre-dilation angioplasty before stenting under fluoroscopy during the procedure.

Fifty percent compression of the left common iliac vein by the right common iliac artery and fifth lumbar vertebral body in the transverse view of computed tomography (arrow).

Accumulation of thrombus burden in the left iliac vein (arrowhead).
Procedure
All procedures were performed with the involvement of at least one vascular surgeon and one interventional radiologist. The patient’s position during the operation and the access site were chosen by the operators according to the preoperative CTV images.
Inferior vena cava filter
The operators decided whether to implant a retrievable inferior vena cava (IVC) filter based on the risk of dislodging massive thrombi from the DVT of the iliofemoral vein, resulting in PE. Vascular access for IVC filter implantation was from the right internal jugular vein or patent contralateral common femoral vein under real-time echo-guided venipuncture. During the IVC filter implantation, all patients were positioned supine under local anesthesia.
AngioJet™ rheolytic thrombectomy
The ipsilateral leg vein was punctured under ultrasound guidance (BD/Bard Site Rite 5; BD/Bard, Franklin Lakes, NJ, USA). Following venous access with an 8-French sheath in place, we first performed pre-procedure venography to evaluate the degree of thrombus and the burden of the left leg. An 8-French AngioJet™ DVT thrombectomy infusion catheter (ZelanteDVT™ catheter; Boston Scientific, Marlborough, MA, USA) was inserted using an over-the-wire technique into the most proximal part of the thrombus. We then infused the diluted thrombolytic agent urokinase (250,000 U) (Green Cross Corporation Co., Ltd., Gyeonggi-do, Korea) under the power-pulsed mode of the AngioJet™ catheter to deliver the drug directly and evenly into the thrombus if there were no absolute or relative contraindications. We then waited for 15 to 20 minutes to allow the thrombolytic agent to work. We performed percutaneous mechanical thrombectomy (PMT) using the thrombectomy mode of the AngioJet™ from the most proximal part of the thrombus in the CIV to the distal part of the thrombus. Venography was performed through an introducer sheath or an AngioJet™ rheolytic thrombectomy catheter. If the venography revealed residual thrombi, we repeated the AngioJet™ rheolytic thrombectomy procedure, focusing on the residual thrombi until all retrievable thrombi were removed or the recommended PMT duration had elapsed (≤480 s) in accordance with the manufacturer’s instructions for use.
Stenting
After AngioJet™ rheolytic thrombectomy, we confirmed the MTS anatomical stenotic lesion using intraoperative multiplanar venography. The exact location of the MTS anatomical stenotic lesion was identified by the balloon waist during the pre-dilatation angioplasty (Figure 3(b)). We chose the appropriate stent size according to the size of the healthy veins proximal and distal to the lesions. We deployed the self-expanding stent with proximal extension into the IVC without touching the contralateral side of the IVC wall to sufficiently cover the stenotic lesion and not compromise the venous outflow in the contralateral leg (Figure 3(c)). The distal end of the stent was extended at least 1 cm from the healthy venous landing zone distal to the MTS stenotic lesion (Figure 3(d)). The stents available at our center are the Wallstent™ (Boston Scientific) and the Venovo™ venous stent (BD/Bard), and they were selected at the physician’s discretion.

(a) A 0.035-inch guidewire (0.035 Radiofocus® Guidewire M; Terumo Corp., Somerset, NJ, USA) was advanced to the inferior vena cava. (b) The exact position of the May–Thurner syndrome-related anatomical stenotic lesion was identified by the balloon waist during pre-dilatation angioplasty. (c) A self-expanding stent was deployed with proximal extension into the inferior vena cava without touching the contralateral side of the inferior vena cava wall to sufficiently cover the stenotic lesion and not compromise the venous outflow in the contralateral leg and (d) The distal end of the stent was extended at least 1 cm into the healthy normal venous landing zone distal to the May–Thurner syndrome-related stenotic lesion.
After the procedure, the introducer sheath was removed and the vascular access wound was sutured with 4-0 monofilament nonabsorbable Prolene sutures or was simply manually compressed until total hemostasis was achieved.
Postoperative care
After the operation, the patients were prescribed low-molecular-weight heparin or novel oral anticoagulants immediately after the procedure, and sufficient intravenous hydration was ensured. The patients were encouraged to ambulate 2 hours after the procedure and wear grade II compressive stockings as early as possible. After discharge, the patients were prescribed novel oral anticoagulants and the heparin was discontinued.
Follow-up
The clinical condition of the affected limb was evaluated at 1, 3, 5, and 12 months postoperatively. The patients thereafter made yearly visits to the vascular surgeons’ or interventional radiologists’ follow-up clinics, where the stents were examined under duplex ultrasound or computed tomography. The clinical condition of the leg was evaluated and recorded in the electronic medical record as no improvement or improvement, based on the patient’s feedback.
Statistical analysis
Data were collected using Microsoft Excel (Microsoft Corp., Redmond, WA, USA), and all analyses were conducted using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA). Descriptive data are expressed as median (interquartile range (IQR)) for continuous variables, and categorical variables are expressed as numbers. The primary patency of the stent in the affected vein was calculated using the Kaplan–Meier method.
Results
During the study period, 14 patients underwent AngioJet™ rheolytic thrombectomy to treat MTS-related DVT (9 women and 5 men). Table 1 shows the patients’ demographics. The patients’ median age was 58 years (IQR, 50–76 years). Their underlying diseases included hypertension in four patients, malignancy in four, diabetes mellitus in three, smoking in two, peripheral artery disease in one, stroke in one, dyslipidemia in one, and chronic obstructive pulmonary disease in one.
Demographic data, clinical findings, and clinical outcomes of patients with MTS-related DVT.
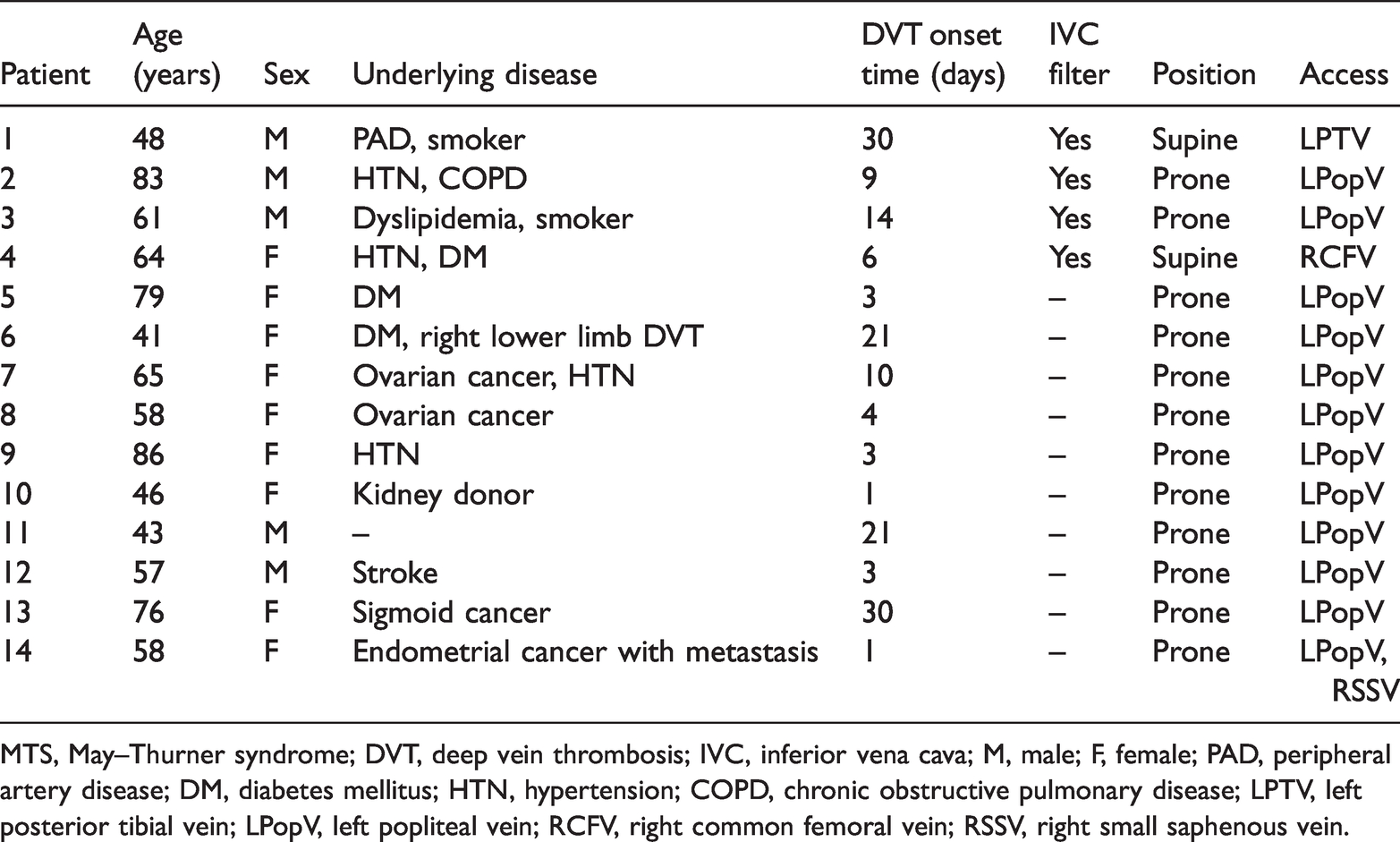
MTS, May–Thurner syndrome; DVT, deep vein thrombosis; IVC, inferior vena cava; M, male; F, female; PAD, peripheral artery disease; DM, diabetes mellitus; HTN, hypertension; COPD, chronic obstructive pulmonary disease; LPTV, left posterior tibial vein; LPopV, left popliteal vein; RCFV, right common femoral vein; RSSV, right small saphenous vein.
The median DVT onset time was 8 days (IQR, 3–21 days), and four patients developed subacute DVT (≥21 days). The first four patients underwent implantation of an IVC filter before the AngioJet™ rheolytic thrombectomy. Two patients had organized thrombi in the superficial femoral vein and underwent adjuvant percutaneous transluminal angioplasty for thrombi maceration. The median procedure time was 130 minutes (IQR, 91–189 minutes).
The median hospital stay was 7 days (IQR, 5–26 days). Patient 1 had residual thrombi and an occluded iliac stent and underwent adjuvant CDT for revascularization during hospitalization. The stent was patent after the re-intervention. The primary patency rate for the iliac stents was 92.9% at 12 months.
Three IVC filters were removed before discharge, and no thrombi were captured in the IVC filter net (as observed by venography) during the IVC retrieval procedure. Patient 3 underwent filter removal 5 months after the operation because of residual thrombi after iliac stenting. Because the stent was patent and the patient had no signs or symptoms, no further intervention was performed. No patients developed major or minor bleeding, and none presented signs or symptoms of PE during or after the procedures.
Discussion
DVT is a common but elusive venous disease that can lead to lethal complications such as PE. 8 According to the guidelines of the European Society of Cardiology, anticoagulant medical treatment is an option for either initial or long-term treatment if there are no contraindications. 9 Despite adequate anticoagulation therapy after DVT, however, 20% to 50% of patients develop PTS,10,11 which is incurable and associated with a significantly impaired quality of life. 12
According to a study by Alesh et al., 13 early thrombus removal by CDT is beneficial in decreasing the risk of PTS and bleeding complications compared with systemic thrombolysis in treating DVT. However, bleeding complications are still the major concern in CDT. 5
By employing Bernoulli’s principle, the AngioJet™ rheolytic thrombectomy device actively removes and suctions fragmented thrombi using power-pulse thrombolysis via a small catheter. The device is an alternative advanced modality that can decrease the dosage of thrombolytic agents and reduce the risk of major bleeding complications inherent in CDT. 14 In this study, we applied AngioJet™ rheolytic thrombectomy to successfully treat MTS-related DVT without bleeding complications. By performing urokinase injection with the power-pulse mode of the AngioJet™, we were able to successfully remove subacute thrombi from four patients. Only one patient (our first case) required a further adjuvant CDT procedure because of the relatively long thrombosis duration and our lack of familiarity with the procedure at that time.
According to Virchow’s triad, a major theory delineating the pathogenesis of venous thromboembolism, the disease will occur as a result of blood stasis. MTS is an uncommon anatomic variation that results from overcompression of the left CIV between the vertebral body of the fifth lumbar vertebra and the overlying right common iliac artery. Alternating blood flow in the left CIV in patients with MTS will induce recurrent DVT. However, MTS has been underestimated in the past and should always be suspected in the left leg of patients with DVT. 15 In patients with MTS-related DVT, it is essential to correct the underlying anatomic variation that can lead to the onset of DVT, thereby preventing DVT recurrence.
The current mainstream treatment for MTS after iliofemoral thrombi removal is endovascular treatment. The Active Stenting for May–Thurner Iliac Compression Syndrome registry reported the results of stent patency in 59 patients with MTS, with a primary patency rate of 84% at 19 months. 16 Goldman et al. 17 retrospectively reviewed 10 cases of stenting for MTS and found a 79% primary patency rate and 100% secondary patency rate at 12 months. Hager et al. 18 performed a retrospective review and analysis of 77 patients who underwent stenting for MTS and reported a 91% primary patency rate at 36 months. Several researchers have reported the results of PMT plus stenting in patients with acute iliofemoral DVT caused by MTS.19,20 Jiang et al. 20 reported a primary patency rate of 91.1% at 24 months. In the present study, we employed the AngioJet™ rheolytic thrombectomy device for thrombus removal and treated the MTS lesions concomitantly. The primary patency rate at 12 months was 92.9%, which is consistent with that of prior studies. No stent migration, fracture, or collapse was detected during follow-up, and none of our patients developed recurrent DVT.
The foundation of successful stenting is adequate assessment of the landing zones. Intravascular ultrasound provides important information using a small ultrasound probe with no risk of contrast medium-related nephropathy, allergy, or radiation exposure compared with venography. 4 However, intravascular ultrasound is not available at our center. We therefore assessed the MTS and landing zones for the stent through preoperative CTV and intraoperative multiplanar venography. In the preoperative CTV images, the left CIV was compressed between the right common iliac artery and the fifth lumbar vertebral body in the transverse view, and extensive distal iliofemoral thrombi were present. Intraoperative multiplanar venography showed that the stenotic MTS lesions had multiple collateral veins that were more proximal to the vein. By combining the CTV and multiplanar venography images, we were able to place the stent in such a manner as to precisely cover the lesion without touching the contralateral wall of the IVC and interfering with the right CIV flow.
To prevent stent collapse and migration, we did not place the stent exactly at the iliocaval confluence. The limitation of the current stent design is that the radial force of the bilateral stent edges is relatively weaker than that of the body. Prior studies have therefore recommended placing the stent so that it protrudes into the IVC.21,22 In a study by Khairy et al., 23 all the patients developed contralateral limb DVT following ipsilateral iliac stenting, which occurred only with complete coverage of the contralateral CIV. Our strategy for MTS stenting was therefore to stent the iliac with cava extension without touching the contralateral wall of the IVC to maintain bilateral CIV flow.
In the present study, we implanted IVC filters in the first four patients only to prevent PE. IVC filter implantation before CDT or PMT for acute iliofemoral DVT has been suggested for certain patients, such as those with preoperative clinical PE, those with multiple DVT risk factors, and women. 24 Considering its pathophysiology, MTS is characterized by chronic iliac artery pulsation that stimulates the underlying iliac vein’s interior vessel wall, producing “spur”-like tissue formation and then partially or totally obstructing the venous outflow, ultimately resulting in venous thrombosis. The MTS-related stenotic lesion acts as a natural barrier/filter in the venous lumen, and its narrow lumen induces venous thrombosis and indirectly prevents the bulky thrombus from accidently dislodging from the iliofemoral vein into the pulmonary artery. Jin et al. 25 found that patients with acute DVT and MTS were at lower risk of PE than were patients with acute DVT without MTS. However, the IVC filter was also a risk factor for contralateral limb DVT. 23 We changed our protocol so that the IVC filter was not routinely implanted before the AngioJet™ rheolytic thrombectomy.
Continued.
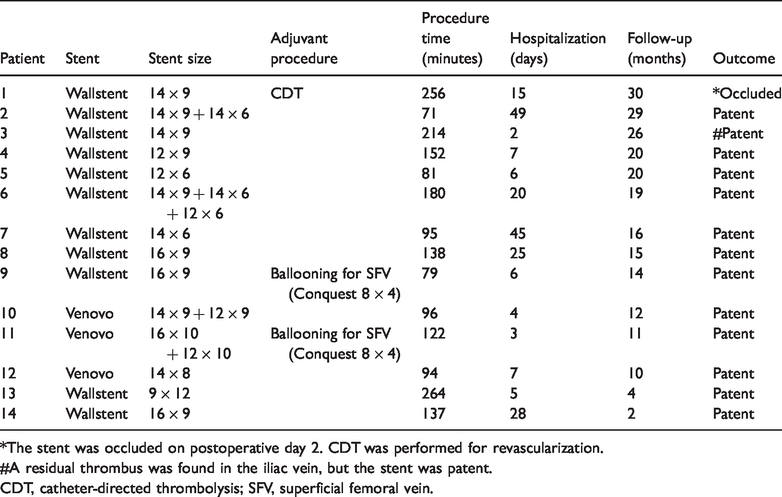
*The stent was occluded on postoperative day 2. CDT was performed for revascularization.
#A residual thrombus was found in the iliac vein, but the stent was patent.
CDT, catheter-directed thrombolysis; SFV, superficial femoral vein.
Conclusions
Although the present study has certain limitations, it has shown that our strategy of employing AngioJet™ rheolytic thrombectomy and stenting of MTS lesions without concomitant coverage of the contralateral CIV may be beneficial for patients with MTS-related DVT.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221100134 - Supplemental material for Clinical outcomes of AngioJet rheolytic thrombectomy in the treatment of May–Thurner syndrome-related deep venous thrombosis
Supplemental material, sj-pdf-1-imr-10.1177_03000605221100134 for Clinical outcomes of AngioJet rheolytic thrombectomy in the treatment of May–Thurner syndrome-related deep venous thrombosis by Wei Wen-Cheng Hsin Chun-Hsien Hsuan-Tzu Yang, Ta-Wei Su, I-Hao Su, Sung-Yu Chu, Po-Jen Ko, Yu Sheng-Yueh Lee Chun-Hui in Journal of International Medical Research
Footnotes
Author contributions
Conceptualization: Po-Jen Ko, Sheng-Yueh Yu, and Chun-Hui Lee. Data curation: Chun-Hsien Hsin and Hsuan-Tzu Yang. Investigation: Ta-Wei Su, I-Hao Su, and Sung-Yu Chu. Methodology: Sung-Yu Chu, Po-Jen Ko, and Sheng-Yueh Yu. Supervision: Po-Jen Ko, Sheng-Yueh Yu, and Chun-Hui Lee. Writing – original draft: Wen-Cheng Wei and Chun-Hsien Hsin. Writing – review and editing: Sheng-Yueh Yu and Chun-Hui Lee.
Declaration of conflicting interests
The authors declare no conflict of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.