
Abstract
Deep venous thrombosis is a common and potentially life-threatening condition that is often associated with various risk factors including underlying malignancy. In this case report, we present a male patient who presented with deep venous thrombosis as the earliest presenting feature of metastatic gallbladder carcinoma. This case report emphasizes the importance of thorough evaluation of patients presenting with unprovoked deep venous thrombosis to early detection of underlying malignancy.
Introduction
Hypercoagulable status leading to superficial and deep venous thrombosis is a well-recognized phenomenon seen in a variety of malignancies.1,2 Clinical presentation with venous thrombosis can occur prior to the detection of underlying malignancy, or it may be detected following the diagnosis and sometimes during chemotherapy for the underlying malignancy. Even though the exact incidence of venous thrombosis associated with cancer is not known, autopsy studies of cancer patients have revealed that venous thrombosis was present in as many as 50% of the cases.3,4 Here we present a male patient who presented with unilateral lower limb deep vein thrombosis as the earliest clinical presentation of metastatic gallbladder carcinoma.
Case presentation
A 43-year-old previously healthy male presented to the local hospital with progressive painful swelling of the right lower limb of 3 weeks duration. There was no preceding trauma to the affected limb or history of fever. He had a history of cigarette smoking of 10 pack years and occasional alcohol consumption. He was a waiter at a hotel, away from his home country, and was engaged in adequate mobilization. He never experienced abdominal discomfort, jaundice or constitutional symptoms such as anorexia and weight loss. Venous duplex ultrasound scan showed right-sided lower limb deep venous thrombosis and he was started on low molecular weight heparin (LMWH). His symptoms improved following 1 week of treatment with LMWH, but he defaulted follow-up thereafter as he was working abroad and had financial restraints. Two months later his symptoms recurred together with right side upper abdominal discomfort and he traveled back to his home country for further assessment and treatment.
On physical examination, he was not pale, not icteric, and had a body mass index of 23 kg/m2. Abdominal examination revealed a non tender right upper quadrant mass. Ultrasound scan (USS) of the abdomen revealed a space-occupying lesion arising from liver segment IV. There was no evidence of chronic liver cell disease. The duplex scan of lower limbs showed extensive deep venous thrombosis involving the right popliteal and right anterior tibial vein and Contrast enhanced Computed tomography(CT) abdomen showed a large 13 × 10 × 9 cm complex lobulated heterogeneous hypodense liver lesion, involving segments 1, 4, 5, 6, with mild heterogeneous peripheral enhancement and an over-distended gall bladder with enhancing mass (Figure 1(a) and (b)). His hematological investigations showed Hb 10.4 g/dl, normal liver function tests, CA19-9 22 U/ml, and alpha-fetoprotein 4.8 ng/ml. His PT/INR and APTT levels were within normal limits. His upper and lower gastrointestinal endoscopies were unremarkable. Histology and immunohistochemistry of the USS guided biopsy from the liver lesion showed a metastatic deposit of an adenocarcinoma. The morphological features and immunohistochemical profile favored an adenocarcinoma of pancreaticobiliary origin (Figure 2). He was started on a therapeutic dose of enoxaparin for deep vein thrombosis. He developed ascites and jaundice over a period of 2 weeks and underwent endoscopic retrograde cholangiopancreatography (ERCP) and palliative biliary stenting. He was referred to an oncology unit for palliative oncological treatment. While he was receiving palliative chemotherapy, he developed heart failure and pneumonia leading to multiorgan failure and death.

CT abdomen ((a)-axial section, (b)-coronal section) showing Gallbladder wall mass with liver metastases.
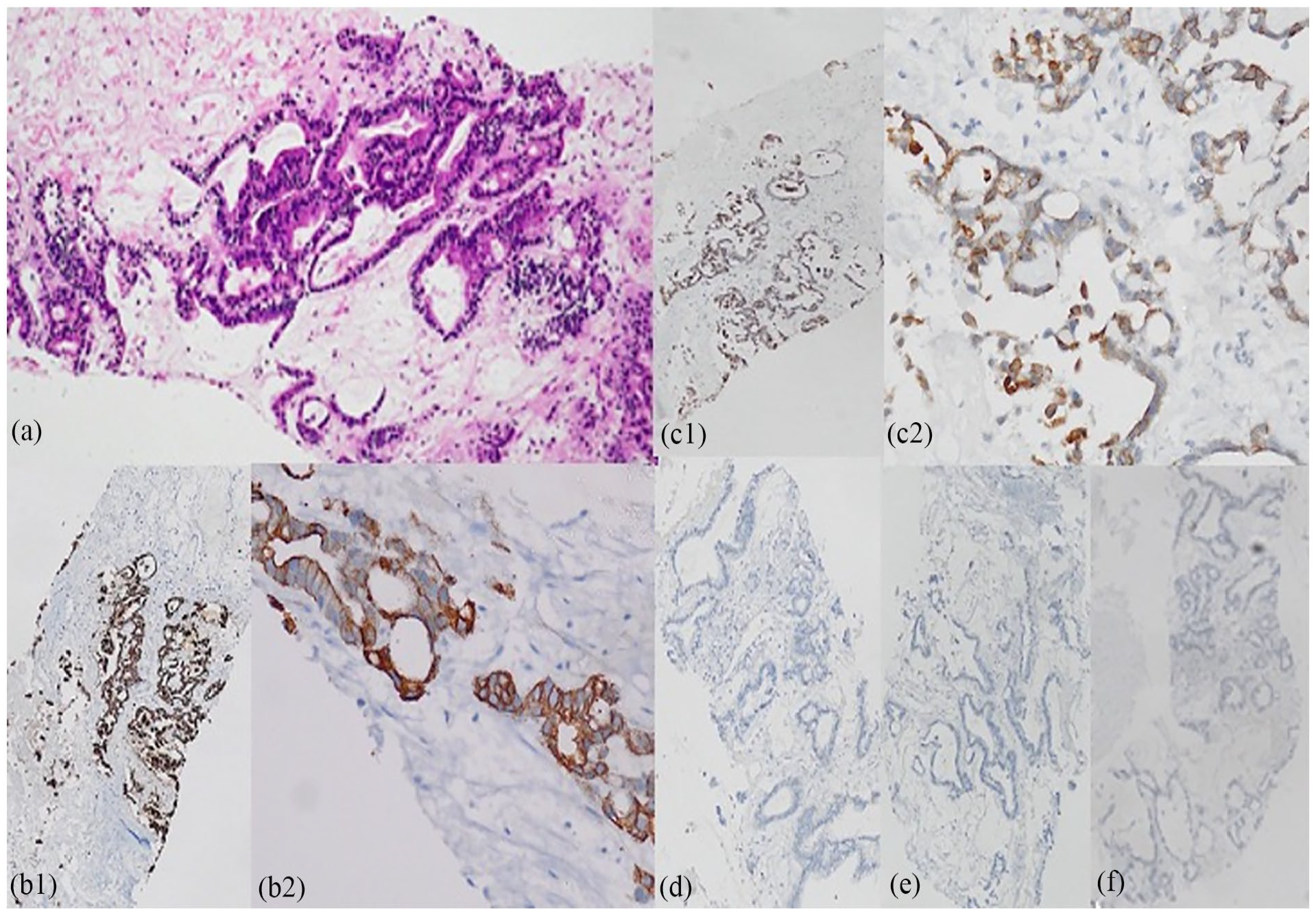
The immunomorphological features favored a metastatic deposit of pancreaticobiliary origin. (a) The tumor was an adenocarcinoma composed of malignant glands (Hematoxylin and eosin × 100) (b) The tumor cells were positive for CK 7 (b1- CK 7 × 100, b2 – CK 7 × 400) (c) The tumor cells were positive for CK 19 (c1 – CK 19 × 100, c2 CK 19 × 400). The tumor cells were negative for (d) CK 20 (CK 20 × 100) (e) Hep Par 1 (HepPar 1 × 100) and (f) TTF-1 (TTF-1 × 100).
Discussion
Malignancy-related deep venous thrombosis is a well-established phenomenon and was first described by Armand Trousseau over 100 years ago and in the current era, it is referred to as cancer-associated thrombosis. 5 Several mechanisms explain this phenomenon, tumor cells secrete procoagulant and platelet-activating substances, and the immune reaction against tumor cells by host cells also induces release of procoagulant factors including tissue factors. These mechanisms create hypercoagulable status and lead to venous thrombosis involving deep and superficial venous systems.1,6 Malignancies of the pancreas, liver, stomach, uterus, lung, and kidney, and primary brain tumors are associated with an increased risk of venous thrombosis. 7 Venous thrombosis is commonly seen in deep veins of the lower limbs and rarely can be seen in visceral veins related to the primary tumor. It has also been noted that mucin-secreting adenocarcinomas have higher risk of causing venous thrombosis. 2 Several previous studies have shown that in patients with idiopathic deep venous thrombosis, about 25% had an underlying undiagnosed malignancy.8,9
Gallbladder carcinoma is a rare malignancy but accounts for about 50% of the malignancies involving the biliary tract. 10 Gallbladder malignancies have aggressive tumor biology, and they are diagnosed at an advanced stage. Most cases of gallbladder malignancy are asymptomatic and detected incidentally during routine imaging for other surgical diseases. Symptoms of gallbladder malignancies are vague and include abdominal pain, indigestion, anorexia, weight loss, and jaundice. Occurrence of venous thrombosis with gallbladder malignancy has been reported in several case reports. Even though the incidence of deep venous thrombosis in gallbladder cancer is low, presence of venous thrombosis in gallbladder malignancy was associated with poor overall survival.11,12
Conclusion
Detection of unprovoked deep venous thrombosis as the earliest clinical feature of gallbladder malignancy is a rare clinical presentation. Clinicians should be aware that gallbladder malignancy at early stage is mostly asymptomatic but can cause unprovoked deep venous thrombosis, and offering suitable tests may help to detect it early.
Footnotes
Acknowledgements
The authors wish to acknowledge all the staff members who involved in patient management
Author contributions
D.S. designed the manuscript. Y.A. writing and assisting the surgeon of the case. H.W. histopathological analysis of the case and providing images of histology slides. N.F. performed ERCP and palliative stenting and revision of the manuscript. D.S. supervisor of the case, primary surgeon of the case, and revision of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative of the subject to anonymized information to be published in this article.