
Abstract
Objective
Implantation of the conceptus in a twin cesarean scar pregnancy (CSP) is considered the rarest type of ectopic pregnancy. Preserving the fetus in utero and effectively dealing with CSP can be challenging. This study aimed to determine the clinical value of ultrasonography by monitoring imaging changes in twin CSP following selective feticide.
Methods
Ultrasonographic and clinical data were collected from four patients with twin CSP who were treated between December 2017 and December 2018 at our hospital.
Results
All patients had a history of cesarean section, followed by a heterotopic CSP, with one embryo implanted into the uterine cavity and the other located in the anterior isthmus. All of the patients were pregnant with twins with double chorionic and amniotic sacs, and all gave birth in our hospital. The patients underwent feticide at 8 to 9 weeks of gestation, after which we focused on monitoring the implantation. Delivery was performed by cesarean section according to scores of an ultrasonic scoring system and clinical manifestations. The patients’ uterus was preserved and they recovered.
Conclusions
This study shows that ultrasound is useful for determining the timing of clinical termination of CSP by selective feticide.
Introduction
One of the rarest types of multiple gestations is a heterotopic pregnancy in which one fetus is intrauterine and the other is ectopic. This condition occurs in approximately 1 of 30,000 pregnancies. 1 Cesarean scar pregnancy (CSP) is also a type of uncommon ectopic pregnancy, comprising only 6% of all ectopic pregnancies.2,3 Implantation of the conceptus within CSP is considered among the rarest and the most dangerous types of ectopic pregnancy, and its etiology remains unclear. 4 If CSP is not diagnosed in a timely manner and treated, it may cause rupture and uncontrolled hemorrhage. Because of the development and application of assisted reproductive technology, the incidence of the intrauterine combined with extrauterine pregnancy has increased over recent years. In China, the cesarean section rate is approximately 50%, and there have been some reports of patients with intrauterine pregnancy complicated by CSP. 5 Nevertheless, these reports have been limited. Generally, efforts are focused on preserving the fetus in utero. If the fetus in utero and CSP are aborted at the same time, the patients have to cope with huge losses. However, preserving the fetus in utero and effectively dealing with CSP can be challenging. Because of the rarity of this condition, there is still no standardized treatment. 6
In the present study, ultrasonographic and clinical data were collected from four patients who were treated for twin CSP following selective feticide at an early stage of pregnancy between December 2017 and December 2018 at our hospital. The ultrasonographic imaging changes were recorded, and their clinical value was determined.
Methods
Patients
We performed a retrospective analysis of ultrasonic images and clinical data of patients with intrauterine pregnancy with twins complicated by CSP. The patients underwent a prenatal examination and delivered between December 2017 and December 2018 in the Third Hospital of Peking University. The observation time was 6 to 8 months from early pregnancy to the end of pregnancy. The outcome was determined 1 week after delivery and data were collected.
Each patient signed an informed consent form that informed the patient about the relevant risks during the operation and the prenatal examination. No ethical approval was required because this study did not involve ethical issues. The article has been prepared according to the STROBE checklist. 7
Procedures and measurements
All patients had undergone a selective cesarean section in the past, which was followed by double chorionic and double amniotic sac twin pregnancies. In the first trimester of pregnancy, A 16-gauge needle was used to aspirate the content of the gestational sac during embryonic feticide in the scar pregnancy without other invasive management procedures. In the process of fetal reduction, under ultrasonic monitoring, a doctor placed a No. 16 straw into the lower fetal sac. The fetal heart was punctured, and potassium chloride was injected into the fetal heart cavity. Because the two embryos were in double chorionic and double amniotic sacs, and potassium chloride was accurately injected into the heart cavity of one embryo under ultrasonic monitoring, the injection did not affect the other embryo. In approximately 5 to 10 minutes, a fetal heart beat was detected in the upper part and no fetal heart beat was detected in the lower part. The next day, another ultrasound scan was performed to confirm this finding. Generally, this method of fetal reduction is safe, but occasionally, both embryos die. Fortunately, this did not occur in our patients. The intrauterine pregnancies were successfully preserved, and this resulted in live births. Placental vestiges were scored using a scoring system after fetal reduction.
Placental attachment scoring system
We designed the placenta accreta scoring system (Table 2) 8 and confirmed its feasibility in the prediction of placenta accreta. To develop this system, we retrospectively analyzed 180 women who were diagnosed with placenta accreta from January 2005 to November 2014 and analyzed 137 patients in a prospective study from January 2015 to October 2016 in the Third Hospital of Peking University. These patients met the following conditions: (1) those who were suspected of having prenatal placenta accreta; (2) those who were assessed by an ultrasound scoring system before delivery; and (3) those who delivered in the Third Hospital of Peking University. According to this analysis, the prediction accuracy of this system was more than 85%, and it could effectively predict the severity of placental implantation and assist doctors in perioperative preparation. This system comprises the following nine scoring items: continuity of clear space, bladder line, lacuna, condition of subplacental vascularity, placental position, placental thickness, blood sinus of the cervix, cervical morphology, and a history of cesarean section. These nine items were rated by 0, 1, and 2 according to the severity, while the total scores reflected the severity of placenta accreta. Receiver operating characteristic curves were used to calculate the critical values of the patients. According to the receiver operating characteristic curves, the boundary value of placenta accreta and increta/percreta was 5, and the boundary value of increta and percreta was 10.
Ultrasonography
We performed color Doppler ultrasound using the Philips Iu22 (Philips Ultrasound, Inc., Bothell, WA, USA) or the GE Volusion E8 (GE Healthcare Austria GmbH, Tiefenbach, Austria). The probe frequency was 3.5 Hz. The patients initially assumed the supine position and assumed the lateral position when necessary. The bladder was moderately filled before the examination. The placental images were taken by longitudinal, transverse, or crown scanning approaches. Because the degree of placenta accreta changes during pregnancy, the final evaluation criteria were based on the last ultrasound score obtained before delivery. The final type of accreta was clearly diagnosed according to the patient's birth and intraoperative clinical conditions.
Clinical data collection
The patients with twin CSP were followed up. We collected their prenatal ultrasound images and clinical data, such as age, number of deliveries, number of cesarean sections, gestational age, intraoperative blood loss, the eventual presence of placenta accreta, and whether the patient underwent hysterectomy. The type of accreta depended on observations during the operation, which were considered as the final criterion. All patients underwent feticide by potassium chloride at 8 to 10 weeks of gestation.
Results
The general information of the four patients included in the study is shown in Table 1. All of the patients had twin pregnancies, with double chorionic and double amniotic sacs. Three of them had a natural pregnancy, and one was assisted with reproductive technology. After feticide in the first trimester, all patients were monitored by ultrasound for scar implantation. The timing of delivery was selected according to the placenta accreta scoring system. No uterine rupture occurred in any of the patients during pregnancy. All neonates were delivered alive, and the uterus was preserved in all patients. Eventually, the mothers and neonates were safely discharged. Details of the patients are described below.
General information of the patients.

CSs, cesarean sections.
Placental attachment scoring system.

Patient 1, who was 29 years old, G2P1, had elective cesarean section performed for placenta previa 2 years previously. When she later became pregnant, B-ultrasound at 8+6 weeks of gestation showed that the appearance of the two fetuses was equivalent to 7+5/8+1 weeks of gestation. There were double chorionic and double amniotic sacs, and one fetus was located at a cesarean scar. The patient underwent a transvaginal reduction of CSP at the 9th week of pregnancy. Ultrasound then showed that the residual muscular layer of the scar was 2-mm thick. There were no major changes in the patient’s scores during pregnancy (scores ranged from 4 to 5 points). This patient’s pregnancy was terminated at 37+ weeks of gestation. She was diagnosed with placenta accreta, and her bleeding volume during the operation was 200 mL.
Patient 2, who was 36 years old, G2P1, had elective cesarean section performed owing to a breech position 2 years previously. She then achieved pregnancy after in vitro fertilization and embryo transfer. At 6+4 weeks of gestation, B-ultrasound showed that the appearance of the two fetuses was equivalent to 6+3/6+3 weeks. One fetus was at the site of a cesarean scar. The patient underwent transvaginal reduction of CSP at the 8th week of pregnancy. Ultrasound then showed that the residual muscular layer of scar was 3-mm thick. The scores of this patient fluctuated between 9 and 13 points. Her pregnancy was emergently terminated at 29+weeks owing to antepartum hemorrhage of 110 mL associated with intrauterine infection. She was diagnosed with placenta percreta, and her bleeding volume during the operation was 3200 mL.
Patient 3, who was 35 years old, G4P1, had elective cesarean section performed for intrauterine infection 3 years previously. After this pregnancy, she had an abortion twice. She then had a natural pregnancy. At 8 weeks of gestation, ultrasound showed double chorionic and double amniotic sacs, and the intrauterine pregnancy was equivalent to 7+6/8 weeks. The location of fetus was considered to be due to CSP, and placenta accreta was present. The patient underwent transvaginal reduction of CSP at the 9th week of pregnancy. Ultrasound showed that the residual muscular layer of the scar was 3-mm thick. The scores in this patient ranged from 9 to 14 points. Her pregnancy was terminated at 35 weeks of gestation. She was diagnosed with placenta percreta, and her bleeding volume during the operation was 1200 mL.
Patient 4 was 34 years old, G2P1, when she had cesarean section performed 3 years previously. She then had a natural pregnancy, with a double chorionic and double amniotic sac. At 7 weeks of gestation, ultrasound showed that the intrauterine pregnancy was equivalent to 6+6/7 weeks. The patient underwent transvaginal reduction of CSP at the 8th week of pregnancy. This patient’s scores ranged from 4 to 8. She underwent an operation at 35 weeks, and was diagnosed with placenta percreta. Her bleeding volume was 2000 mL.
We describe the course of patient 3’s pregnancy in more detail as follows. Patient 3 was 35 years old, with an intrauterine pregnancy equivalent to 7+6/8 weeks, as shown by ultrasound. One fetus was located above the internal cervical orifice, and was on the anterior and posterior wall of the uterus. Abundant cervical blood flow signals were observed. The muscle thickness at the uterine incision was 0.2 cm, and it had visible placental lacunae and a “boiling water” sign that was symptomatic of CSP and placenta accreta (Figure 1). Ultrasound showed a deformed fetal sac of 4.4 × 4.2 × 2.5 cm above the internal cervical orifice 12 weeks after fetal reduction, with no fetal bud and no fetal heartbeat (Figure 2). Honeycomb-like anechoic cells were observed around the fetal sac, and color Doppler flow imaging showed that these were sinuses. The continuous myometrium disappeared in the anterior isthmus of the uterus (Figures 3 and 4).
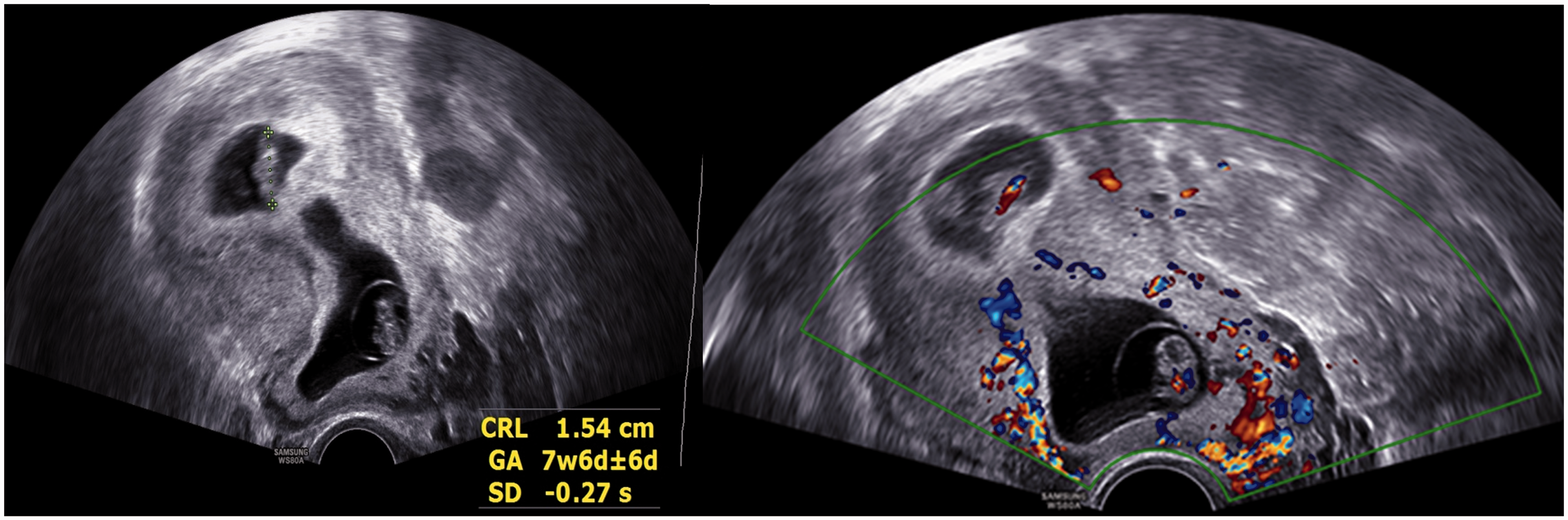
Early pregnancy ultrasound image shows one fetus in cesarean scar pregnancy.
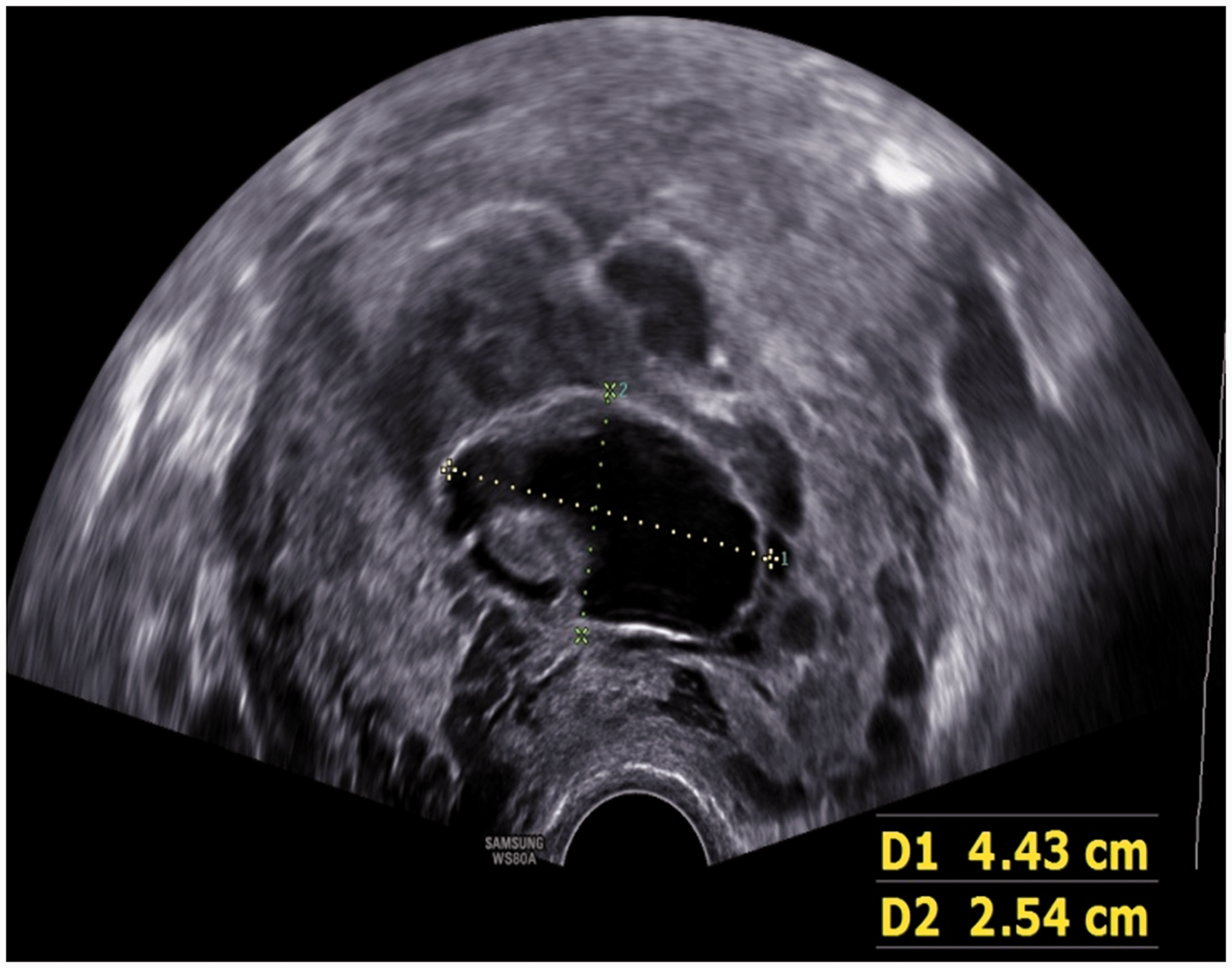
Ultrasound shows the fetal sac after feticide.

After feticide, color Doppler flow imaging shows local disappearance of the myometrium in a uterine scar.

After feticide, color Doppler flow imaging shows that peripheral blood flow is abundant.
According to the placenta accreta scoring system, the following scores were observed: 9 at 16 weeks of gestation, 10 at 25 weeks of gestation, 13 at 32 weeks of gestation, and 14 at 34 weeks of gestation. There was no obvious vaginal bleeding or uterine contraction during pregnancy. Dexamethasone was administered at 28 weeks of gestational age to promote fetal lung maturation, after which the patient was discharged for delivery. Selective cesarean section was planned at 35+ weeks of gestation. During the operation, we found that placental attachment of the lower uterus protruded outward, the local uterine myometrium had disappeared, and only a transparent serosal layer remained. Large vessels were attached to the surface of the uterus, and the implantation area was 5 × 4 cm. The fetus was safely delivered. Apgar scores for 1, 5, and 10 minutes were all 10 points. The birth weight was 2260 g, the bleeding during the operation was 1200 mL, and the uterus was preserved. The pathology was defined as placental hemorrhage and infarction. The mother and neonate were discharged 6 days after the operation.
Discussion
Clinical significance of this study
Twin pregnancy is a common form of a high-risk pregnancy. Studies in China and in other countries have shown that the rate of complications in twin pregnancies is significantly higher than that in singleton pregnancies. 9 CSP is a rare ectopic pregnancy that was first reported by Larsen and Solomon. 10 CSP may result in substantial blood loss, which can be controlled by drastic measures, such as uterine artery ligation, embolization, or emergent hysterectomy.11,12 The occurrence of CSP in conjunction with a viable intrauterine pregnancy and the patient's desire to maintain an intrauterine pregnancy may make the management of this condition even more challenging. The diagnosis of CSP is sometimes not made until uterine rupture occurs, and the patient experiences hemoperitoneum and hypovolemic shock. Emergency hysterectomy may be the only effective treatment available in such cases. However, CSP causes a clinical dilemma when the preservation of intrauterine pregnancy is desired. These types of cases rarely occur. Therefore, there is still no standardized protocol for CSP. In the present study, we only included four patients because this disease is extremely rare. These four cases of twin CSP following selective feticide in the early stage of pregnancy were evaluated by ultrasound monitoring. These results were used for selection of the best timing for terminating pregnancy to achieve good pregnancy outcomes for the mother and neonate. This was a preliminary study of such rare cases, but accumulated experience is required for the treatment of similar cases in the future.
Comparison of this study with other studies
After searching the existing literature, we found only a few articles published in English that reported on individual cases of an intrauterine pregnancy with CSP.5,13–15 They described a heterotopic CSP with one embryo implanted into the uterine cavity, and the other embryo was located in the anterior isthmus wall, which was successfully resolved with feticide at an early stage of pregnancy. There have also been some reports on intrauterine live pregnancy resulting in live births, but they did not mention placenta accreta in the reduction sites. 5 The specific information related to these cases is listed in Table 3.5,13–15 In the present study, we reported four patients with this condition. However, in all of them, placenta accreta occurred in parts of the feticide lesion. According to the placenta accreta scoring system that we designed, we were able to accurately predict the type of placental attachment and the duration of pregnancy. By thoroughly assessing the risk for the mother and neonate, we were able to choose a relatively safe time for delivery. Finally, the gestational weeks were prolonged as much as possible, and all four patients had live births. Moreover, the uterus was preserved in all four patients, and the mothers and neonates were safely discharged.
Characteristics of CSP from previous literature.

CSs, cesarean sections.
Advantages and limitations of the study
Intrauterine pregnancy combined with CSP has been reported in only a few cases worldwide, but there were four cases in our hospital in only 1 year. We have gained some treatment experience by summarizing these cases and also identified two problems to be solved. First, we need to determine how to perform fetal reduction in scar pregnancy and extend the gestational age of intrauterine pregnancy as much as possible so that a live birth can be achieved. Second, although the fetus stops developing at the site of fetocide, the original placental tissue still exists, and placental accreta may still occur. Therefore, we need to determine how to monitor the development of this lesion and avoid the adverse effects of sudden massive hemorrhage and uterine rupture. This is important to ensure the safety of the fetus and the mother in intrauterine pregnancy. The accumulated experience of these four patients can be used to assist in clinical treatment of this type of patient and it lays the foundation for future treatment. Nonetheless, our study has some limitations, such as the small number of cases, and it was a retrospective study. In future work, we will attempt to accumulate more cases and carry out prospective research to further examine the treatment for such patients.
A previous case study showed that, in patients with twin CSP, elective feticide with potassium chloride was successful in terminating the heterotopic pregnancy, leaving placental vascularization intact. 16 In the present study, we performed transvaginal aspiration of the gestational sacs during feticide. Therefore, both of these methods are feasible for CSP. We relied on a scoring system for predicting the type of placental attachment and the degree of risk. According to different scoring levels, customized follow-up and treatment options can be made for patients. Our scoring system showed great clinical significance for the timing of pregnancy termination, preoperative preparation, selection of surgical methods, and organization of experienced teams. The use of a scoring system helped to avoid insufficient or excessive waste of blood, thus reducing the potential maternal and childhood morbidity and mortality. According to our experience, a patient with a score of ≤5 points should undergo repeated ultrasound examinations every 3 to 4 weeks before delivery. They should then attempt to deliver after 37 weeks, depending on the presence of vaginal bleeding, abdominal pain, and other symptoms. A patient with a score of ≥6 and ≤9 should undergo repeated ultrasound examinations every 2 to 3 weeks before delivery. They should attempt to deliver between 35 and 36 weeks according to the patient’s symptoms. A patient with a score of ≥10 should undergo repeated ultrasound examinations every 1 to 2 weeks before delivery. They should attempt to deliver between 33 and 34 weeks according to the patient’s symptoms. In this study, a sonographic feature of twin CSP after selective feticide was that, in the scar of the original cesarean section, the pregnancy focus (infarcted placenta) was observed after the feticide. Different sonographic manifestations depended on the severity of placenta accreta.
Conclusions
Our study shows that ultrasound is important because it provides useful information on the timing of clinical termination of twin CSP by selective feticide at an early stage of pregnancy.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221095683 - Supplemental material for Ultrasound for monitoring twin cesarean scar pregnancy following feticide
Supplemental material, sj-pdf-1-imr-10.1177_03000605221095683 for Ultrasound for monitoring twin cesarean scar pregnancy following feticide by Yiwen Chong, Wei Wang, Aiqing Zhang and Yangyu Zhao in Journal of International Medical Research
Footnotes
Acknowledgements
We wish to thank staff at the Department of Obstetrics and Gynecology Ultrasound and obstetrics lecturers who helped to complete the collection of ultrasound images and clinical data. Finally, we wish to thank the lecturers at the Epidemiology Research Center for their guidance and assistance with statistical analysis and manuscript writing.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the National Key Research and Development Program of China (2018YFC1004100 and 2016YFC1000404).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.