
Abstract
Objective
This study aimed to assess using Doppler ultrasound for analyzing stability of deep venous thrombosis (DVT) of the lower extremities.
Methods
Patients with DVT of the lower extremities who were treated from August 2017 to December 2019 were selected. The patients were divided into stable and unstable groups according to whether thrombus was collected in a filter. Related ultrasound and blood test results were analyzed and compared.
Results
A total of 126 patients with DVT of the lower extremities were included, of whom 74 were in the stable group and 52 were in the unstable group. There were significant differences in the prothrombin time (PT), and lipoprotein alpha, D-dimer, and triglyceride levels between the groups. D-dimer levels >2800 ug/L, smoking, history of venous thrombosis, PT >13.15 s, and body mass index >24.45 kg/m2 were independent risk factors for stability of DVT of the lower extremities. The area under the curve with combined detection of DVT was significantly higher than that for body mass index, PT, and D-dimer alone.
Conclusion
Doppler ultrasound may be reliable for analyzing the stability of DVT of the lower extremities. Related strategies targeting risk factors are required for reducing DVT of the lower extremities.
Introduction
With changes in lifestyle, diet, and population aging, the incidence of vascular thrombosis-related diseases is increasing yearly. The incidence of venous thromboembolic-related diseases is reported to be 0.1%, and it seriously threatens human life and quality of life. 1 Deep venous thrombosis (DVT) is the most serious of the venous thromboembolic-related diseases, such as pulmonary embolism. Shedding of DVT can cause fatal pulmonary embolism, which seriously endangers the life of patients. 2 Early diagnosis and treatment of DVT have been the focus of attention by clinicians and researchers, and these can improve the quality of life and reduce the economic burden of patients. 3
Angiography is a common method for identifying venous embolism, but assessing occlusion of the distal vessel and determining the extent of embolization are difficult. 4 Doppler ultrasound is a non-invasive, convenient, and non-radioactive vascular test, which can accurately and effectively reflect limb vascular conditions. 5 In recent years, many scholars have begun to study the risk factors for DVT in the lower extremities. The risk of detachment of thrombus is correlated with the time of thrombosis, and ultrasound elastography is an accurate method of determining the formation time of DVT. 6 , 7 However, this method is risky because it may cause thrombus to fall off during examination of DVT. Therefore, a safer and more accurate method is required to evaluate stability of DVT. Color Doppler ultrasonography has the advantages of convenience and high accuracy, and it may be more suitable for detecting stability of DVT. 8 Additionally, formation and development of thrombus are affected in many ways. Therefore, the related factors affecting stability of thrombus need to be further studied.
In the present study, we attempted to use color Doppler ultrasound to observe related indicators of DVT combined with clinical symptoms, signs, and laboratory tests. This study aimed to evaluate the ultrasound performance of unstable and stable DVT, and to identify the potential risk factors for stability of DVT of the lower extremities. We hope to provide a reliable basis for clinical diagnosis and treatment of DVT in the lower extremities.
Methods
Ethical considerations
This present study was certified and approved by the ethics committee of Luoyang Central Hospital Affiliated to Zhengzhou University (201711015). Informed consent was obtained from all patients.
Participants
Patients with DVT of the lower extremities, which was diagnosed in the Department of Ultrasound of our hospital from August 2017 to December 2019, were selected. The inclusion criteria of the study subjects were as follows: (1) patients received temporary inferior vena cava (IVC) filter placement; and (2) Doppler ultrasound examinations on bilateral IVCs were conducted before and after removal of the inferior vena cava filter. The exclusion criteria were as follows: (1) catheter thrombectomy was conducted; and (2) permanent, but not temporary, IVC filter placement was performed.
All patients underwent temporary IVC filter placement. The indication of an IVC filter was as follows: (1) the IVC or femoral veins had free floating emboli; (2) pulmonary artery embolism still recurred after anticoagulation treatment; (3) patients had severe congenital heart disease or other cardiopulmonary diseases combined with thrombosis; and (4) patients who could not persist in having anticoagulation therapy. The filter was removed after 10 days. The patients were divided into the stable and unstable groups according to whether the thrombus was collected in the filter.
Anticoagulation therapy
Both groups of patients were provided appropriate general treatment according to their condition, including dehydration, hemostasis, reduction of blood pressure, anti-infection, nutritional support, and brain protection. The affected limb was raised by 30 to 45 degrees. Furthermore, to increase the circulation of venous blood, 50% magnesium sulfate was used for a local wet compress on the affected limbs. Patients in the stable group were administered low-molecular-weight heparin calcium 5000 U periumbilical subcutaneous injection and those in the unstable group were provided low-molecular-weight heparin calcium 1000 U periumbilical subcutaneous injection. All injections were performed once per day for 14 days.
Ultrasound examination
The Siemens Acuson Sequoia 512 color Doppler ultrasound system (Philips iE33; Philips Company, Phoenix, AZ, USA) with a linear array probe and a frequency of 7 to 12 MHz was used for DVT examinations. We explained the purpose and process of the examination to the subject and relatives to obtain their cooperation, and an informed consent form was signed and obtained. During the examination, the patient was fully exposed to the affected limb, and the lower extremity was in a mild external rotation and abducted state. The total femoral, femoral, iliac crest, anterior tibial, posterior tibial, temporal and intermuscular veins were sequentially scanned (Figure 1). The angle between the probe sound beam and the color Doppler flow direction and the axial direction of the blood vessel was <60 degrees, and the echo of the thrombus and blood flow in the lumen were observed. If the patient’s deep venous blood flow showed poor filling or spontaneous imaging, the Valsalva test was used or the patient was instructed to perform deep breathing exercises to determine if color Doppler flow in the lumen was improved. The diagnoses of DVT were as follows: substantial echo in the lumen was observed; collateral vessel formation and blood perfusion were observed; lack of a blood flow signal in the thrombus; and venous blood echoes were observed in the upper and lower reaches of the thrombus, the flow rate was slow, and the echo was moderately concentrated.
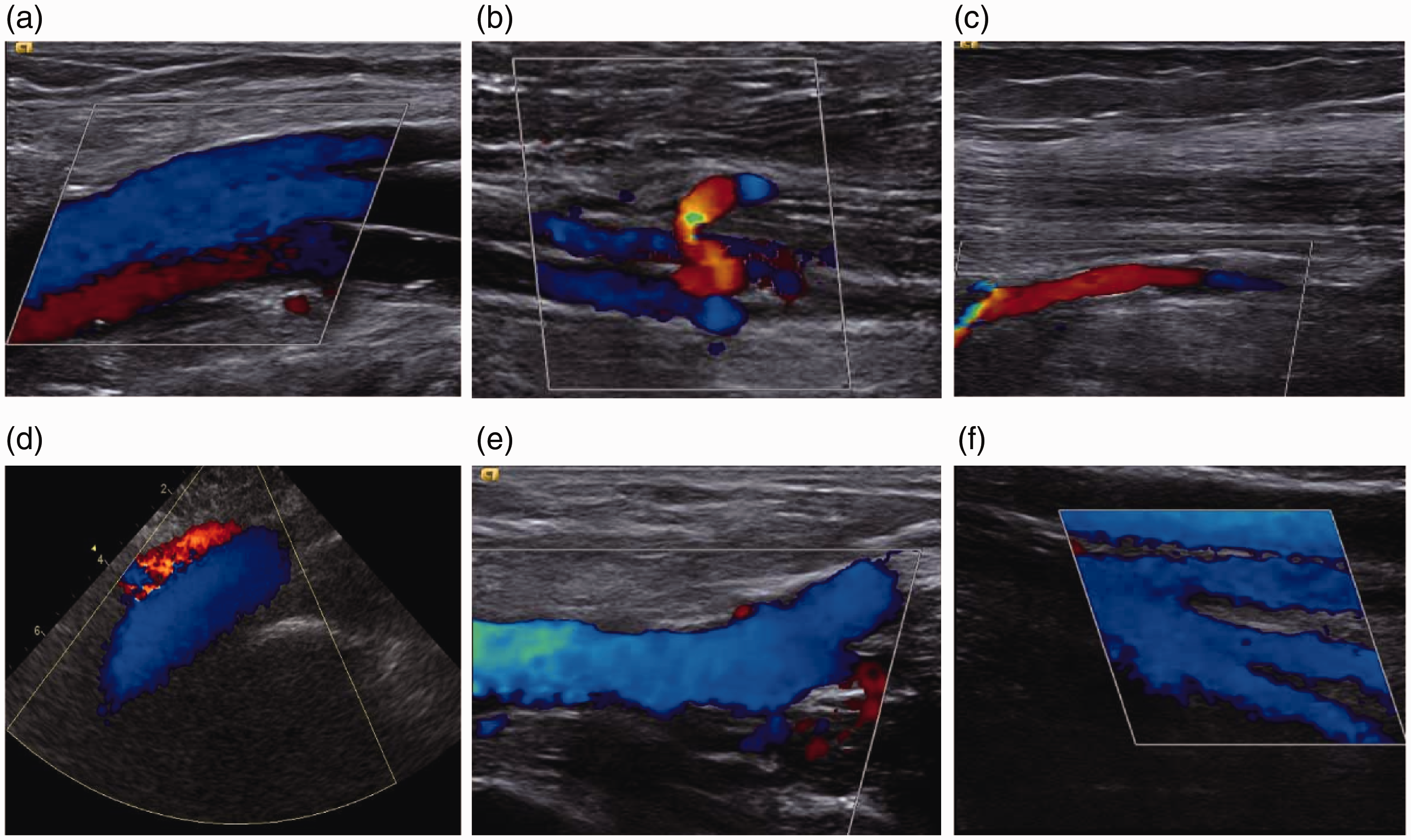
Deep vein examination of the lower extremity by Doppler ultrasound. a, external iliac vein; b, total femoral vein; c, shallow and deep femoral vein; d, axillary vein; e, posterior tibial vein; and f, intermuscular vein.
Blood analysis
We conducted a 1-month follow-up. Venous blood was collected for blood analysis. The STAGO X600 automatic blood analyzer (GE Vivid E9; Siemens Company, Hessen, Germany) was used for blood analysis, and all of the procedures were conducted in accordance with the manufacturer’s instructions. The following blood indices were analyzed: levels of triglycerides, lipoprotein alpha, platelets, total cholesterol, low-density lipoprotein, high-density lipoprotein, apolipoprotein A, apolipoprotein B, plasma fibrinogen, and D-dimer, the thrombin time, activated partial thromboplastin time, and prothrombin time (PT).
Statistical analyses
All collected data were recorded and analyzed using SPSS version 23.0 software (IBM Corp., Armonk, NY, USA). Categorical variables were analyzed using the χ2 test or Fisher’s exact test, and continuous variables were analyzed using the Student’s t test or the Mann–Whitney U test. Data are generally presented as the mean and standard deviation. Multivariate logistic regression analysis was performed using the forward likelihood ratio selection method to identify independent factors of DVT and odds ratios and 95% confidence intervals (CIs) are shown. Potential candidate variables were those with P<0.05 in univariate analyses. Furthermore, we used receiver operating characteristic curves to analyze the diagnostic efficacy and the combined test. A p value <0.05 was considered statistically significant.
Results
Characteristics of the included patients
A total of 126 patients with DVT of the lower extremities were included of whom 74 were in the stable group and 52 were in the unstable group. The overall mean age of the included patients was 50.82±8.95 years old. The characteristics of the patients in the stable and unstable groups are shown in Table 1. The mean BMI was significantly higher, and the mean rates of smoking and a history of venous thrombosis were significantly higher in the unstable group than in the stable group (all p<0.05). There were no significant differences in sex, age, hypertension, diabetes, a history of cerebrovascular disease, local pain, the collateral circulation, and the degree of swelling of the lower extremities between the two groups.
Characteristics of the included patients.

BMI: body mass index.
Blood analysis
The mean PT, and mean lipoprotein alpha and D-dimer levels were significantly higher and the mean triglyceride level was significantly lower in the unstable group than in the stable group (all p<0.05) (Table 2). There were no significant differences in levels of high-density lipoprotein, fibrinogen, total cholesterol, apolipoprotein A, apolipoprotein B, and platelets, and the thrombin time and activated partial thromboplastin time between the two groups.
Results of biochemical blood analysis.

HDL: high-density lipoprotein; FIB: fibrinogen; TT: thrombin time; APTT: activated partial thromboplastin time; PT: prothrombin time; Lpα: lipoprotein alpha; D-D: D-dimer; TG: triglyceride; CHOL: total cholesterol; APO A: apolipoprotein A; APO B: apolipoprotein B; Plt: platelets.
Risk factors for DVT of the lower extremities
D-dimer levels >2800 µg/L, smoking, a history of venous thrombosis, PT >13.15 s, and BMI >24.45 kg/m2 were independent risk factors for stability of DVT of the lower extremities (all p<0.05) (Table 3).
Multivariate analysis of risk factors for deep venous thrombosis of the lower extremities.

SE: standard error; OR: odds ratio; CI: confidence interval; D-D: D-dimer; PT: prothrombin time; BMI: body mass index.
Diagnostic efficacy
Figure 2 and Table 4 show the diagnostic efficacy of BMI, PT, and D-dimer for DVT. The area under the curve for the combination of BMI, PT, and D-dimer was significantly higher than that for each of BMI, PT, and D-dimer alone for detection of DVT (all p<0.05).

Receiver operating characteristic curve analysis on the diagnostic efficacy of body mass index, prothrombin time, and D-dimer levels for detection of deep venous thrombosis.
Diagnostic reference value of BMI, PT, and D-D for deep venous thrombosis.

BMI: body mass index; PT: prothrombin time; D-D: D-dimer; AUC: area under the curve.
Discussion
In recent years, the incidence of venous thrombosis has increased yearly. The incidence of venous thromboembolism in the United States is 104 to 117 per 100,000 cases per year, and in Europe it is 110 to 183 per 100,000 cases per year. There are also 13 to 57 per 100,000 cases of DVT per year in China. 9 , 10 The onset of DVT is relatively insidious and the early clinical symptoms are not obvious. If left untreated, DVT can develop into post-thrombotic syndrome, and it may finally cause fatal pulmonary embolism. 11 , 12 Timely diagnosis and early effective measures can significantly reduce the detrimental effects of DVT. 13 Therefore, clinical attention must be paid to early diagnosis and treatment of patients with DVT.
Currently, the primary method of diagnosing DVT is digital subtraction angiography, but the use of iodine contrast agents may lead to adverse reactions, such as allergies or kidney damage in patients. 14 Additionally, this method is invasive and its use is limited in some community hospitals. 15 In recent years, the technique of ultrasound has become increasingly advanced. The sensitivity of ultrasound detection of DVT is approximately 95% and the specificity is as high as 100%. 16 , 17 Furthermore, ultrasound has the advantages of being real-time, non-invasive, reproducible, and a low cost. 18 Ultrasound may be the preferred choice for diagnosing lower limb DVT in some settings. However, the rate of missed diagnosis of lower limb DVT by ultrasound is approximately 50% in patients without symptoms of DVT. 19 Combined D-dimer and ultrasound screening in patients with acute spinal cord injuries improves the detection of venous thromboembolism. 20 , 21 Therefore, the related risk factors need to be identified to provide evidence for early detection and treatment of DVT.
The fibrinolytic system plays an important role in preventing thrombosis. In the normal state, the coagulation and anticoagulant systems are in a state of dynamic equilibrium. 22 When the equilibrium state is broken, blood clots can be formed if the coagulation system predominates. In the onset of thrombus, the body immediately attempts to dissolve the formed thrombus by activating the fibrinolytic system to produce plasmin, which degrades the cross-linked fibrin, and one of the simplest degradation products is D-dimer. D-dimer levels in patients with DVT are significantly higher than those in the control group.23–25 However, D-dimer levels do not necessarily indicate the presence of thrombosis, especially for patients older than 80 years in whom the D-dimer threshold should be increased. 26 D-dimer levels of the patients in our study were significantly higher than normal values, and D-dimer levels in the unstable group were significantly higher than those in the stable group. This finding indicated that high D-dimer levels have reliable diagnostic value for DVT. Future studies with larger samples are required to identify the diagnostic value of D-dimer and the PT in DVT.
DVT often occurs as an adverse reaction in the treatment of other diseases. DVT can also occur as a complication of a certain disease in cases of orthopedic diseases, respiratory diseases, and cardiovascular diseases.27–29 Approximately 90% patients with tumors have abnormal coagulation function, and the blood is hypercoagulable and easily forms venous thrombosis. 30 , 31 Especially in chemotherapy of malignant tumors, chemotherapy drugs cause damage to the venous wall, which is an important cause of DVT in patients. 32 Inpatients are also prone to DVT of the lower extremities because of prolonged bed rest during hospitalization. 33 Our study showed that patients who smoked, had a history of venous thrombosis, and had a BMI >24.45 kg/m2 were more like to have DVT of the lower extremities. Smoking and obesity have been reported to increase hypercoagulability of blood.34–36 Therefore, strategies on smoking and obesity control are required to prevent DVT of lower extremities.
There are several limitations in the present study. First, as a retrospective study, the accuracy of the collected data and cooperation of identified subjects may have affected the study results. This could have resulted in a certain degree of information bias and deficiency. Second, the included sample was too small with insufficient power enough to provide a reliable cutoff value among the analyzed indices to provide solid evidence for detection DVT. Third, because we only conducted a 1-month follow-up, we did not collect data on mortality. Data on mortality should be an important consideration in future studies. Finally, in our study, the included patients were divided into the stable and unstable groups according to whether the thrombus was collected in the IVC filter. However, thrombus in the IVC filter does not exclude the possibility that it was formed at the IVC filter. Therefore, we might have excluded some patients with thrombus.
In conclusion, Doppler ultrasound appears to be a reliable method to analyze the stability of DVT of the lower extremities. Patients with D-dimer levels >2800 µg/L, smoking, a history of venous thrombosis, a PT >13.15 s, and a BMI >24.45 kg/m2 are independent risk factors for DVT of the lower extremities, and related prophylaxis is warranted.
Footnotes
Author contributions
S Z and G W designed the research; S Z, W Y, H W, and Y L conducted the research; S Z, W Y, Y F, and H L analyzed the data; S Z wrote the first draft of manuscript; and G W had primary responsibility for final content. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.