
Abstract
Heartburn and acid regurgitation are the typical symptoms of gastroesophageal reflux. Despite the availability of several treatment options, antacids remain the mainstay treatment for gastroesophageal reflux-related symptoms based on their efficacy, safety, and over-the-counter availability. Antacids are generally recommended for adults and children at least 12 years old, and the FDA recommends antacids as the first-line treatment for heartburn in pregnancy. This narrative review summarizes the mechanism, features, and limitations related to different antacid ingredients and techniques available to study the acid neutralization and buffering capacity of antacid formulations. Using supporting clinical evidence for different antacid ingredients, it also discusses the importance of antacids as OTC medicines and first-line therapies for heartburn, particularly in the era of the COVID-19 pandemic, in which reliance on self-care has increased. The review will also assist pharmacists and other healthcare professionals in helping individuals with heartburn to make informed self-care decisions and educating them to ensure that antacids are used in an optimal, safe, and effective manner.
Keywords
Introduction
Heartburn is an uncomfortable, burning feeling in the chest, behind the breastbone, or in the upper part of the abdomen that sometimes spreads to the throat. 1 It is specifically related to the reflux of gastric acid through the lower esophageal sphincter, which is a typical symptom of gastroesophageal reflux disease (GERD). Some patients with GERD might also present with atypical symptoms (e.g., epigastric fullness/pressure/pain, dyspepsia, nausea, bloating, belching) and extra-esophageal symptoms (chronic cough, bronchospasm, wheezing, hoarseness, sore throat, asthma, laryngitis, dental erosions). GERD has been classified into three stages based on the frequency of symptoms: stage I (≤3 episodes per week), stage II (>3 times per week), and stage III (daily symptoms). Symptoms are more commonly observed after meals, and they worsen in recumbent positions.
Antacids comprise a major class of over-the-counter (OTC) medicines sold globally, and consumers with acid indigestion and heartburn spend billions of dollars on these non-prescription medications in search of relief. 2 Antacids provide symptomatic relief from heartburn, hyperacidity, acid indigestion, GERD and upset stomach associated with these conditions. 3 Antacids act by neutralizing excess hydrochloric acid (HCl) in gastric juice and inhibit the proteolytic enzyme pepsin. 4 An antacid that increases gastric pH from 1.5 to 3.5 can reduce the concentration of gastric acid by 100-fold. 5 A few studies reported that some antacids can be safely used during pregnancy owing to their local action rather than systemic effects.6,7
The effectiveness of each antacid depends on its neutralizing and buffering capacity. Manufacturers of antacids often reformulate some products to improve their palatability and organoleptic properties for a better consumer experience. Thus, several antacid products are available in the market, each claiming a relative advantage over one another, baffling physicians and the public with choices. The decision to select an antacid can be made according to the acid-neutralizing capacity (ANC), which can differ significantly, but it is unfortunately not stated on product labels. 8 An antacid can also be selected by considering its buffering capacity to maintain gastric pH above 3.5 for a considerable duration. This narrative review provides background and context for the current understanding of antacids and their roles in treating heartburn, practical considerations for clinical practice as well as techniques available to study the ANC and buffering capacity of antacid formulations, and the benefits and drawbacks of methods used. This narrative will also assist pharmacists and other healthcare professionals in helping individuals with heartburn make informed self-care decisions as well as educating them to ensure that antacids are used in an optimal, safe, and effective manner, particularly in the era of the COVID-19 pandemic, in which reliance on self-care has increased.
Materials and methods
The databases Medline, Embase, and Google Scholar were searched for relevant studies using combinations of the following basic and Medical Subject Headings terms: “antacid,” “sodium bicarbonate,” “calcium carbonate,’ “magnesium carbonate,” “magnesium hydroxide,” “aluminum hydroxide,” “acid-neutralizing capacity,” “heartburn,” “gastroesophageal reflux disease,” “GERD,” and “gastric acidity.”
Epidemiology of GERD
In 2020, a meta-analysis of 96 studies from 37 countries reported the global pooled prevalence of GERD as 13.98%, with significant differences identified between regions and countries. In Asia, the estimated rate was 12.92%, versus 19.55% in North America and 14.12% in Europe. 9 Similarly, a previous study also estimated lower prevalence rates of GERD in Asia than in Western countries (10% vs. 14.1%–21.3%). 10 On the contrary, the actual prevalence of GERD in Asia is much higher and similar to that reported in Western countries, but is difficult to determine because of the lack of an exact word for heartburn in some Asian languages, the potential for patient self-treatment, and variation in diagnostic practices and definitions for heartburn and GERD. 11 For instance, the experience, understanding, and reporting of heartburn varied significantly among racial groups. The prevalence of heartburn was higher among African Americans (46.1%) and Caucasians (34.6%) but exceedingly low among East Asians (2.6%). 12 In addition, a group of experts who participated in a Delphi-based study on the management of GERD in the Asia–Pacific region reached a consensus that the prevalence rates of GERD in Asia are increasing. 13
From 2006 to 2016, there has been a significant increase in the proportion of younger patients with GERD, especially within the age range of 30 to 39 years (15–19, 0.2%; 20–29, 2.4%; 30–39, 3.2%; 40–49, 2.8%; 50–59, 2.5%; 60–69, 0.8%, all P < 0.001). 14 Rising obesity and unhealthy dietary patterns might be some of the reasons behind this increased prevalence of GERD in the younger population. 15
It has been estimated that at least weekly symptoms of GERD are most commonly observed among residents of North America (19.8%), followed by residents of Europe (15.2%), the Middle East (14.4%), and East Asia (5.2%). 16 In Australia, approximately 11.3% of the population has chronic GERD. 17 Some studies indicated that GERD symptoms are more prevalent in men than in women; however, evidence is conflicting, and the predominance in men cannot be reliably determined using current data. Nevertheless, complications from GERD do appear to be more prevalent in men. 16
Impact of COVID-19 lockdown periods on gastrointestinal symptoms
Lockdowns have brought significant lifestyle changes. Sedentary lifestyles, remote working, boredom, and anxiety evoked by COVID-19 lockdowns have a direct effect on individuals’ eating behaviors. Significant (P < 0.001) increases in meals consumed, binge eating, snacking, and unhealthy food consumption have been observed during COVID-19-related home confinement. 18 An Italian Internet-based survey among medical students analyzing gastrointestinal symptoms before and during the COVID-19 lockdown period reported an increased prevalence of heartburn (P < 0.001) and indigestion symptoms (P < 0.001) during the lockdown period because of changed dietary habits and anxiety symptoms. 19 Similarly, a cross-sectional survey comparing the prevalence of gastrointestinal symptoms in the Bulgarian adult population before and during the COVID-19 lockdown period reported increased rates of overall gastrointestinal symptoms (68.9% vs. 56.0%, P < 0.001), functional dyspepsia (18.3% vs. 12.7%, P < 0.001), and heartburn (31.7% vs. 26.2%, P = 0.002). 20
Frequently used terms for heartburn
Heartburn is a commonly used but frequently misunderstood word. There is no direct translation for the word heartburn in most languages. It is likely that some meaning may be lost in translation such that the word-for-word translation may carry a completely different meaning. The lack of an exact word for heartburn might contribute to low symptom reporting and a consequently low rate of diagnosis.21,22
Heartburn is often associated with a sour taste in the back of the mouth with or without regurgitation of the refluxate. Heartburn has many synonyms, including “acid indigestion,” “acid regurgitation,” “sour stomach,” “hyperacidity,” and simply “acidity.” Heartburn is usually described as burning discomfort experienced behind the breastbone. Patients describe heartburn as a “burning sensation in esophagus, stomach, throat, trachea,” “a burning feeling rising from the stomach or lower chest up towards the neck,” “a burning, warm or acid sensation in the epigastrium, substernal area, or both,” “a burning feeling in epigastrium rises through the chest in substernal area,” or simply “a feeling of fullness or discomfort in epigastrium”.22 –26 In 2018, Clarrett and Hachem defined heartburn as a burning sensation in the chest that radiates toward the mouth because of acid reflux into the esophagus. 27 The terms “burning,” “hot,” and “acidic” are typically used by patients unless the symptoms become so intense that pain is experienced. 28
Antacids as a mainstay intervention for reflux symptoms
Acid suppression is the backbone for treating heartburn and other reflux symptoms. The World Gastroenterology Organization developed guidelines for the community-based management of common gastrointestinal symptoms recommending antacids, alginates, and histamine H2 receptor antagonists (H2RAs) as appropriate OTC treatment options for infrequent, mild, or moderate symptoms of heartburn. 29 Antacids provide rapid, but temporary and short-term relief of heartburn. Currently, antacid therapy is recommended for mild gastroesophageal reflux symptoms, whereas proton pump inhibitors (PPIs) is recommended for severe symptoms. 30 A position statement from the Indian Society of Gastroenterology on GERD management in adults also recommended PPIs in patients with frequent or severe symptoms. 31 Clinical studies demonstrated that antacid formulations containing sodium bicarbonate, calcium carbonate, aluminum hydroxide, or magnesium hydroxide/carbonate provide significant symptomatic relief against heartburn (Table 1).
Design, intervention (antacid salts), and findings of studies conducted among patients with gastroesophageal reflux disease-related conditions.

aNot relevant because the article was a systematic review of different clinical studies.
bThe data were not available in the published article.
Antacids alone or in combination with PPIs/H2RAs have displayed superiority over placebo/active comparator in various randomized control trials of the treatment of hyperacidity/acid indigestion or GERD-related heartburn and upset stomach (Table 1). However, a discussion on PPIs and H2RAs will not be within the scope of this review article. In addition, a 2009 US community-based survey found that of 42.1% of patients with GERD symptoms who supplemented their PPI treatment with other GERD-related medications, 95.1% used OTC medications. 32 Among OTC medicine users, antacids were the most commonly chosen treatments (84.7% of patients). Antacids are generally considered to have a good safety profile, but high doses and chronic consumption can cause acid rebound through either gastrin release or the direct effect of antacids on parietal cells. 33
Criteria for calling any product an ‘antacid’
Antacids are compared quantitatively in terms of ANC, defined as the number of milliequivalents (mEq) of HCl required to maintain 1 mL of an antacid suspension at pH 3 for 2 h in vitro. According to the FDA, the active antacid ingredient(s) must contribute 25% of the total ANC of the product, and the finished product must contain at least 5 mEq of ANC as measured by the procedure provided in the United States Pharmacopeia 23/National Formulary 18. 34
Impact of heartburn on quality of life and the relevance of antacids in self-care
According to the Genval workshop report, a negative impact on health-related well-being is a criterion for reflux disease when heartburn occurs 2 or more days a week. 35 Studies revealed a significant decrease in well-being with increases in the symptom frequency of heartburn.36 –38 Patients with heartburn had work-related interferences, eating or drinking problems, sleep interruption, and severely impaired daily activity. 39 Nocturnal heartburn, found in 54 ± 22% of patients with GERD, can lead to poor sleep quality followed by sleep arousal, daytime fatigue, and impaired work productivity. 40 Treatment of heartburn symptoms has been significantly associated with improvement in quality of life.41,42 Based on this finding, the World Gastroenterology Organization suggests that the primary goals for self-treating frequent heartburn are the complete symptomatic relief and restoration of quality of life. 29 The reduction of heartburn symptoms is significantly associated with improved quality of life, with the greatest impact on psychological well-being and physical functioning. 41 The use of antacids alone or in combination with other therapies has produced improvements in vitality, physical and social function, and emotional well-being in patients with heartburn.43 –45 Thus, appropriate antacid use can improve health-related quality of life by ameliorating gastroesophageal reflux symptoms.
The World Health Organization defines self-care as “the ability of individuals, families and communities to promote health, prevent disease, maintain health, and to cope with illness and disability with or without the support of a healthcare provider,” which includes non-drug self-treatment and self-medication.46,47 Amid the COVID-19 pandemic, self-care and self-management are even more critical aspects of the evolving healthcare system to manage self-recognized minor ailments such as heartburn and acid regurgitation. The demand for antacids and various OTC medicines has increased because these treatments have proven appropriate for addressing the unmet needs of consumers. 48
This adds to the importance of optimal interfacing between health systems and sites of healthcare delivery. Pharmacists play a vital role in assisting patients to choose self-care approaches and select optimal OTC medicines. Pharmacists can advise consumers on the safe and effective use of antacids, reinforce directions provided by the product labeling, help cease inappropriate use of antacids, and address their interactions with other medications.
The following factors must be considered by healthcare professionals when prescribing/suggesting an antacid:
Pros and cons of various antacids ingredients Supporting body of evidence Impact in special populations Comorbidities and concomitant medications ANC Buffering capacity Risk of rebound acidity
Antacid ingredients: mechanisms to clinical evidence
Antacid products come in powder, tablets, or liquids dosage forms. Antacids contain salts of magnesium, aluminum, calcium, sodium, carbon, or bismuth in their formulations. The combination of two salts, such as magnesium and aluminum, form the principal composition of most antacids. 49 With normally prescribed doses, antacids raise gastric pH significantly; however, the onset of action depends on the dose, dosage forms, and extent of chewing (for tablets). For example, powder forms of antacids exhibit a faster onset of action than liquid forms. 50 Effervescent powder forms of sodium bicarbonate antacids can start neutralizing acid in a few seconds. 51 Antacids have a duration of action of 20 to 60 minutes when ingested on an empty stomach. After a meal, approximately 45 mEq/hour HCl is secreted. A single dose of 156 mEq of antacid given 1 hour after a meal neutralizes the acid for up to 2 hours. 52 The ANC of different formulations of antacids is highly variable. Powder and liquid preparations of antacids usually have higher ANCs than tablets. 53
Antacids have been classified into two classes: systemic or absorbable and non-systemic or non-absorbable antacids. Absorbable antacids are readily absorbed into the systemic circulation, and they can produce systemic electrolytic alterations as well as alkalosis (e.g., sodium bicarbonate). Non-absorbable antacids such as aluminum hydroxide, aluminum phosphate, calcium carbonate, and magnesium hydroxide are not absorbed to a significant extent; e.g., only 15% to 30% of calcium and 5% to 10% of magnesium are absorbed from their respective antacid formulations.54 –56
Each antacid ingredient has a unique mechanism with the ultimate goal of acid neutralization (Figure 1). Ingredients with different features and limitations provide options to physicians for addressing the intra- and intersubject variability of patients. The features and limitations of various antacid ingredients are presented in Table 2.

Effects of different antacid ingredients on gastric acid. The representative figure presents the mechanism of carbonate salts only. Other antacid salts were discussed in the article. Most of the gastric acid (approximately 45 mEq/h) is secreted across the apical membrane of the stomach through a proton pump (H+/K+ ATPase) after meal consumption. The carbonate salt of antacids binds to H+ ions from gastric hydrochloric acid to produce chloride salts (calcium chloride, sodium chloride, magnesium chloride, and aluminum chloride), carbon dioxide, and water. This decreases H+ concentrations in the stomach, thus raising the pH. The orange region denotes the acidic environment of the stomach, the green region denotes the antacid-mediated neutralization/adsorption of gastric acid, and the yellow region denotes alkalized/neutralized gastric acid. In the alkaline conditions of the small intestine, soluble calcium chloride, sodium chloride, magnesium chloride, and aluminum chloride are converted back to their carbonate salts. The sodium bicarbonate rapidly empties into the small intestine, where it is absorbed; thus, it is considered an absorbable antacid. Calcium carbonate, magnesium carbonate, and aluminum carbonate are excreted with the stool, decreasing their absorption; thus, they are considered non-absorbable antacids.
Features and limitations of different types of antacid salts.
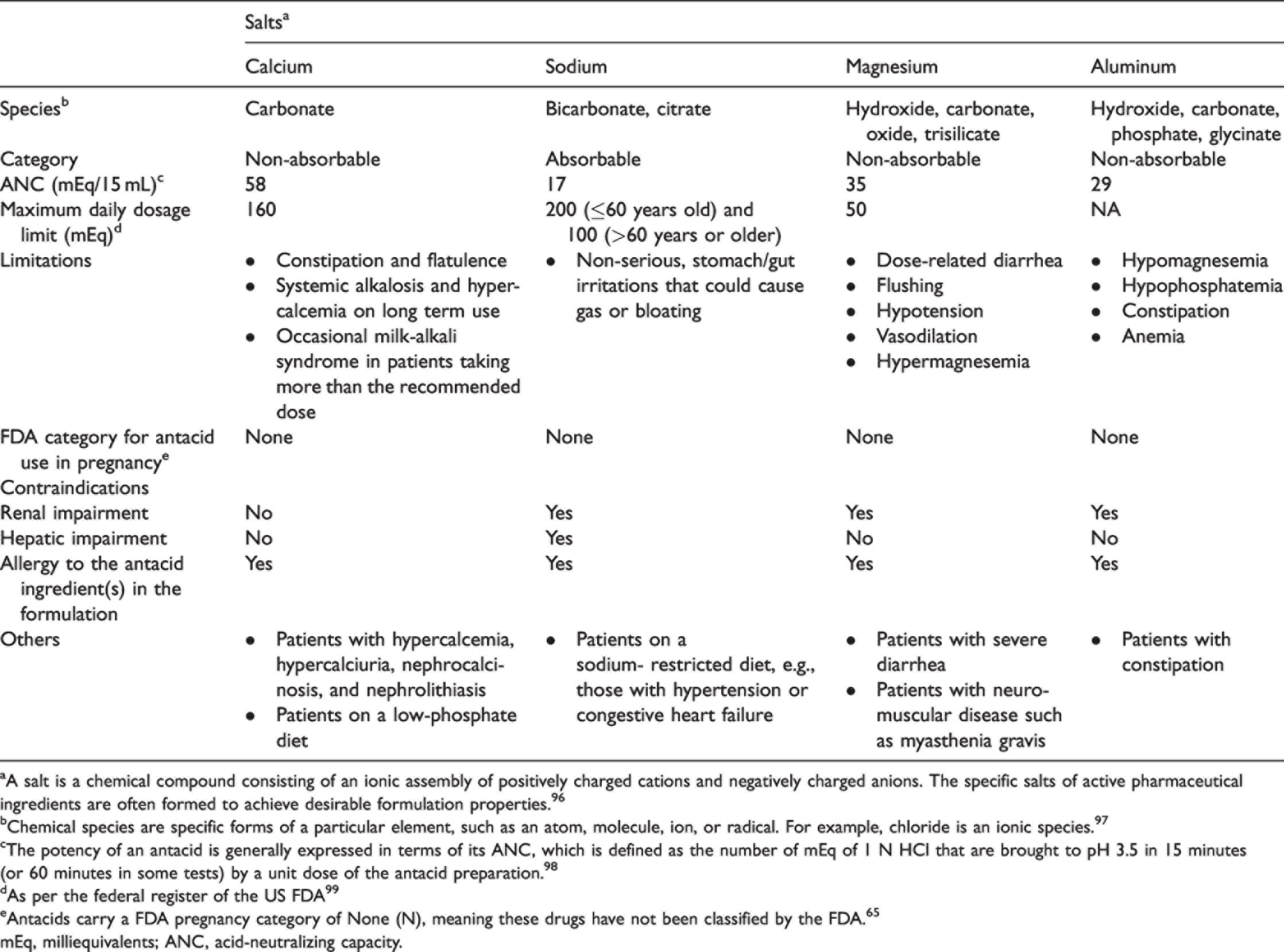
aA salt is a chemical compound consisting of an ionic assembly of positively charged cations and negatively charged anions. The specific salts of active pharmaceutical ingredients are often formed to achieve desirable formulation properties. 96
bChemical species are specific forms of a particular element, such as an atom, molecule, ion, or radical. For example, chloride is an ionic species. 97
cThe potency of an antacid is generally expressed in terms of its ANC, which is defined as the number of mEq of 1 N HCl that are brought to pH 3.5 in 15 minutes (or 60 minutes in some tests) by a unit dose of the antacid preparation. 98
dAs per the federal register of the US FDA 99
eAntacids carry a FDA pregnancy category of None (N), meaning these drugs have not been classified by the FDA. 65
mEq, milliequivalents; ANC, acid-neutralizing capacity.
Pepsin and bile acid inhibition activity
Pepsin is a proteinase that is produced from the inactive form pepsinogen by the parietal cells of the gastric mucosa, whereas bile acid is a digestive liquid produced by the liver.
Pepsin is activated at pH 1 to 2, and it has limited activity when the pH is around 3.5 to 5. 57 Glyco- and tauro-conjugated bile acids have been reported to be harmful to the esophageal mucosa at acidic pH (pH <4 and even down to pH 2 for tauro-conjugated bile acids). 58 In patients with reflux disease, both pepsin and bile acids have been found in the esophageal reflux. 59 Pepsin in the refluxate disrupts the esophageal mucosal barrier by acting on the epithelial cell surface, whereas bile acids achieve the same effect by diffusing into cells and damaging them. 60 Thus, the activity of pepsin and bile acids should be limited to prevent such damage. In 1971, an in vitro experiment by Kuruvilla revealed high anti-peptic activity (82% and 81%, respectively) for both magnesium carbonate and calcium carbonate. 61 In addition, aluminum and calcium antacids appear to adsorb pepsin and reduce its activity more strongly than would be predicted by pH changes alone. 62 Antacids such as magnesium and aluminum hydroxide can bind to bile salts, but magnesium hydroxide binds to bile salts at a much lesser extent than aluminum hydroxide.52,63 Thus, antacids are used as add-on treatments for gastritis, peptic ulcer disease, and esophagitis.
Special populations
Management of heartburn during pregnancy
Heartburn is a common consequence of pregnancy. Prior research presented the prevalence of heartburn as 22% in the first trimester, 39% in the second trimester, and 60% to 72% in the third trimester. 64 Increases in the levels of female sex hormones such as progesterone can reduce lower esophageal sphincter pressure. The step-up algorithm, starting with dietary changes and lifestyle modifications, should be used to manage heartburn during pregnancy. Antacids carry an FDA pregnancy category of none (N), which means these drugs have not been classified by the FDA. 65 Antacids are recommended as first-line treatments for heartburn in pregnancy when lifestyle modifications fail. If symptoms persist despite antacid use, then H2RAs can be used, excluding nizatidine because it has been found to be teratogenic in animal studies. All PPIs and H2RAs are FDA category B drugs, excluding omeprazole, which is an FDA category C drug. PPIs are reserved for women with complicated GERD or intractable symptoms. Approximately 30% to 50% of pregnant patients with symptoms will never need to “step-up” therapy from antacids. Although magnesium-, calcium-, and aluminum-containing antacids display good safety profiles during pregnancy, they should not be used for long-term therapy or in large doses.66,67 Treatments containing sodium bicarbonate should be avoided in pregnancy because of risks of fluid overload as well as maternal and fetal metabolic alkalosis risks (Table 2).
Management of gastroesophageal reflux in children
Infants normally experience gastroesophageal reflux symptoms that peak at 4 months of age because of physiological factors, and these events resolve over time. Antacids are not useful in infants with reflux symptoms, but they may be considered for short-term use in older children (12 years and older) to relieve heartburn.68,69 If regurgitation becomes frequent, then lifestyle changes, postural therapy, and thickened feedings should be considered.70,71
Comorbidities and concomitant medications
Similarly as any other medicines, antacids can potentially cause drug–drug interactions, especially in patients with comorbidities such as renal or hepatic impairment in those taking concurrent medications without medical supervision. Antacids can influence the rate and/or extent of absorption of concurrently administered drugs with pH-sensitive release from a dosage form, pH-dependent stability, or pH-dependent solubility by increasing gastric pH. 72
ANC and reliability of the in vitro test used
ANC, stated in mEq, is the amount of acid that can be neutralized using one standard dose of an antacid. The most effective antacids should have a high ANC that can be estimated by back titration through in vitro experiments. 73 The back titration method, a static test, is useful for comparing the level of neutralization achievable by a range of antacids, but it does not consider their rate of reaction. At least three variables, namely gastric secretion, gastric emptying, and the acid-consuming capacity, influence the efficacy of an antacid in vivo. The impact of the former two variables cannot be determined by back titration. However, more sophisticated in vitro models (e.g., dynamic simulators) can both measure all of these variables and offer a faster and more ethical alternative to studies in animals and humans. 74 According to the Committee for Medicinal Products for Human Use, the therapeutic equivalence of locally acting gastrointestinal products can be demonstrated using these in vitro or in vivo methods, provided they have been proven to accurately reflect in vivo drug release and availability at the sites of action. 75 The type of studies required to demonstrate equivalence should be determined via careful consideration of the product characteristics, mechanism of action, underlying disease being treated, validity of any in vitro or in vivo studies, the effects of any excipients, and differences in dose delivery systems.
Buffering capacity and reliability of the in vitro test used
Various in vitro tests have been developed to evaluate the buffering capacity of antacids. These tests include pH-stat titration and continuous acid challenge tests such as the Rossett–Rice method, the Simulator of the Human Intestinal Microbial Ecosystem (SHIME®), and the TNO Simulated Gastro-intestinal Tract Model 1 (TIM-1). These tests are dynamic, and they provide a more precise measure of antacid reactivity. pH-stat titration provides an accurate estimation of the rate at which the antacid is reacting under in vitro or fixed conditions, but it provides little information of its in vivo behavior.
By contrast, continuous acid challenge tests can serve as predictors of in vivo behavior. These tests are generally used to measure maximum pH achieved by an antacid, its duration of action, and the amount of antacid that will be lost if gastric emptying is simulated. The gastric emptying rate is an important factor for slowly reacting antacids such as magnesium trisilicate. The Rossett–Rice test is an acid neutralizing dynamic assay used as a standard to evaluate or compare the in vitro efficacy of antacid formulations. Using the Rossett–Rice test, Deepika et al. reported that the pH of acidic content was increased to 3.5 significantly faster and pH ≥3.5 was retained for a longer period with a sodium bicarbonate, sodium carbonate, and citric acid combination than with an aluminum hydroxide, magnesium hydrochloride, and simethicone combination. 50 The SHIME® apparatus mimics the physiological and microbiological conditions of the human gastrointestinal tract. The apparatus is the conglomeration of five reactors simulating different processes that occur in the human gastrointestinal tract. The steps required for food uptake and digestion in the stomach and small intestine are simulated by the first two reactors, whereas the other three compartments represent the ascending, transverse, and descending colon, respectively. 76 TIM-1 is a computer-controlled, dynamic, multi-compartmental system that simulates all physiological processes of the human upper gastrointestinal tract (lumen of the stomach and small intestine). 74 It offers relatively easy manipulation, reproducibility (no biological variation) and, most importantly, accuracy compared with in vivo techniques.
Summary
Antacids are widely used globally for the treatment of symptoms of acid-reflux related conditions. Despite their rapid action and good safety profile, antacids with a high ANC and good buffering capacity are required for the efficient management of these conditions. The ANC and buffering capacity can be measured using well-established test methods, thus making them predictive of the clinical effectiveness of antacid preparations in relieving gastrointestinal symptoms. For these reasons, providing the ANC and buffering capacity on labels as previously suggested could help ensure the quality, efficacy, and value of antacids. Nevertheless, the potential for adverse effects or drug interactions exists. Awareness of these possibilities is important because patients often fail to inform their physicians about antacid use unless specifically asked. Self-care and self-management are critical aspects of the evolving healthcare system in managing self-recognized minor ailments such as heartburn and acid regurgitation. To support this, pharmacists, the most accessible healthcare professionals, can improve patients’ awareness about antacid therapy and its related possibilities through counseling and education.
Footnotes
Acknowledgements
Syed Obaidur Rahman, Rajiv Kumar, and Nitu Bansal from WNS Global Services provided editorial and medical writing assistance with funding from GSK Consumer Healthcare.
Declaration of conflicting interests
All authors are employees of GSK Consumer Healthcare.
Funding
Not applicable