
Abstract
This study investigated the surgical method and therapeutic effect of retrograde island flap bridge transfer of the adjacent phalangeal artery combined with vascular pedicle tubular skin grafting to repair finger pulp defects. From June 2008 to May 2020, 21 fingers (19 patients) were repaired using this method. The postoperative flap survival rate and complications, and the clinical effect, were evaluated. All flaps survived, and all patients were followed-up for 12 to 46 months. The static two-point discrimination (2PD) was 7 to 11 mm, no apparent complications were observed in the donor area and the McIndoe cold intolerance symptom severity (CISS) scores indicated mild severity. The Michigan hand outcome questionnaire (MHQ) indicated that all patients were satisfied with their overall hand appearance and function. Results were excellent in 15 cases and good in 4 cases, according to the Dargan function evaluation (DFE). It is safe and effective to repair finger pulp defects with a retrograde island flap bridge transfer of the adjacent phalangeal artery combined with vascular pedicle tubular skin grafting. This skin flap has the advantages of simple severing, good texture and concealed donor area, which is convenient for early postoperative functional exercise of the finger.
Keywords
Introduction
The finger pulp dense texture and sensation act as the “eyes” of the hand; however, finger pulp injury is common, clinically. Owing to the similarities between finger and toe structure, lateral flaps of the toe have historically been the best method to repair defects of the finger pulp.1–3 However, free toe skin flaps have many disadvantages, and it is not easy for patients to accept the aesthetic results. When the proximal end of the finger is seriously injured, or a finger pulp defect extends past the distal interphalangeal joint, an island flap of the digital artery of the injured finger cannot be used for repair, and an island flap of the adjacent digital artery will be used for repair. However, this surgical method results in large scars on the palm and has significant drawbacks.4–6 The digital artery dorsal cutaneous branch-chain flap of the adjacent finger causes only minor damage to the finger because the vessel is not connected to the main branches of the digital artery. However, owing to the slender perforating branches of the blood vessels, this flap often has an insufficient blood supply and a high probability of necrosis. Furthermore, the connective tissue of the skin on the back of the finger is loose, although the sliding properties are suitable; the skin is thin, the position is exposed, the repaired finger pulp is incomplete and the texture and sensory recovery are poor. There are many insufficiencies in the repair of finger pulp defects.7–8 The digital artery flap is still the most popular flap, clinically, because of its safety and good postoperative effects. The flap in this study is located on the side of the finger. The donor area is hidden and can carry the dorsal branch of the digital nerve to restore feeling in the flap. After the flap is severed, the skin graft in the donor area survives, sacrifice of sensory function is minimal and the appearance, and texture and sensation in the recipient area are good. From June 2008 to May 2020, 21 fingers (19 cases) with finger pulp defects were repaired by reverse island flap bridge transfer of the adjacent phalangeal artery combined with vascular pedicle tubular skin grafting, and satisfactory results were obtained. The details are reported in this article.
Patients and data
In this study, there were 19 cases (21 fingers) comprising 12 men (12 fingers) and 7 women (9 fingers) with an average age of age 40.7 years (range: 16–57 years). The cause of injury in all cases was crushing injury by a machine. The injured sites were the index finger (4 cases), middle finger (5 cases), ring finger (6 cases), little finger (2 cases), index finger and little finger (1 case) and middle finger and ring finger (1 case). There were 14 cases (16 fingers) with severe contusion of the proximal and middle phalangeal bones combined with finger pulp defects and 5 cases (5 fingers) with finger pulp defects extending further than the distal interphalangeal joint with all phalangeal bones exposed. Defect area measurements ranged from 2.4 cm × 1.8 cm to 4.5 cm × 2.2 cm, and the operation time ranged from 1.4 hours to 2.5 hours. The fingers involved and the characteristics of the defects are shown in Table 1.
The patients’ demographic data, injury types and defect sizes.

Sex: 1: male, 2: female, M: finger pulp defect extending past the distal interphalangeal joint, N: severe contusion of the proximal and middle phalanges combined with finger pulp defect.
This retrospective study was approved for publication by the Ethics Committee of the Affiliated Jiangnan Hospital of Zhejiang Chinese Medical University (Hangzhou Xiaoshan Hospital of Traditional Chinese Medicine; Approval Number: XSZYY2081115), and the study was performed in accordance with the tenets of the Declaration of Helsinki. All patients agreed to participate, provided written informed consent prior to treatment, and signed the consent for publication form, including consent for the use of accompanying images. A copy of the written consent is available for review by the Editor of this journal. The reporting of this study conforms to the CARE guidelines. 9
Inclusion and exclusion criteria
Inclusion criteria
1. Age ranging from 15 to 60 years in patients with a clear mind and no psychological disorders, and able to participate in treatment and follow-up. 2. Skin and soft tissue defect of the finger pulp, including defects extending further than the distal interphalangeal joint (indicating that the digital artery arch has been damaged), combined with severe injury of the proximal finger, or vascular injury, inflammatory oedema and poor skin condition. Additionally, each patient had high requirements and hopes to retain the finger and restore good sensory function of the finger pulp. 3. No finger injury in the adjacent finger donor area.
Exclusion criteria
1. Simple skin and soft tissue defect of the finger pulp and good skin and soft tissue conditions in the proximal finger that could be repaired with a free flap or island flap from the same finger. 2. Patients older than 60 years of age. 3. Patients addicted to smoking and those with poor compliance during treatment and who could not cooperate with bed rest treatment requirements.
Treatment methods
Preoperative treatment
After admission, patients received symptomatic support, such as analgesia and anti-inflammatory treatment. All patients underwent preoperative examinations to assess the surgical risks.
Surgical methods
After brachial plexus nerve anaesthesia, the operative area was cleaned and disinfected and a sterile drape was placed. The wound was then thoroughly debrided and haemostasis was established. Next, the skin flap was designed and incised at the proximal end of the adjacent finger according to the size of the wound. A serrated incision was made on the side of the distal finger to create the flap, and a subcutaneous tunnel was opened along the incision. The skin flap was then cut, the internal digital artery of the skin flap was ligated and cut from the proximal high position and the digital artery and dorsal branch of the digital nerve were brought into the skin flap. Next, the vascular pedicle was separated retrograde along the proper digital nerve to the distal middle segment or the distal interphalangeal joint. Generally, the length of the vascular pedicle was approximately 2 cm. The tourniquet was released, which was placed to stop wound bleeding, and the blood circulation to the skin flap was observed. After the skin flap became ruddy in colour, the incision at the pedicle was sutured, and a medium thickness skin graft was taken from the abdomen or elbow crease. The wound in the donor area was sutured, and the skin flap was transferred to the recipient area. The dorsal branch of the digital nerve carried by the skin flap was anastomosed to the stump of the intrinsic digital nerve at the wound surface under a microscope then the skin flap was sutured to cover the wound surface. The exposed vascular pedicle was covered by a tubular skin graft wrapped with excess tissue from the medium thickness skin graft.
Postoperative management
After the operation, the affected limb was fixed with a plaster support with the wrist joint in 60 degrees of flexion. An area extending 30 to 40 cm from the grafted skin flap was kept warm by continuous infrared irradiation. Postoperatively, the patients received anti-infection, anti-vasospasm and anticoagulation therapy and analgesia, and blood circulation to the flap was closely observed. One week postoperatively, the fixation and dressings were removed, and the patients were instructed to begin to exercise their fingers in flexion and extension. The pedicle was severed 16 to 22 days after surgery. The appearance, sensation in the finger pulp and functional recovery of the finger joint were observed throughout the follow-up.
Results
At the final follow-up, sensation in the flaps and donor sites was assessed using static two-point discrimination (2PD). 10 Cold intolerance was evaluated using the Blond McIndoe cold intolerance symptom severity (CISS) score. 11 The CISS scores were arbitrarily grouped into four ranges: 0–25, 26–50, 51–75 and 76–100, which corresponded to mild, moderate, severe and extreme severity, respectively. The patients reported their satisfaction with the functional recovery of the injured fingers using the Michigan hand outcome questionnaire (MHQ), 12 with higher MHQ scores indicating better hand health. The function of the finger joint was evaluated according to the Dargan function evaluation, as follows: 13 excellent: the tip of the finger in flexion passed the transverse pattern of the palm; good: the tip of the finger in flexion reached the transverse pattern of the palm, and generally, the distance between the tip of the finger in flexion and the transverse pattern of the palm was less than 2 cm; poor: the distance between the tip of the finger in flexion and the transverse pattern of the palm was >2 cm. The outcomes were assessed by an independent senior surgeon blinded to the procedures.
Nineteen patients were followed-up for 12 to 46 months. All flaps survived, with no effect on survival owing to the length of the vascular pedicle. There were no deep infections in the donor and recipient sites. The texture of the skin flaps was good, and the appearance was natural and not bloated. There was no effect on finger blood circulation, fingertip sensation or joint activity in the donor area. There was also no discomfort during the follow-up period, such as fear of cold. There were no ulcers in the skin graft in the donor area and only slight numbness on the side of the back of the middle finger in the donor area. The sensations of pain, temperature and touch recovered well, and the CISS scores indicated mild severity. The 2PD was 7 to 11 mm, and there was no apparent dysfunction in the donor area. There were no complications, such as infection, venous reflux disorder, redness, swelling and cyanosis in the transplanted flaps. According to the MHQ at the last follow-up, 19 patients were delighted with their hands’ overall appearance and function. There were 15 excellent cases and four good cases according to the finger joint Dargan function evaluation (Table 2). Typical cases are shown in Figure 1–2.
The patients’ clinical and functional results.

CISS: cold intolerance symptom severity, 2PD: two-point discrimination, MHQ: Michigan hand outcome questionnaire, DFE: Dargan function evaluation.

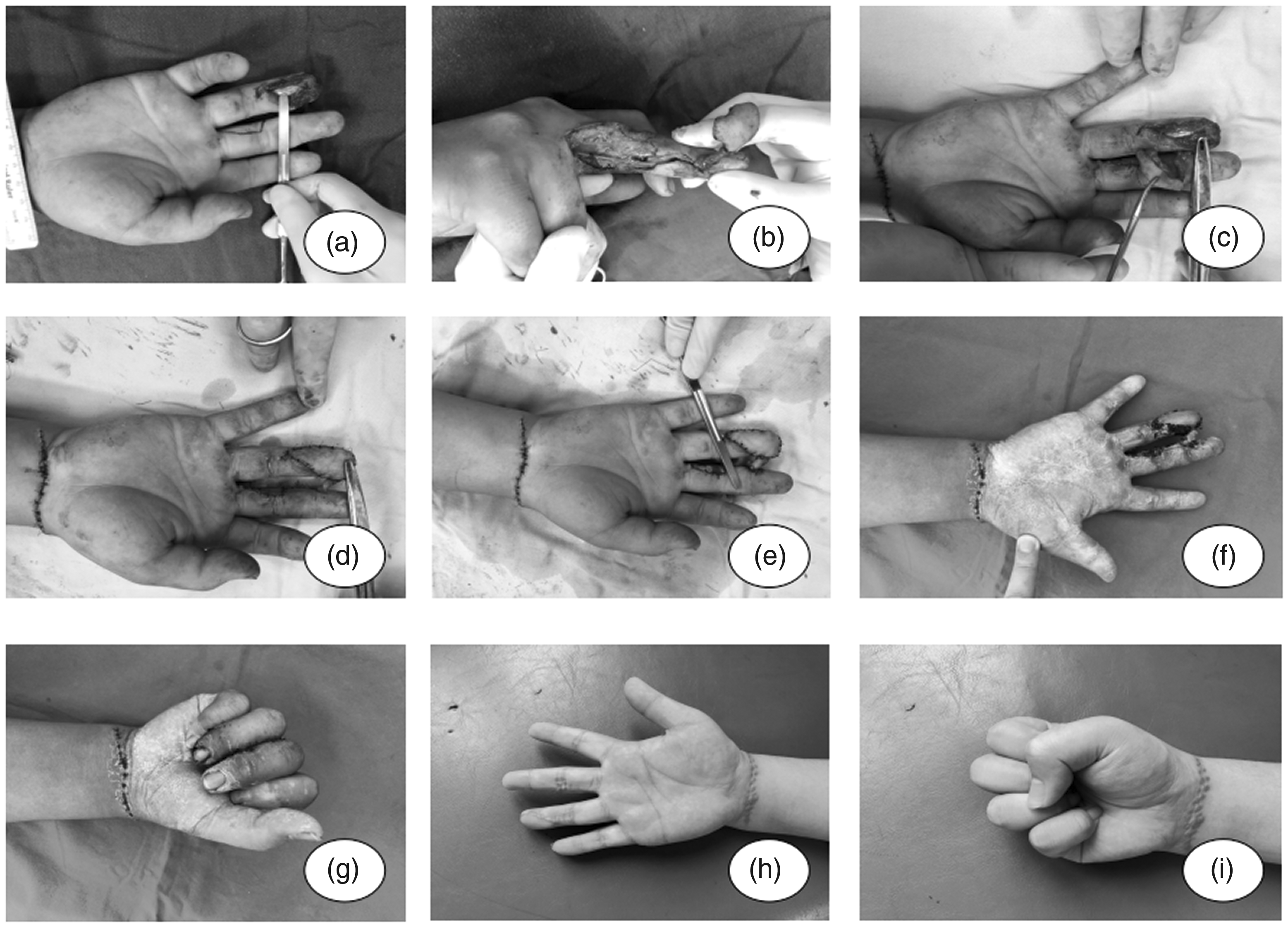
Patient, female, early 50s. (a) Preoperative appearance of the left middle and ring finger injuries. (b) The appearance of the wound surfaces after debridement and suturing. (c) Intraoperative appearance of the flap. (d and e) Intraoperative flap transplantation. (f) Intraoperative tubular skin grafting at the vascular pedicle. (g) Survival of the flap after pedicle amputation. (h and i) Postoperative skin flap appearance and finger function.
Patient, male, early teens. (a) Preoperative appearance of the right ring finger injuries. (b) Intraoperative appearance of the flap. (c and d) Intraoperative flap transplantation. (e) Intraoperative tubular skin grafting at the vascular pedicle. (f and g) Survival of the flap after pedicle amputation. (h and i) Postoperative skin flap appearance and finger function.
Discussion
Research status of flap repair for finger pulp defects
With the development of the manufacturing industry and the popularisation of mechanical operations, hand injury, especially finger pulp defects, are seen increasingly more often, clinically, and the treatment technology is becoming mature. The hand is a motor organ and a crucial cosmetic organ; therefore, repairing hand defects strives to achieve both ideal appearance and function. The skin overlying the finger pulp is composed of dense connective tissue, containing rich nerve endings and sensory corpuscles, and there are many vertical fibres in the dermis to fix the skin to the phalanx and deep fascia. Therefore, the skin overlying the pulp of the finger has low slippage, good wear resistance and acute sensation.14–15 The skin in pedicled skin flaps and free skin flaps used routinely in clinical practice are quite different from the skin overlying the finger pulp in texture and nerve distribution and cannot restore its sensation and wear resistance. Therefore, currently, it is best to use a lateral flap from the toe or finger to repair finger pulp defects.16–19 Owing to the great difficulty of operation, significant trauma and high probability of failure, some patients are unwilling to accept a free toe lateral skin flap. When the finger pulp defect is combined with severe injury to the proximal and middle phalanges of the finger or with vascular injury, inflammatory oedema and poor skin condition, local island flaps and free flaps cannot be used for repair. When the finger pulp defect extends past the distal interphalangeal joint, an island flap of the digital artery of the same finger cannot be used for repair because of damage to the distal digital artery arch. The vascular pedicle of an island flap of the adjacent finger artery must be separated to the common digital artery. The resulting large incision leaves the palm with a large scar, which easily results in scar contracture. 20
It has been reported that bridge transfer of a digital artery retrograde island flap was used to repair an adjacent finger defect; however, additional rectangular flaps were designed at the vascular pedicle.21–23 This vascular pedicle treatment can waste finger skin. Zhang et al. and Zhang et al.24–25 repaired skin and soft tissue defects of the leg with free skin flap bridge transfer. The vascular pedicle of the free skin flap was exposed and anastomosed to the posterior tibial artery of the contralateral leg, and the exposed vascular pedicle was covered with a reticular skin graft. This dramatically simplifies the operation, saves the amount of skin used in the leg and the legs can be placed parallel, which is a comfortable postoperative position. Additionally, all flaps survived in both studies, which eliminated concern regarding vascular crisis caused by the exposed vascular pedicle. Owing to the small area of the lateral flap of the finger, to reduce the damage to the donor area, we exposed the finger artery pedicle of the flap and covered it with a skin flap. This method does not require incising the skin on the side of the finger to make a skin tube to wrap the vascular pedicle and can significantly reduce trauma to the donor finger. This approach is also simple and shortens the operation time. Compared with the conventional island flap of the adjacent digital artery, which must be separated from the common digital artery, our procedure requires a secondary pedicle amputation. However, this approach causes no collateral damage to the palm. In addition, the flap has a large contact area with the donor site, and the blood supply is reliable. The pedicle can be severed easily and in advance without suturing or with only 1 to 2 sutures, and the shape is beautiful.26–27
Strengths and limitations
The strengths and limitations of this surgical method are shown in Table 3. In this study, retrograde island flap bridge transfer of the adjacent finger artery combined with a vascular pedicle tubular skin graft was used to repair finger pulp defects. This method has the following advantages: 1. The donor area is concealed, and the texture of the skin flap is close to that of the recipient area. The dorsal branch of the digital nerve can be carried to anastomose to the proper digital nerve of the recipient area. The appearance of the flap is beautiful after repair, and sensation in the finger pulp can be restored. 2. The flap contains the main finger artery, which is a reliable blood supply and is associated with fast wound healing. Additionally, the flap can be cut to obtain a longer vessel pedicle. Postoperatively, the flap is easy to care for, the patient's hand and finger position is comfortable and flexion and extension exercises can begin early after surgery. 3. The operation is performed in the same surgical field, with simple procedures and with no need for vascular anastomosis. Additionally, the postoperative success rate in this study was high. 4. The flap pedicle is narrow, the pedicle is easy to sever, the contact area is large and the pedicle can be severed in advance. 5. There is no damage to the proximally injured tissue of the finger, and the flap will not cause necrosis of the skin and soft tissue of the finger or necrosis of the finger itself because of new trauma. 6. Compared with other island flaps, the injured finger has no open subcutaneous tunnel, and the scar is small. However, this technique also has some shortcomings: 1. The flap is cut in a small area and can be used to repair only two finger-pulp defects simultaneously. 2. It is necessary to sacrifice the digital artery on one side of the finger in the donor area. To restore sensation in the flap, it is necessary to carry the dorsal branch of the digital nerve, and sensation on the side of the donor finger may decrease postoperatively, as a result.
Strengths and limitations of retrograde island flap bridge transfer of the adjacent phalangeal artery combined with vascular pedicle tubular skin grafting.

Precautions for surgery and postoperative management
We should pay attention to the following points when using this surgical procedure: 1. The pedicle of the finger artery in the skin flap should carry a fascia pedicle measuring approximately 0.5 cm to 1.0 cm to facilitate venous return and pedicle skin grafting while avoiding vascular spasms caused by arterial injury. 2. Do not twist the pedicle when the flap is transferred and cover the vascular pedicle with a thin layer of skin during skin grafting. Additionally, suture with fine nylon suture to avoid damage to the vascular pedicle. 3. Do not transfer the proper finger nerve with the skin flap to avoid damaging the function of the donor finger nerve.
In summary, in this study, we used a retrograde island flap bridge transfer of the adjacent finger artery combined with a vascular pedicle tubular skin graft to repair finger pulp defects and achieved good results. This is a safe and effective operation. The flap has the advantages that it is simple to sever the flap, the flap has good texture and the donor area is concealed, which is convenient for early functional exercise of the finger, postoperatively.
Footnotes
Author contributions
Weibin Du and HeLou Zhang collected the data and wrote the manuscript. Weibin Du, Fangbing Zhu and HeLou Zhang were major contributors to writing the manuscript. Jun Yang, Wei Zhuang and Qiao Hou contributed to the conception and design of the study. All authors read and approved the final manuscript.
Declaration of competing interests
All the authors declare that they have no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the National Natural Science Foundation of China (NO. 81904053), the Medical and Health Science and Technology Project of Zhejiang Province (NO. 2020KY797) and the Major Science and Technology Program for Social Development of Xiaoshan District, Hangzhou (NO. 11216, 2019318).
Supplemental material
Supplemental material for this article is available online.