
Abstract
The treatment strategy for an idiopathic retroperitoneal mass has not yet been established. Additionally, differentiating between benign and malignant is a challenge. Herein, we report a case in which we performed partial resection of a mass in a symptomatic patient with idiopathic retroperitoneal fibrosis that mimicked malignancy. A 44-year-old woman with an unremarkable medical history other than gallstones presented with a 1-month history of abdominal pain and repetitive vomiting. Imaging studies identified a large, retroperitoneal mass compressing the duodenum that had grown acutely over the preceding 2 weeks. The possibility that the mass was malignant could not be excluded. Considering the invasiveness and potential curability, we performed partial resection of the mass, which involved partial colonic resection with reconstruction, to allow for pathological diagnosis and intestinal obstruction treatment. The final pathological findings revealed that the mass consisted of hemorrhagic and fibrotic tissue without a tumorous component. The patient’s postoperative course was unremarkable. She is alive 8 years postoperatively with no recurrence. In conclusion, a surgical approach, including biopsies, to idiopathic retroperitoneal fibrosis that mimics malignancy should be actively considered in symptomatic patients. Decisions regarding the required degree of surgical intervention call for sufficient, case-specific discussion.
Keywords
Introduction
Idiopathic retroperitoneal fibrosis (IRF) is a rare condition of unknown etiology that is characterized by non-specific, non-suppurative desmoplastic retroperitoneal inflammation. Although malignant retroperitoneal fibrosis accounts for up to 8% of IRF cases, its clinical diagnosis remains challenging despite advancements in imaging modalities. 1 In this report, we describe a case of IRF with extensive retroperitoneal infiltration that mimicked malignancy and required surgery for diagnosis. This case report was written in accordance with the CARE guidelines. 2
Case Report
A 44-year-old Japanese woman with a history of gallstones that were identified during a medical checkup, periodically received cholecystic monitoring at a neighboring hospital. She presented to the hospital with a 1-month history of continuous abdominal pain, loss of appetite, and repeated episodes of vomiting. She had never smoked. Contrast-enhanced computed tomography (CT) demonstrated an 8.3 cm × 7.0 cm mass with marginal enhancement that was compressing the second and third parts of the duodenum and, consequently, causing gastric dilatation. The mass was not near the aorta. The right ureter was located behind the retroperitoneal mass but was not closely adjacent. A regional increase in the mesenteric fat density around the mass was also observed (Figure 1). The signal intensity inside the lesion was consistent with blood. Magnetic resonance cholangiopancreatography performed 2 weeks prior as part of the cholecystolithiasis examination had not detected this lesion. She was subsequently referred to our institution for further evaluation and management of the abdominal mass.
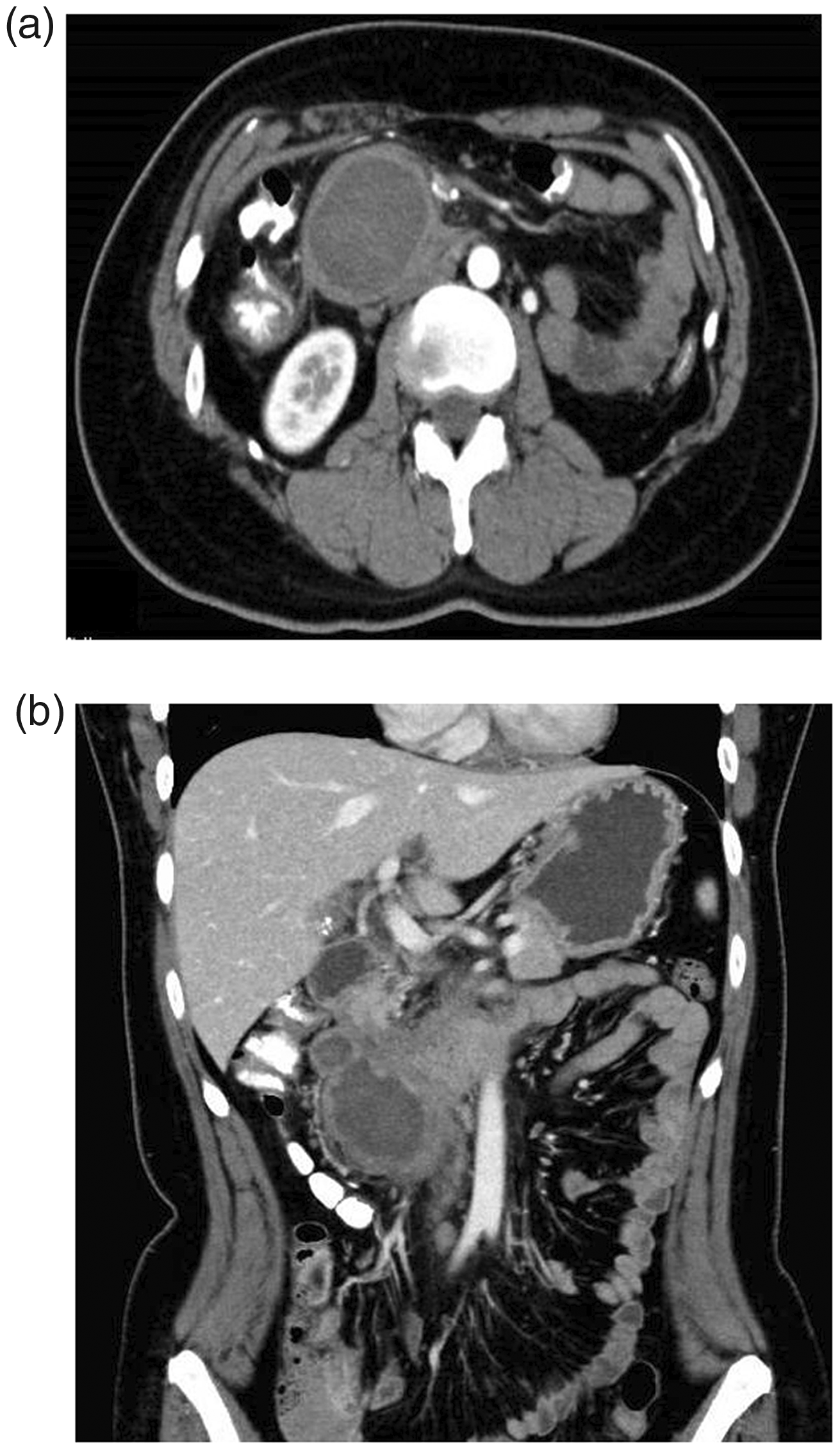
Abdominal computed tomography images demonstrating a solid, retroperitoneal mass that was causing digestive obstruction. The mass was compressing the second and third parts of the duodenum and, consequently, causing gastric dilatation. The mass was not near the aorta. (a) Axial and (b) Coronal images.
The serum tumor markers, carcinoembryonic antigen and carbohydrate antigen 19-9, were within their normal ranges. The C-reactive protein level was 1.9 mg/L, and renal function was normal. On esophagogastroduodenoscopy, a stricture was found 3 cm to the anal side of the papilla of Vater that was caused by extraluminal compression of the digestive tract; there was no tumor exposure. This finding suggested that the mass was not an epithelium-derived tumor. Expanding mesenchymal neoplasms, including malignancies with high hemorrhagic potential, were included in the differential diagnosis. Regarding the intervention, we opted for surgical resection to allow for pathological diagnosis and treatment of potential intestinal obstruction. Regarding the surgical strategy, simple tumor resection was considered the adequate and less invasive method, if feasible. Pancreaticoduodenectomy was considered the most invasive option and was only to be performed if R0 resection could be achieved.
Laparotomy was performed. The mass was recognized as a tense, elastically hard tumor that was accompanied by several, nodule-like, daughter indurations involving the ligament of Treitz. These findings led to the diagnosis of malignancy, despite the fact that the intraoperative frozen section examination failed to exhibit any tumorous components. The superior mesenteric plexus appeared to have stiffened, which implied tumorous invasion. Moreover, the mass appeared to have closely invaded the papilla of Vater and infiltrated the second part of the duodenum and transverse mesocolon. When considering all of these findings, R0 resection did not seem feasible, even by performing pancreaticoduodenectomy. A decision to conduct mass reduction surgery was made, considering the need to prevent bleeding and relieve digestive tract obstruction.
After ileocecal vessel and accessory right colic vein ligation was performed, the infiltrated sections of the ileum and the transverse colon were removed. The duodenum was also resected at the anal side of the papilla of Vater, despite the procedure resulting in leaving some components of the mass where it had infiltrated the second part of the duodenum. The mass was resected with the right hemicolon. Reconstruction was then performed, as follows: duodenojejunostomy, gastrojejunostomy, Braun anastomosis, and ileotransversostomy (Figures 2 and 3). The operation time was 436 minutes, and the total amount of blood lost was 2281 mL.
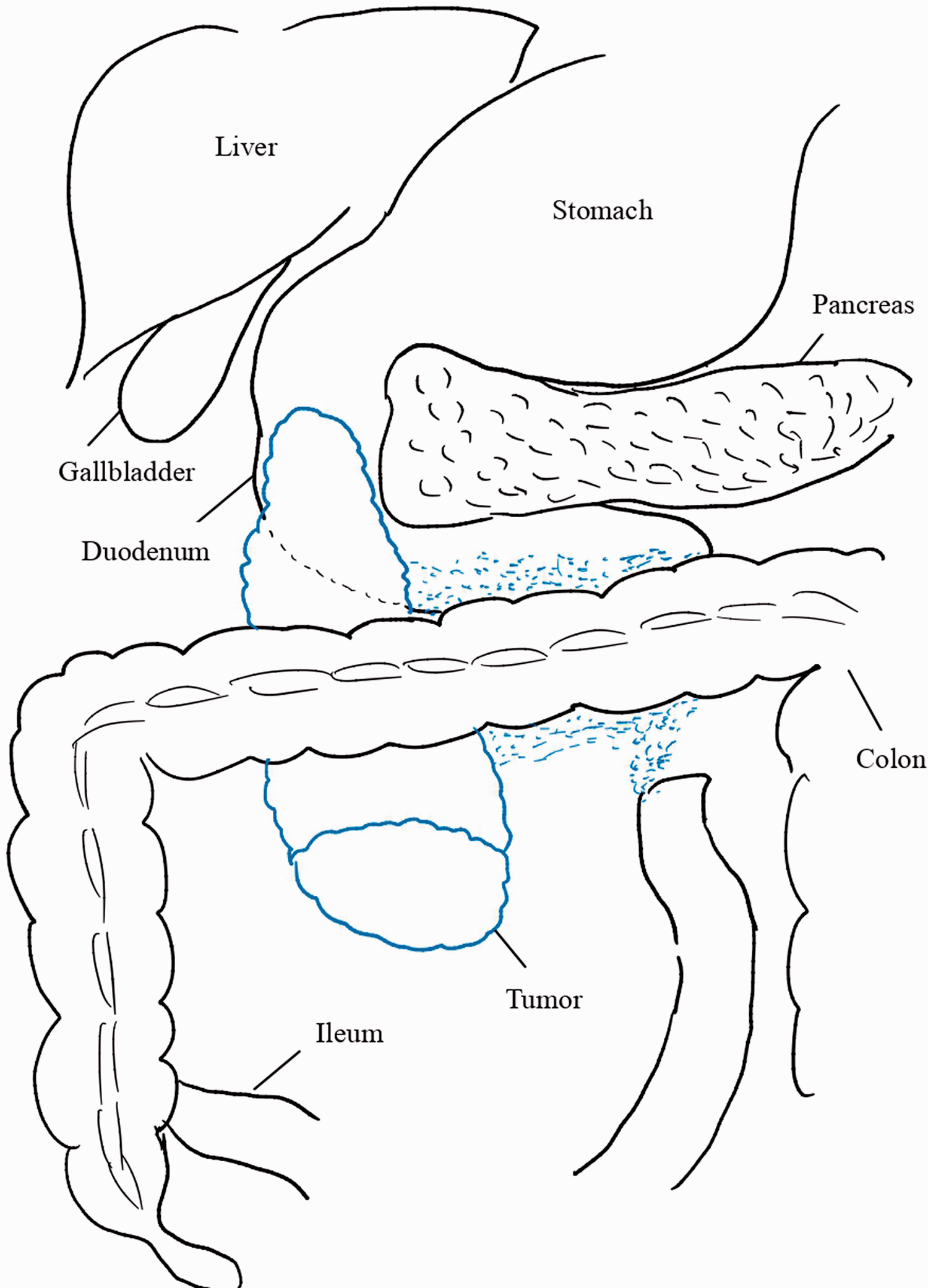
Schema demonstrating the retroperitoneal mass location. The mass (outlined in blue) appeared to invade the papilla of Vater, the second part of the duodenum, and the transverse mesocolon. The small blue dashes indicate several nodule-like, daughter indurations involving the ligament of Treitz.

Schema of the reconstruction. Duodenojejunostomy was followed by gastrojejunostomy, Braun anastomosis, and ileotransversostomy.
Histopathological examination of the resected specimen showed that the retroperitoneal mass consisted of hemorrhagic and fibrotic components on the serosal side of the colon, with no tumor cells. This non-tumorous lesion, which was mainly located in the subserosal layer, had a cavity that contained blood clots. Immunohistochemically, the myofibroblasts in the mass were positive for α-smooth muscle actin, and negative for β-catenin and S100. Elastica van Gieson staining showed no vascular disruption. The mass was thought to have originated from acute hemorrhage that developed in the preceding chronic fibrotic lesion as the intralesional fibrotic components were deemed vestigial histologically (Figure 4).

Pathological findings from the resected specimen. Fibrotic tissue with inflammatory cell infiltrates is seen in the subserosal adipose tissue. Infiltrating inflammatory cells are mainly histiocytes and small lymphocytes, with no plasma cells. No neoplastic change is identified (hematoxylin and eosin staining; ×4).
The postsurgical course was uneventful. To date, 8 years of postoperative outpatient surveillance, comprising esophagogastroduodenoscopy and contrast-enhanced CT, have revealed no evidence of recurrence of the mass-forming disease.
The final diagnosis was idiopathic retroperitoneal fibrosis.
Discussion
IRF was first reported in 1905 by Albarrán, a French urologist. 3 IRF is a rare disease, the etiology of which has yet to be clearly determined. Approximately two-thirds of retroperitoneal fibrosis cases are considered idiopathic with no known triggerable factors, while the etiologies of other cases are ascribed to drugs, malignant diseases, infection, or past surgical interventions.3,4 In this case, the patient had an unremarkable medical history other than gallstones, for which she was not receiving medication. In the majority of patients with IRF, the levels of acute-phase reactants, such as erythrocyte sedimentation rate and C-reactive protein, are reportedly increased. 5 Additionally, some patients with IRF do not have elevated acute-phase reactant levels, 5 as in the present case. Acute-phase reactant levels are routinely used to monitor disease activity; 5 however, Pelkmans et al. insisted that neither acute-phase reactant levels nor their initial changes is a major predictor for treatment success. 5 In the present case, the mass consisted mainly of hemorrhagic and fibrotic components, which may imply that the patient’s symptoms were related more to anatomical extension of the mass than intense inflammation, as normal C-reactive protein levels can indicate.
IRF is typically characterized by the formation of dense fibrotic tissue plaques that can extend from the pelvis to the renal pedicles and ureters. 6 Thus, this disease commonly manifests as ureteric obstruction in addition to non-specific symptoms, such as abdominal or back pain and weight loss. However, duodenal involvement is extremely rare. To the best of our knowledge, only 11 cases of retroperitoneal fibrosis that caused duodenal stenosis have been reported.7 –17 In most cases, the provisional diagnosis was solely based on the radiological findings and clinical manifestations. Of the 11 cases, 4 were successfully treated with corticosteroids without surgical intervention.8,13 –15 Another four patients improved with surgery only,11,12,16,17 and both surgery and corticosteroid administration were performed for two patients, although one died suddenly after discharge.9,10 One patient received no treatment because of death due to acute myocardial infarction. 7 In the current case, the unbearable clinical manifestations of duodenal stenosis, the possibility of malignancy, and the extremely rapid growth of the mass, presumably owing to intra-mass hemorrhage, justified the surgical strategy. There was consistent suspicion that the mass was malignant both pre- and intraoperatively. To date, the patient has been clinically well and has not received corticosteroid therapy. This suggests that surgical resection with a sufficient margin can potentially inhibit chronic inflammation and fibrotic tissue maturation in IRF.
If the clinical symptoms are not severe or the tumor-like growth is not acute, as was the case with our patient, exploratory laparotomy may be useful in making a final diagnosis. 6 Amis et al. stressed the importance of multiple deep surgical biopsies to completely rule out malignancy; 4 however, performing multiple biopsies in the retroperitoneal area may be accompanied by unfavorable morbidity.
It should be noted that acute intra-mass hemorrhage associated with chronic fibrosis can mimic infiltrative malignancy. Cronin et al. suggested that CT and magnetic resonance imaging poorly differentiate benign from malignant causes of retroperitoneal masses. 18 This may indicate that surgical biopsy, including surgical resection, should be actively considered for the pathological diagnosis and alleviation of symptoms in symptomatic patients, unless the retroperitoneal mass can be proven to be benign. Concurrently, sufficient discussion of the surgical strategy is of great importance. In our case, pancreaticoduodenectomy would have been considered excessively invasive. However, following patients without an invasive strategy can only be justified if patients are asymptomatic.
Recently, several studies have reported the importance of postoperative continuous monitoring in patients with IRF.19,20 Our case is categorized into the low-risk group in accordance with the criteria advocated by Moriconi et al. 20 Nonetheless, the 15-year cumulative incidence rate of IRF recurrence was estimated to be as high as 48% in a previous study. 19 Therefore, we will continue periodic surveillance for our patient.
In conclusion, our case is of remarkable pedagogical value in terms of the insight it provides into clinical decision-making regarding retroperitoneal masses that mimic infiltrative malignancy in symptomatic patients.
Footnotes
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics statement
The need to obtain ethics approval was waived because this study is a case report, and the manuscript contains no photographs or identifiable information. Written consent for treatment was obtained from the patient. Written consent to publish the case information was obtained from the patient.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.