
Abstract
Objectives
This study aimed to investigate the prognostic value of serum prealbumin, N-terminal pro-B-type natriuretic peptide (NT-proBNP), heart type fatty acid binding protein (hFABP), and cardiac troponin I (cTnI) for heart failure and cardiac death in elderly patients.
Methods
We studied 426 consecutive patients with New York Heart Association classes I to IV who were recruited between February 2014 and 2018. Cardiac mortality was the primary end point. Receiver operator characteristic curves were created to analyze predictive values.
Results
When prealbumin, NT-proBNP, hFABP, and cTnI were combined, the areas under the receiver operator characteristic curve reached 0.930 and 0.903 for heart failure and cardiac death, respectively. Prealbumin, NT-proBNP, hFABP, and cTnI levels changed differently during therapy in patients in different prognosis groups. These parameters improved in patients who did not develop major adverse cardiovascular events (MACEs), but were unchanged or deteriorated in patients with MACEs. Multivariate Cox regression analysis showed that these parameters were significant independent risk factors for MACEs and cardiac death.
Conclusions
Our study shows that serum prealbumin, NT-proBNP, hFABP, and cTnI levels are significant prognostic factors for elderly patients with poor cardiac function. These parameters are more accurate for prognosis when used together.
Keywords
Introduction
Severe heart failure (HF) is a terminal illness of patients with heart disease and is the main cause of cardiac death in up to 40% of patients. 1 This rate is even higher in elderly patients with New York Heart Association (NYHA) functional classes III and IV where the cardiac death rate could be >70%.2,3 Timely diagnosis and treatment for HF are important for reducing the mortality rate and improving prognosis. One approach is to use biomarkers to predict the prognosis of HF. 4 However, the diagnosis and evaluation of disease severity for HF are still clinically challenging. In recent years, a number of biomarkers have been proposed to assist in diagnosis of HF.5,6 An example of one of these biomarkers is N-terminal pro-B-type natriuretic peptide (NT-proBNP), which is a useful indicator for estimating the prognosis of HF. 5 NT-proBNP levels are also elevated when myocardial ischemia occurs in patients with HF. 7
The progress of cardiac disease is associated with many factors, such as reduced nutritional intake, increased degenerative metabolism, reduced liver function, and chronic inflammation. 8 Therefore, a multiple biomarker approach is likely to provide better diagnosis and prognosis for HF. Prealbumin is mostly synthesized in the liver and is a tetrameric protein with a molecular weight of 54 kDa 9 and a half-life of approximately 2 days. Prealbumin has been proposed as a biomarker for impaired nutritional status that has a risk for surgical site infection. 10 This protein is also a sensitive and early indicator of nutritional conditions compared with other widely used indicators, such as serum albumin, total cholesterol, and the lymphocyte count. 11 NT-proBNP is a cardiac natriuretic hormone that regulates heart function. When HF occurs, there is profound activation of ventricular synthesis of NT-proBNP. 12 Fatty acid binding protein (FABP) is a 15-kDa protein consisting of 132 amino acids. 13 Heart type fatty acid binding protein (hFABP) belongs to the FABP superfamily and is located primarily in the heart, and it constitutes 5% to 15% of the cytosolic protein pool 14 where it transports fatty acids to mitochondria for ß-oxidation and energy expenditure. 15 Cardiac troponin I (cTnI) is the molecular switch of the sarcomere and is related to relaxation performance in cardiac myocytes.16,17
In this study, we evaluated the combined prognostic value of prealbumin, NT-proBNP, hFABP, and cTnI for HF in elderly patients who are hospitalized because of chronic HF. Our findings could help evaluate and stratify the severity and risk of death in patients with HF and provide monitoring tools for treatment of this disease.
Materials and methods
Patients
Elderly patients with HF who were treated in our hospital owing to worsening of chronic HF between February 2014 and 2018 were studied. Patients were included if they were diagnosed with HF in accordance with the national guidelines 18 and aged between 65 to 91 years. Patients were excluded if they had a tumor, severe respiratory diseases, surgery involving the heart or brain, and mental disorders. Included patients were assessed for the NYHA functional class 19 at admission and further grouped on the basis of primary outcome into the non-major adverse cardiovascular event (MACE) or MACE group. Patients were treated according to the national guidelines. 18 Drugs including diuretics (e.g., bumetanide, metolazone, and tolvaptan), renin and angiotensin system inhibitors (e.g., the angiotensin-converting enzyme inhibitor drugs benazepril and captopril and the angiotensin II receptor blocker drugs azilsartan, eprosartan, and losartan), and β receptor blockers (e.g., acebutolol and bisoprolol) were used for treatment. The MACE group included patients with readmission, cardiovascular mortality, non-fatal myocardial infarction, and non-fatal stroke. The primary end point was cardiovascular mortality.
Demographic and clinical data, including age, sex, underlying diseases, and laboratory findings were collected. The study complied with the Declaration of Helsinki and was approved by the institutional ethics committee of the First Affiliated Hospital of Huzhou University, Huzhou, China (approval number: HUE2013-84). Written informed consent was received from all patients.
Biochemical measurements
Fasting venous blood was drawn from patients within 24 hours after admission and during the hospitalization and treatment periods. Prealbumin, NT-proBNP, hFABP, and cTnI levels were determined using enzyme-linked immunosorbent assays with commercial kits purchased from Ruilai Bioeng (Beijing, China). The assays were carried out in triplicate according to the manufacturer’s instructions on an ARCHITECT c16000 Clinical Chemistry Analyzer (Abbott, Abbott Park, IL, USA). The detection limit, coefficients of variation, and normal limits for NT-proBNP, hFABP, and cTnI levels were as follows: 3 pg/mL, 5%, and 4000 pg/mL; 1.25 ng/mL, 4%, and 1000 ng/mL; and 25 fg/mL, 4%, and 100 fg/mL; respectively.
Follow-up and determination of MACEs
All patients were followed up for 180 days starting from admission. Follow-up was performed through a telephone interview and hospital visit during initial hospitalization and readmission. MACEs were recorded during the visit. MACEs were defined as cardiovascular mortality, recurrent myocardial ischemia, acute myocardial infarction, deterioration of HF, non-fatal myocardial infarction and non-fatal stroke, and readmission due to severe arrhythmia.
Statistical analysis
The data were analyzed by SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA). The normality of distribution of continuous variables was tested by the one-sample Kolmogorov–Smirnov test. Continuous variables with a normal distribution are presented as mean ± standard deviation and non-normal variables are reported as median (interquartile range). Means of two continuous normally distributed variables were compared by the independent samples Student’s t test. Receiver operator characteristic (ROC) curves were created to analyze the prognostic values of biomarkers for HF. Survival curves were calculated using the Kaplan–Meier method and compared by the log-rank test according to univariate analysis. Multivariate Cox regression analysis was used to analyze the factors affecting MACEs, death, and readmission for patients with HF. A P value <0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 426 patients were included in this study, with 190 men and 236 women with a mean (± standard deviation) age of 73.6 ± 18.2 years. Among them, 146 and 280 patients were assessed as having NYHA classes I to II and classes III to IV, respectively. There were no differences in age, sex, body mass index, systolic blood pressure, diastolic blood pressure, heart rate, estimated glomerular filtration rate, and left ventricular ejection fraction between the two groups (Table 1). The percentages of patients with myocardial infarction, hypertension, and diabetes mellitus were also similar between the two groups. However, in NYHA classes III to IV, there were significantly higher rates of patients with newly diagnosed HF, HF with preserved ejection fraction, atrial fibrillation, and stroke compared with those in patients with NYHA classes I to II (all P < 0.05, Table 1).
Baseline characteristics of the patients (n = 426).
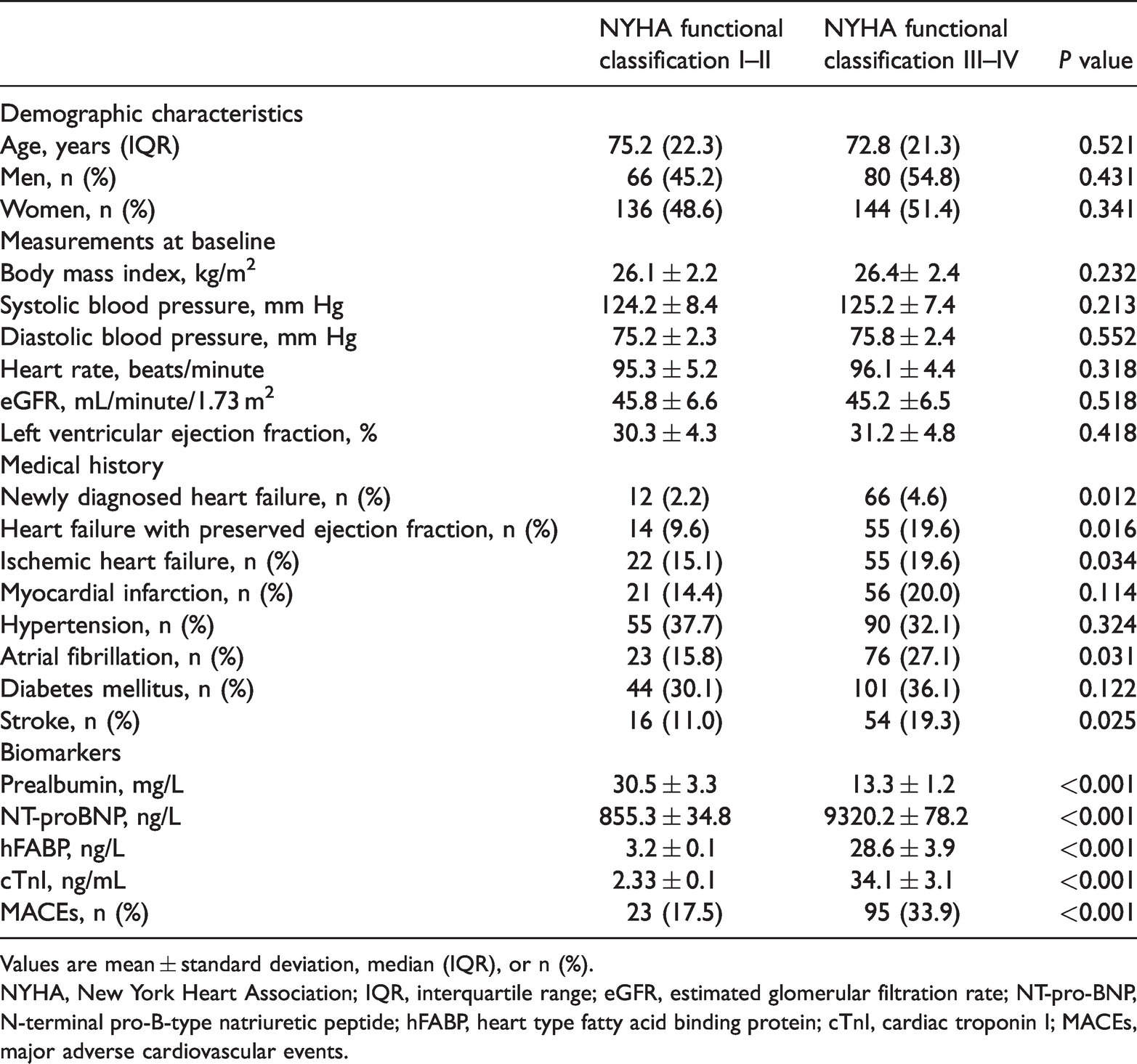
Values are mean ± standard deviation, median (IQR), or n (%).
NYHA, New York Heart Association; IQR, interquartile range; eGFR, estimated glomerular filtration rate; NT-pro-BNP, N-terminal pro-B-type natriuretic peptide; hFABP, heart type fatty acid binding protein; cTnI, cardiac troponin I; MACEs, major adverse cardiovascular events.
Associations of prealbumin, NT-proBNP, hFABP, and cTnI levels with NYHA class
Patients with NYHA classes III to IV had significantly lower prealbumin levels and significantly higher NT-proBNP, hFABP, and cTnI levels compared with patients with NYHA classes I to II (all P < 0.001, Table 1). Furthermore, the rate of MACEs was significantly higher in the NYHA III to IV group than in the NYHA I to II group (P < 0.001, Table 1). MACEs were negatively correlated with prealbumin levels (r = −0.89, P < 0.05) and positively correlated with NT-proBNP, hFABP, and cTnI level (r = 0.89, 0.91, and 0.62, respectively, all P < 0.05).
ROC curve analysis and risk stratification
ROC curve analysis showed that the area under the curves (AUCs) of prealbumin, NT-proBNP, hFABP, and cTnI for predicting readmission for HF were 0.822 (P = 0.015), 0.901 (P = 0.011), 0.818 (P = 0.022), and 0.650 (P = 0.031), respectively (Figure 1a). The sensitivity and specificity of prediction were highest with NT-proBNP and hFABP alone. Use of all markers (prealbumin, NT-proBNP, hFABP, and cTnI) increased the sensitivity and specificity to 95.0% and 95.6%, respectively, with an AUC of 0.930 (P = 0.009, Table 2). For cardiac death, the AUCs were 0.662, 0.672, 0.721, and 0.613 for these biomarkers (Figure 1b). The sensitivity was high with NT-proBNP and sensitivity and specificity were high with hFABP in single biomarker assessment (Table 2). When these biomarkers were combined, the specificity and specificity increased to 93.9% and 91.4%, respectively (Table 2), and the AUC was significantly higher than that for single parameters (all P < 0.05, Table 2). When the cutoffs were used to stratify mortality, the survival rate was significantly higher when prealbumin levels were ≥2.24 µmol/L, NT-proBNP levels were <6335.1 ng/L, hFABP levels were <6335.1 ng/L, and cTnI levels were <3.08 ng/mL (Figure 2a–d). Patients with HF and high cTnI levels had a significantly higher mortality rate than those with low cTnI levels (33.8% vs 12.7%, P < 0.05).

Receiver operator characteristic curves for prealbumin, NT-proBNP, hFABP, and cTnI-based prediction in elderly patients for prognosis of heart failure (a) and cardiac death (b).
Comparison of prognostic value of serum prealbumin, NT-proBNP, hFABP, and cTnI levels for cardiac death and HF.

Data followed by the same letter in the same column are not significantly different at P < 0.05.
AUC, area under the curve; HF, heart failure; NT-proBNP, N-terminal pro-B-type natriuretic peptide; hFABP, heart type fatty acid binding protein; cTnI, cardiac troponin I.

Kaplan–Meier survival curves for patients with heart failure stratified with the cutoff values of prealbumin (a), NT-proBNP (b), hFABP (c), and cTnI (d).
Changes in prealbumin, NT-proBNP, hFABP, and cTnI levels during treatment
Before treatment, prealbumin levels were significantly lower, and NT-proBNP, H-FABP, and cTnI levels were significantly higher in the MACE group (including the readmission group and cardiac death group shown in Table 3) than in the non-MACE group (all P < 0.05). Additionally, prealbumin levels were significantly lower, and NT-proBNP, H-FABP, and cTnI levels were significantly higher in the cardiac death group than in the readmission group (all P < 0.05) (Table 3).
Changes in prealbumin, NT-proBNP, hFABP, and cTnI levels during the treatment period.
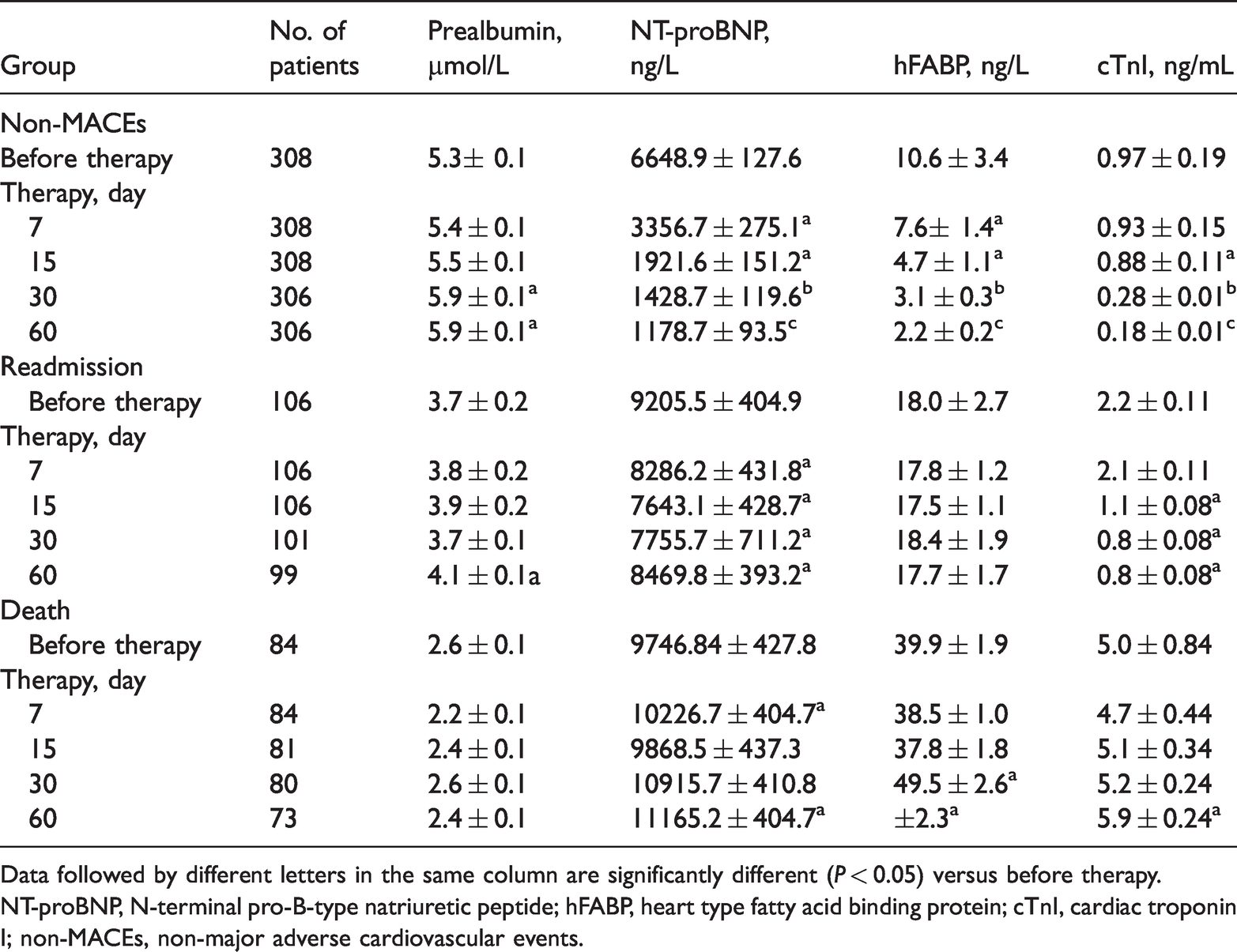
Data followed by different letters in the same column are significantly different (P < 0.05) versus before therapy.
NT-proBNP, N-terminal pro-B-type natriuretic peptide; hFABP, heart type fatty acid binding protein; cTnI, cardiac troponin I; non-MACEs, non-major adverse cardiovascular events.
For patients in the non-MACE group, NT-proBNP, hFABP, and cTnI levels significantly decreased (all P < 0.05), while prealbumin levels remained unchanged during the first 2 weeks of treatment. Prealbumin levels were significantly increased after treatment for 30 days, while NT-proBNP, hFABP and cTnI levels continued to decrease (all P < 0.05, Table 3). For patients in the readmission group, prealbumin and hFABP levels remained relatively stable during 60 days of treatment, but NT-proBNP and cTnI levels tended to decrease, although this reduction appeared to occur mostly with 15 days of treatment and did not increase thereafter. In the cardiac death group, prealbumin levels were relatively stable during the treatment period, but the remaining three parameters tended to increase, particularly after treatment for 30 days (Table 3).
Multivariate Cox regression analysis
The factors affecting MACEs, death, and readmission for patients with HF were analyzed using multivariate Cox regression analysis with all four biomarkers and the left ventricular ejection fraction as independent variables. We found that prealbumin, NT-proBNP, hFABP, and cTnI were significant risk factors for MACEs and death (all P < 0.05), but not readmission. The left ventricular ejection fraction was not associated with these outcomes (Table 4).
Multivariate Cox regression analysis of the factors associated with MACEs, readmission, and cardiac death in patients with heart failure

MACEs, non-major adverse cardiovascular events; SE, standard error; OR, odds ratio; CI, confidence interval; NT-proBNP, N-terminal pro-B-type natriuretic peptide; hFABP, heart type fatty acid binding protein; cTnI, cardiac troponin I; LVEF, left ventricular ejection fraction.
Discussion
HF is a complex clinical syndrome, which is rarely characterized using single biochemical markers for its clinical and pathophysiological characteristics. 20 Except for NT-proBNP/B-type natriuretic peptide, which is widely used in diagnosing acute HF,21,22 no other biomarkers have been widely accepted as significant indicators for diagnosis and treatment of HF. A recent study showed that in chronic HF, myocardial injury may occur because of inflammation or deprivation of nutrition, particularly in elderly patients. 23 Therefore, prealbumin, as well as NT-proBNP, hFABP, and cTnI levels, were assessed for their value in prognosis of patients with HF in this study.
Our study showed that prealbumin levels were lower, and NT-proBNP, hFABP, and cTnI levels were higher in patients with a high NYHA functional class, which indicated that these parameters were important for the prognosis of HF. Prealbumin is a negative acute-phase reactant, and its synthesis is inhibited in an inflammatory environment. Because of the shorter half-time of prealbumin than albumin, it can be used to estimate nutrition and the inflammatory state of patients more accurately than serum albumin (ranges from <35 g/L in patients with hypoalbuminemia to >45 g/L in healthy individuals). Low prealbumin levels are associated with poorer overall survival and disease-free survival in patients with advanced gastric cancer.24,25 Furthermore, patients with HF and low prealbumin levels at discharge are associated with high short-term mortality 26 and decreased admission serum albumin levels are associated with high long-term mortality in hospital survivors of acute myocardial infarction. 27 These results are consistent with our observations, indicating that prealbumin is a reliable indicator for the prognosis of HF.
NT-proBNP was originally isolated from porcine brain extracts and is a cardiac natriuretic hormone. Together with the highly homologous atrial natriuretic peptide, NT-proBNP forms a dual natriuretic peptide system of the heart. In HF, secretion of B-type natriuretic peptide is stimulated owing to increased wall stretch, neurohormonal activation, and hypoxia. In the normal condition, the atrium is the main cardiac production site, but as HF develops, there is profound activation of ventricular NT-proBNP synthesis. 12 Therefore, serum NT-proBNP levels can sensitively reflect changes in ventricular pressure and load capacity, and they increase with increasing severity of HF. 28
In healthy humans, the normal range of hFABP levels in serum or plasma is <5 ng/mL.29,30 The diagnostic value of hFABP has been assessed comprehensively in patients suffering from acute myocardial infarction with varying diagnostic areas under ROC curves.31,32 However, hFABP sometimes generates conflicting results when combined with cTnI for early diagnosis of acute myocardial infarction.33,34 cTnI has reliable accuracy for early diagnosis of acute myocardial infarction with an AUC of 0.95.35,36 Levels of cTnI are frequently elevated in patients with HF and can be an indicator for high mortality in emergency departments. 37 Additionally, circulating cTn levels are highly specific for measuring myocardial damage 38 and are associated with acute and advanced chronic HF.39,40 High hFABP and cTnI levels in patients with a high NYHA functional class and HF in our study suggested that there might be more myocardial cell injury or progressive necrosis, which is consistent with a previous report. 41
ROC curve analysis showed that the AUCs based on the four parameters for mortality were > 0.5, which indicated that they might have prognostic value for HF. For prognosis of HF, NT-proBNP had the highest prognostic value (AUC = 0.901) followed by prealbumin, hFABP, and cTnI. For prognosis of mortality, hFABP had the highest AUC of 0.721, followed by NT-proBNP, prealbumin, and cTnI. These results are consistent with previous reports.42,43 However, when these four parameters were used together, the diagnostic accuracy significantly improved compared with single biomarkers. Additionally, the AUC reached 0.903 for mortality of HF and the specificity and specificity increased to 95.0% and 95.6% for HF and to 93.9% and 91.4% for mortality, respectively. These findings indicated that the multimarker approach increases prognostic reliability for elderly patients with HF. A combination of uric acid and NT-ProBNP was shown to be a better prognostic marker for short-term clinical outcomes in patients with acute HF. 42 Multimarker strategy is essential for accurate prediction of cardiac death in patients with acutely decompensated chronic HF. 44
In the current study, when these cutoffs were used to stratify risk, Kaplan–Meier survival curve analysis showed that the survival probability was high when prealbumin levels were above and other parameter levels were below the cutoff values. This finding suggests that these measurements can be used as objective indicators of risk stratification in patients with HF. Furthermore, multivariate Cox regression analysis showed that the four parameters were significant risk factors for MACEs and death. Levels of cTnI can be detected in the blood of patients with HF. Even when cTnI levels are within the normal range, their detection is an indication of a poor prognosis of patients, particularly if serum cardiac troponin T levels are persistently high, despite conventional treatment. 45 This finding is probably due to ongoing subclinical degeneration of myocytes associated with deterioration of the patients’ clinical status. In our study, patients with HF and high cTnI levels had a significantly higher mortality rate than those with low cTnI levels (33.8% vs 12.7%, P < 0.05). This finding is consistent with a previous study. 46
In this study, we measured prealbumin, NT-ProBNP, hFABP, and cTnI levels before and after treatment. We found that changes in these levels were different among patients with a different prognosis. In the non-MACE group, levels of these four parameters improved as the treatment time increased. However, in patients in the readmission and cardiac death groups, these levels deteriorated or remained unchanged over the treatment period. These findings were particularly remarkable for NT-proBNP and cTnI levels. Therefore, these parameters can be used to predict the progress of therapy. This finding is also in line with previous studies that showed that persistently increased serum cardiac troponin levels in patients with acute HF are predictive of adverse outcomes. 47 Therefore, patients should be monitored continuously during the therapy period for better management of HF.
Conclusion
Our study shows that serum prealbumin, NT-proBNP, hFABP, and cTnI levels are significant predictors for prognosis of elderly patients with HF and poor cardiac function, and are more accurate when used in combination. These parameters can be used to judge the severity of HF and monitor therapeutic progress for better management of HF.
Footnotes
Availability of data and material
The datasets used during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
KL and GC designed the study. KL and SG collected the data and performed analysis. SW analyzed the data and revised the manuscript. KL and GC drafted the manuscript. All authors read and approved the final manuscript.