
Abstract
We present a case of a 34-year-old man who was admitted to our hospital with a six-month history of nausea and vomiting that had worsened over the past two weeks. Diagnosis of primary hyperparathyroidism (PHPT) due to a single parathyroid adenoma was confirmed by laboratory results and imaging but following pharmacological therapy the patient developed a dry cough. Single-photon emission tomography/computed tomography (SPECT/CT) with technetium-99m-diphosphonate (99mTc-MDP) was used to assist in the diagnosis and results showed diffuse metastatic microcalcification in the lungs and stomach. The patient underwent right parathyroidectomy and 99mTc-MDP SPECT/CT scan six months later showed a significantly reduced radioactive distribution in the lungs and none in the stomach. Diffuse metastatic microcalcification in the lungs and stomach due to PHTP is rare and can easily be misdiagnosed.
Background
Primary hyperparathyroidism (PHPT), a common endocrine disorder characterized by hypercalcaemia and an elevated parathyroid hormone (PTH) levels, is diagnosed by biochemical methods. 1 The condition is due to excessive PTH secretion from a single parathyroid adenoma (80–90% cases), multiple gland disorder (10–20% cases) or parathyroid cancer (<1% cases).1,2 Abnormal calcium homeostasis due to PHPT can involve several organs including bone and kidneys, as well as neuromuscular, cardiovascular, and gastrointestinal systems. 3
Clinical symptoms of PHPT affecting the respiratory system are rare and often caused by metastatic microcalcification.4–7 Diagnosis is challenging because it may be misdiagnosed as pulmonary oedema and/or interstitial lung disease. We present here a case of PHPT with diffuse metastatic microcalcification in the lungs and stomach detected by single-photon emission tomography/computed tomography (SPECT/CT) using technetium-99m-diphosphonate (99mTc-MDP).
Case Report
A previously healthy 34-year-old Chinese man was admitted to our hospital with a six-month history of nausea and vomiting that had progressively worsened over the past two weeks. He was an ex-smoker of 2–3 packs/day for 10 years and had no history of exposure to occupational fumes. The patient’s physical examination findings were unremarkable and his vital signs were normal. His laboratory test findings on admission are shown in Table 1. The following parameters were elevated: haemoglobin (Hb), 74 g/l (normal range 113–172 g/l); alkaline phosphatase, 360 U/l (normal range, 45–125 U/l); creatinine 182 µmol/l (normal range, 57–97 µmol/l); calcium, 3.1 mmol/l (normal, 2.1–2.5 mmol/l); PTH (1516 pg/ml (normal range, 12–65 pg/ml); erythrocyte sedimentation rate, 83 mm/h (normal range, 0–15 mm/h). All other laboratory findings, including plasma 25- hydroxyvitamin D levels, were within the normal range. In addition, indicators of liver, coagulation and thyroid function as well as tumour markers and antinuclear antibodies were within normal limits.
Laboratory test results.

Numbers in bold are outside the normal range.
Technetium-99m-sestamibi (99mTc-MIBI) scintigraphy showed focal radiotracer accumulation along the right inferior aspect of the thyroid lobe on early-phase imaging (Figure 1A) that persisted on delayed imaging (Figure 1B). SPECT/CT fused images (Figure 1C, D and E) showed focal 99mTc-MIBI uptake localized to a single abnormal right inferior parathyroid gland. Enhanced CT showed vivid enhancement of the lesion in the arterial phase (Figure 1F) and weak clearance in the venous phase (Figure 1G). Ultrasonography showed a homogeneously hypoechoic nodule, 1.5 cm in size, posterior to the right thyroid gland (Figure 1H). Based on these results, a diagnosis of PHPT due to a single parathyroid adenoma was made and parathyroidectomy was recommended. However, on the second day after admission, the patient developed a dry cough with no fever. A chest CT scan showed diffuse ground-glass appearance in both lungs. Bronchoscopy, bronchoalveolar lavage and ultrasonic cardiography indicated no abnormalities. The patient was prescribed antibiotics/antifungals (piperacillin, sodium tazobactam and caspofungin), corticosteroids (methylprednisolone) and montelukast for seven days and cinacalcet, salcatonin, iron supplementation (Niferex) and furosemide for 14 days.
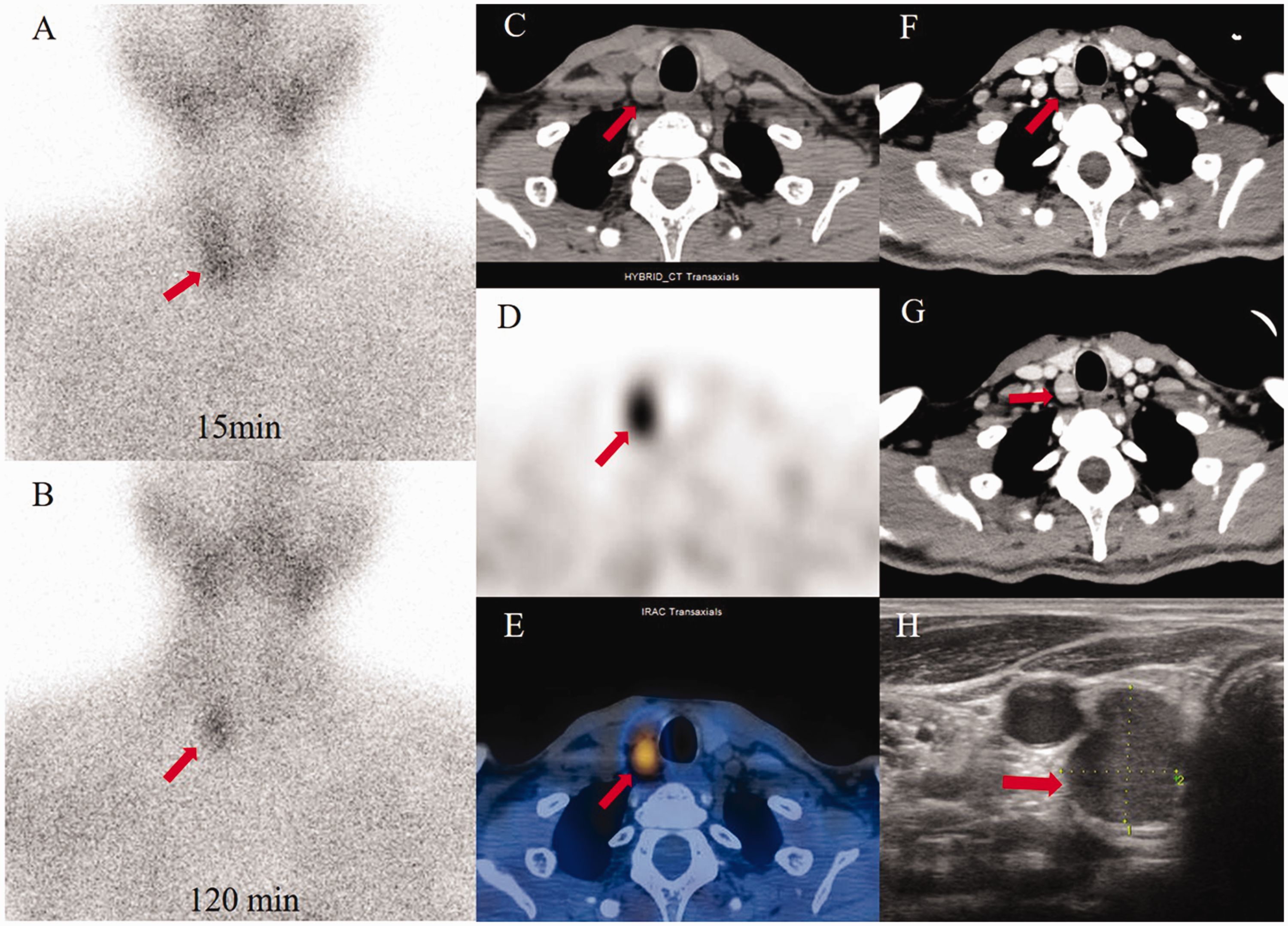
(A) Technetium-99m-sestamibi (99mTc-MIBI) scintigraphy showed focal radiotracer accumulation (arrow) in the right inferior thyroid lobe on early-phase and (B) delayed-phase imaging (120 mins later). (C) Single-photon emission tomography/computed tomography (SPECT/CT) with 99mTc-MIBI demonstrated a soft tissue nodule located in the posterior lobe of the right inferior thyroid gland with radiotracer accumulation (arrow). (D) Axial view. (E) Fused image. (F) Enhanced CT indicated vivid enhancement of the nodule in the arterial phase (arrow). (G) Weak clearance in the venous phase (arrow). (H) Ultrasonography showed a homogeneously hypoechoic parathyroid nodule 1.5 cm in size (arrow).
After 14 days, his dry cough had not improved. A whole-body scan using technetium-99m-diphosphonate (99mTc-MDP) indicated increased accumulation of radioactivity diffusely throughout the lungs and stomach (Figure 2A). SPECT/CT fused images showed that the radioactive uptake was heterogeneously distributed within the pulmonary parenchyma and stomach (Figure 2B and C). Gastroscopy without biopsy yielded normal results. His diagnosis was amended to metastatic pulmonary and gastric microcalcification due to parathyroid adenoma. The patient underwent right parathyroidectomy. Histopathology of the PTH tissues showed nest-like distribution of chief cells, which confirmed a parathyroid adenoma (Figure 3A and B).

(A) A whole-body scan using technetium-99m-diphosphonate (99mTc-MDP) showed extensive diffuse pulmonary and gastric uptake. (B and C) Single-photon emission tomography/computed tomography (SPECT/CT) with 99mTc-MDP showed that the radioactive uptake was heterogeneously distributed within the pulmonary parenchyma and stomach (arrow). without any abnormal bone uptake. Upper is CT; middle is SPECT; bottom is fused image.

Haematoxylin and eosin staining of the parathyroid adenoma. The adenoma consisted of chief cells in a nest-like distribution (A) magnification x40 (B) magnification x100.
One day after surgery, the patient’s PTH level decreased to 9.6 pg/ml, and his calcium levels returned to within normal levels (Table 1). His dry cough gradually improved and the patient regained health. At the follow-up visit, six months after surgery, his calcium and 25-hydroxyvitamin D levels were within normal limits but his PTH levels were mildly elevated (Table 1). A repeat 99mTc-MDP SPECT/CT showed no radioactive distribution in the stomach and significantly reduced radioactive distribution with slight, uniform ground-glass features in the pulmonary parenchyma (Figure 4A, B and C).

(A) A whole-body scan using technetium-99m-diphosphonate (99mTc-MDP) showed no radioactive distribution in the stomach and significantly reduced radioactive distribution in the pulmonary parenchyma. (B and C) Single-photon emission tomography/computed tomography (SPECT/CT) with 99mTc-MDP showed mild radioactive distribution with slight, uniform ground-glass features in the pulmonary parenchyma and no radioactivity in the stomach (arrow). Upper is CT; middle is SPECT; bottom is fused image.
This case report was approved by the Ethics Committee of the First Affiliated Hospital, Zhejiang University School of Medicine. Signed patient consent is required from the patient. We followed the CARE guidelines.
Discussion
PHPT, the most common cause of hypercalcaemia, predominantly affects postmenopausal women, with a female/male ratio of 2.5: 1. 8 The condition may present as a symptomatic or asymptomatic disease and mainly affects the skeletal and urinary systems. 9 To our knowledge, there have been few reports of patients with a parathyroid adenoma who presented with symptoms suggesting metastatic microcalcification in lungs and stomach.4–7
Metastatic microcalcification is defined as calcium deposition in normal tissue and usually occurs in conditions caused by hypercalcaemia. Most reports of metastatic microcalcification have involved patients with end-stage chronic renal disease but occasionally the entity has been reported in patients with osteolytic malignancies, sarcoidosis, hypervitaminosis D and PHPT.10–15 Data from the few reports of metastatic microcalcification due to parathyroid adenoma have shown that the deposition tends to occur in the stomach, kidneys, heart and lungs, with the pulmonary system being particularly susceptible.4–7,16 The pathogenic mechanisms of metastatic microcalcification have yet to be elucidated but most reports suggest that hypercalcaemia and a local alkaline environment may contribute to the condition. 17 In the case presented here, the patient had hypercalcaemia due to PHPT and impaired kidney function, which would have resulted in a decrease in the excretion of excess calcium. Therefore, excess calcium would have been deposited in tissues and organs including the lungs. Some reports have shown that metastatic microcalcification occurs in the apical lobes of the lungs, which have lower CO2 levels than the upper lobes, and so a greater alkaline environment.17,18
From the few reports of metastatic microcalcification in the lungs due to PHPT, it appears that the patients tend to present with cough and dyspnoea. 4–7, However, respiratory distress and fulminant respiratory failure have also been reported.5–7,16,19 Our patient had dry cough, which may have been related to microcalcification in the alveolar septa. The results of his CT scan were non-specific. Because the observed heterogeneous ground-glass opacities that were distributed throughout both lungs could have been due to other primary diseases such as pulmonary oedema or interstitial lung disease, we used SPECT/CT with 99mTc-MDP to assist in the diagnosis. This method is a sensitive technique for detecting metastatic microcalcification because the hydroxyapatite crystals that are the chief constituent of the microcalcification avidly absorb 99mTc-MDP. 17,20Metastatic microcalcification in the stomach was also observed by SPECT/CT in this patient. Regaining a normal calcium concentration in the blood is crucial in the treatment of metastatic microcalcification and after successful parathyroidectomy, metastatic microcalcification and its related symptoms improved in our patient.
In conclusion, diffuse metastatic microcalcification in the lungs and stomach due to PHTP is rare and can easily be misdiagnosed and inadequately treated. With the assistance of SPECT/CT with 99mTc-MDP we were able to make an accurate diagnosis of metastatic microcalcification in the lungs and stomach in a male patient with a parathyroid adenoma.
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Science and Technology Panning Project of Zhejiang Province, China (2018KY363) and Department of education of Zhejiang Province, China (Y201738214).