
Abstract
Objective
Perioperative cardiovascular events constitute the majority of complications in noncardiac surgery. Older and female patients have been less investigated. We aimed to evaluate differences in perioperative cardiovascular outcomes by age and sex.
Methods
We enrolled 1079 patients (57.5 ± 17.0 years, 42.6% women) undergoing intra-abdominal surgery from July 2007 to June 2008 and compared occurrence of perioperative cardiac events by age (≥65 vs. <65 years) and sex. Multivariable logistic regression was used to investigate associations between age, sex, and outcomes.
Results
Age ≥65 years was associated with perioperative myocardial infarction (MI) (odds ratio [OR] 2.9, 95% confidence interval [CI]: 1.3–6.6) and total cardiovascular events (OR 2.4, 95% CI: 1.3–4.2). Age ≥65 years was associated with higher perioperative MI risks in men (OR 4.7, 95% CI: 1.3–17.6) than in women (OR 3.1, 95% CI: 1.2–8.3). Advanced age was associated with heart failure in women (OR 13.9, 95% CI: 1.7–110.5). Female sex was a risk factor for heart failure in elderly patients (OR 4.2, 95% CI: 1.1–15.7).
Conclusions
Advanced age appeared to be associated with increased perioperative cardiac risk but differed by sex. Tailored strategies should be considered with respect to the patient’s sex.
Introduction
It is estimated that more than 300 million noncardiac surgeries are performed each year, and the numbers are increasing.1,2 Despite great advances in medical techniques, significant perioperative morbidity and mortality occur, and nearly half of these deaths are attributed to cardiovascular causes. 3
Age is thought to be an essential risk factor for adverse cardiac outcomes. 4 With life expectancy increasing, various heart diseases associated with aging have become more common among patients undergoing surgery. However, elderly people have often not been well represented in large-scale studies; when they have been included, most studies have involved cardiovascular surgery and less is known about noncardiac surgeries. Women have different traditional risk factors for cardiac disease than men 5 and tend to have atypical symptoms, which can lead to a delay in seeking medical help and receiving appropriate treatment. Catecholamine stress, however, might lead to exaggerated responses in women, 6 and thus could result in more perioperative cardiac events. It is unclear whether elderly patients and women, as less investigated populations, might show different incidence and types of perioperative cardiovascular outcomes than their younger and male counterparts undergoing noncardiac surgery.
In the present study, we aimed to observe individuals undergoing intra-abdominal surgery in a 1-year period in our center, focusing on possible differences in age- and sex-related perioperative cardiac complications.
Material and methods
Ethical approval
This retrospective cohort study was conducted in a comprehensive surgical department of a tertiary center and was approved by the Ethics Committee on Clinical Investigation of Peking University First Hospital. Considering the retrospective nature of the present study, a waiver of informed consent from patients was obtained.
Patients and study design
From 1 July 2007 to 30 June 2008, consecutive eligible adult patients (age ≥18 years) hospitalized for open abdominal surgery in our center were enrolled to establish the study cohort. Medical records were retrieved to capture data on patients’ characteristics, including demographics, past medical history, and perioperative variables. The perioperative period was defined as the interval between admission and discharge. The medical history variables were defined by the presence of eligible diagnosis codes (International Classification of Diseases, Tenth Revision [ICD-10]: I10 for hypertension, I20 for coronary heart disease, I50 for heart failure) or prescription fills.
Exposure variable—abdominal surgery
In this study, the exposure variable was abdominal surgery, which was defined as open abdominal surgery that involved the stomach, duodenum and jejunum, liver, bile bladder, spleen, pancreas, colon, appendix, intestine, sigmoid colon, or rectum. Surgery conducted through laparoscopy was excluded.
Follow-up and outcomes
Patients were followed during their hospital stays. Medical records were retrieved to capture data on symptoms, physical examination, laboratory investigations, electrocardiography (ECG), and imaging. The perioperative cardiovascular outcome endpoints were re-evaluated according to the following definitions:
Perioperative myocardial infarction (MI): Detection of an increase and/or decrease in cardiac biomarker value with at least one value above the 99th percentile upper reference limit (URL) and with at least one of the following criteria: symptoms of ischemia, new ST-T changes or left bundle branch block (LBBB), development of pathological Q waves in the ECG, imaging evidence of new loss of viable myocardium, or identification of an intracoronary thrombus by angiography, according to the Third Universal Definition of Myocardial Infarction.
7
We used cardiac troponin I (cTnI) to define perioperative MI, and total cardiac events (as follows) were counted using this endpoint. Acute heart failure: At least one of the following criteria was met: exertional, resting, or paroxysmal nocturnal dyspnea; S3 heart sound; new-onset bilateral rales, fluid overload, or peripheral edema that required diuretics; signs of heart failure on chest X-ray or echocardiography.
8
Arrhythmia: New-onset arrhythmia recorded by ECG during the index hospitalization, including ventricular fibrillation/tachycardia, atrial fibrillation, atrial flutter, supraventricular tachycardia except for sinus tachycardia, second- or third-degree atrioventricular block, and long R-R interval (>2 s). Death of cardiac origin. All-cause death. Total cardiovascular events: occurrence of at least one of the events mentioned above.
Statistical analyses
Continuous data are described as mean ± standard deviation or median and interquartile range, and categorical data are expressed as percentages. Baseline and perioperative characteristics were compared between two groups using the t-test or Mann–Whitney U test for continuous variables, and with Fisher exact tests or chi-square tests for categorical variables. Age- and sex-related factors were analyzed according to age ≥65 or <65 years and male or female, respectively.
Univariable analysis was used to screen possible confounders from the medical history (hypertension, diabetes, coronary heart disease, cerebrovascular disease, chronic obstructive pulmonary disease, chronic kidney disease, and anemia), indication for surgery (cancer vs. other disease), type and timing of the surgery (complicated surgery involving more than three major organs vs. others; elective vs. emergent surgery), type of anesthesia (general anesthesia vs. other modes of anesthesia), and blood loss (>100 mL vs. ≤100 mL) for each endpoint. Multivariable logistic regression was conducted to investigate whether the cardiac outcomes were associated with age and sex after adjusting for the confounders. Odds ratios (OR) are reported with 95% confidence intervals (CI). For each age and sex subgroup, logistic regression was conducted to further assess the association between age, sex, and cardiac outcomes.
A p-value <0.05 (two-tailed) was considered statistically significant. All analyses were performed using SPSS statistical software (version 22.0; IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics of the study population
We retrospectively evaluated 1258 patients who underwent intra-abdominal surgery between 1 July 2007 and 30 June 2008. Of these, we excluded patients with missing baseline information or with repeat surgery in the same time period for any reason (179/1258, 14.2%). A total of 1079 patients (average age 57.5 ± 17.0 years) were included in the analysis, of whom 460 (42.6%) were women. Overall, this was a cohort with considerable comorbidities, including hypertension (29.0%), diabetes (14.3%), hyperlipidemia (37.5%), anemia (23.5%), coronary heart disease (9.7%), and cerebrovascular disease (5.3%). Most (74.2%) of the surgeries were elective. Complicated surgeries (involving more than three major organs) constituted 9.1% of the total procedures. About one-third (33.2%) of patients received general anesthesia (Table 1).
Characteristics of patients in the whole population and stratified by age and sex.

*p < 0.05.
SD, standard deviation; COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease; IQR, interquartile range.
Elderly (≥65 years) patients had more comorbidities, including hypertension, diabetes, coronary artery disease, cerebrovascular disease, and chronic kidney disease, than younger patients. They also had more cancer, received more general anesthesia, and had a longer time for anesthesia and surgery and greater blood loss. Fewer of them underwent emergent surgery (Table 1).
Men and women were of similar ages in the whole study population. Women were significantly less likely to be smokers or to have chronic obstructive pulmonary disease (COPD) compared with men, but had more history of hypertension. Women underwent fewer emergent surgeries and had less blood loss than men (Table 1).
Perioperative cardiovascular events
Eighty-three patients (7.7%) experienced cardiovascular events during the perioperative period. Events of interest included 40 cases of perioperative MI, 18 cases of acute heart failure, 24 cases of arrhythmia (20 cases were atrial fibrillation), 1 death of cardiac origin, and 30 cases of all-cause deaths. Some patients experienced more than one type of perioperative cardiovascular event.
Age-associated perioperative cardiovascular events
Older patients (≥65 years) had significantly more adverse perioperative cardiac events, including MI, acute heart failure, atrial fibrillation, deaths, and total cardiovascular events compared with younger patients (Figure 1). When we evaluated the association of age with perioperative risk, however, patient outcomes differed by sex. Older men had significantly more perioperative MI (7.2% vs. 1.6%, p = 0.001), deaths (4.8% vs. 1.6%, p = 0.027), and total cardiovascular events than younger men (10.8% vs. 4.1%, p = 0.002). Older women had more perioperative MI than younger women (6.5% vs. 1.5%, p = 0.007). They also had more atrial fibrillation (5.9% vs. 0.4%, p < 0.001), acute heart failure (4.8% vs. 0.4%, p = 0.002), and total cardiovascular events (17.2% vs. 3.3%, p < 0.001) than younger women but not more deaths (3.2% vs. 2.2%, p = 0.558) (Figure 1).

Occurrence of perioperative cardiovascular events in older (≥65 years) and younger (<65 years) patients in the whole population (a) and in male (b) and female (c) subgroups.
In the logistic regression analysis, advanced age (≥65 years) was associated with occurrence of multiple perioperative cardiovascular events in the total population. After adjusting for baseline and perioperative variables, age ≥65 years was still associated with perioperative MI (OR 2.9, 95% CI: 1.3–6.6, p = 0.013) and total cardiovascular events (OR 2.4, 95% CI: 1.3–4.2, p = 0.003). However, advanced age showed different associations with perioperative events for male and female subgroups. Specifically, age ≥65 years was associated with MI (OR 4.7, 95% CI: 1.3–17.6, p = 0.020) and total cardiovascular events (OR 2.2, 95% CI: 1.1–4.4, p = 0.026) in men; and was associated with MI (OR 3.1, 95% CI: 1.2–8.3, p = 0.024), heart failure (OR 13.9, 95% CI: 1.7–110.5, p = 0.013), and total cardiovascular events (OR 3.5, 95% CI: 1.4–8.9, p = 0.008) in women (Figure 2).

Forest plot showing the association between advanced age (≥65 years) and the adjusted odds ratio (OR) of perioperative cardiovascular outcomes. Horizontal lines represent 95% confidence intervals (CI). *p < 0.05.
Sex-associated perioperative cardiovascular events
In general, no significant differences were observed between men and women for all types of cardiovascular events. The same was true in the younger population (<65 years). In the older patients, however, more cases of acute heart failure occurred in women than in men (4.8% vs. 1.2%, p = 0.034) (Figure 3). After adjusting for baseline and perioperative variables, female sex was still associated with heart failure in older patients (OR 4.2, 95% CI: 1.1–15.7, p = 0.034) (Figure 4).

Perioperative cardiovascular events occurred in male and female patients in the whole population (a) and in the younger (<65 years) (b) and older (≥65 years) (c) subgroups.
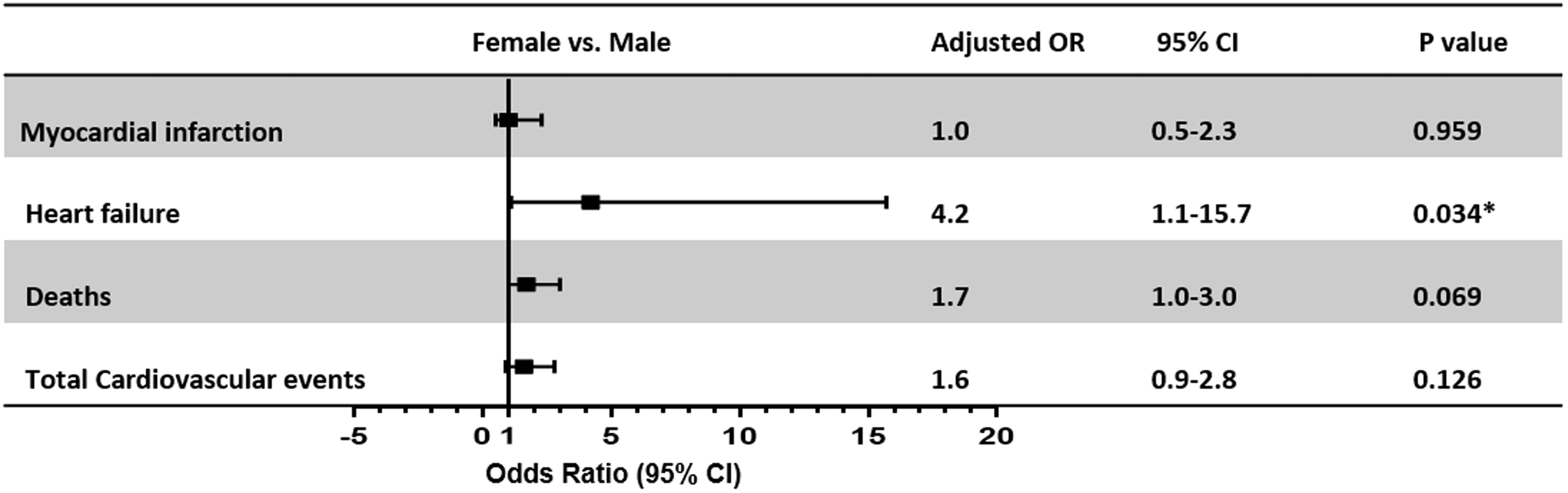
Forest plot showing the association between female sex and adjusted odds ratio (OR) of perioperative cardiovascular outcomes in older patients (≥65 years). Horizontal lines represent 95% confidence intervals (CI). *p < 0.05.
Discussion
In the present study, we evaluated age- and sex-related cardiovascular risks in patients undergoing open abdominal surgery. Elderly patients had increased perioperative cardiac events compared with younger patients. More importantly, diverse perioperative cardiac complications were observed in elderly patients of different sexes.
With improvements in medicine, the life expectancy of the general population has increased. It is estimated that elderly individuals require surgery almost four times more often than younger people. 9 Age has long been considered in perioperative risk stratification systems.10,11 Patients with advanced age and prevalent atherosclerotic risk factors are more vulnerable to adverse cardiac outcomes. In addition, reduced elasticity of heart and vascular beds occurs with aging, making diastolic dysfunction a natural effect of aging. Insults of perioperative stresses, such as anesthesia induction, mechanical ventilation, corticosteroid and catecholamine release, blood loss, and tissue inflammation, might make atherosclerotic plaques unstable and cause acute cardiac decompensation. 12 Elderly patients with reduced cardiac reserve may be challenged by these stressors. Therefore, it is not surprising that elderly patients have significantly increased perioperative cardiovascular events compared with younger patients.
A key finding in the present study lies in the observation that advanced age was associated with different cardiovascular outcomes for men and women. The events we focused on were perioperative MI and heart failure. Perioperative MI has been shown to be the most common major perioperative cardiovascular complication, ranging from 1.4% to 5.8% in noncardiac surgery,13–15 and it is associated with a poor prognosis. The detection of an increase and/or decrease in cardiac biomarkers, with at least one of the values being elevated above the 99th percentile URL, is central to the universal definition of MI. 7 Historically, well-accepted studies of perioperative MI were based on the diagnosis of the WHO definition, which requires increased creatinine kinase isoenzyme (CK-MB) levels. 16 Because troponin assays, which have a much higher sensitivity than CK-MB, have been used as a biomarker in the definition of MI, 16 the occurrence of perioperative MI has increased correspondingly. This discrepancy in the diagnostic standard also contributed to our higher incidence of composite cardiac events compared with prior studies.13–15 When using the CK-MB cut-off, we observed an MI rate in line with earlier research.
In our cohort, elderly men had significantly more perioperative MI and deaths than younger men. Age ≥65 years was associated with an approximately five-fold increased risk of perioperative MI. In contrast, elderly women had increased perioperative MI risks but to a lesser extent (approximately three-fold increased risk) compared with younger women. These data highlighted the more severe ischemic myocardial injury in elderly men. Perioperative MI is thought to involve various mechanisms. Primary coronary ischemia (type 1), as a consequence of rupture of unstable plaque and formation of a thrombus, is a classical acute coronary syndrome. Type 2 MI, defined as an imbalance of myocardial oxygen supply and demand, might result from various perioperative insults, including hypoxia, blood loss, inflammation, fluctuations of blood pressure, and arrhythmias. 7 Elderly patients of both sexes had more history of hypertension, diabetes, coronary heart disease, and cerebrovascular disease than younger patients, indicating a higher accumulative atherosclerotic burden and greater inclination to develop type 1 MI. Our results were further confirmed by a recent prospective diagnostic study that enrolled 2018 consecutive patients undergoing noncardiac surgery in which the high-risk criteria were >65 years of age or preexisting atherosclerotic disease. 17 However, women tend to develop atherosclerosis later in life than men because of the protection from estrogen before menopause, 18 which might alleviate part of the accumulative risks of aging. Women are also more likely to have non-obstructive coronary artery disease, with microvascular and endothelial dysfunction leading to myocardial ischemia. 19 Coronary microvascular disease, in turn, might also serve as a preconditioning mechanism. Additionally, elderly patients in our study endured prolonged anesthesia and surgery and more blood loss during surgery, contributing to greater occurrence of type 2 MI. With more men being smokers and having a history of COPD, they might have suffered more from reduced pulmonary function and oxygen supply during surgery.
Elderly women had a significantly increased incidence of perioperative heart failure compared with younger women, which resulted in increased total perioperative cardiovascular events. Female sex per se was identified as a risk factor for perioperative heart failure in older patients after adjustment for other confounders. Overall, older women were found to be the most vulnerable to perioperative heart failure.
Heart failure can account for 2.5% to 10% of the perioperative complications for noncardiac surgery20,21 and is another major adverse cardiac outcome. Advanced age is thought to affect cardiac dysfunction, and the impact is more pronounced for women. 22 The age-associated increase in systolic blood pressure is steeper in women than in men, resulting in a higher prevalence of hypertension in women, 23 which was well demonstrated in the distribution of our cohort. Hypertension has been shown to place women at higher risk of heart failure, 24 partially because women have greater ventricular stiffness than men at any given age, as well as steady increases with aging. 25 Women also have a blunted vasodilator reserve, evidenced by an abrupt rise in pulmonary artery pressure in response to saline infusion. 26 This elevation of pulmonary artery pressure is associated with acute cardiac decompensation. 27 In a perioperative scenario, therefore, significant fluid shifts could induce volume overload of the circulation and promote the development of heart failure. Additionally, women are more sensitive to sympathetic stress and catecholamine surge, both of which are critical triggers of arrhythmia. 28 Atrial fibrillation was the most common arrhythmia in our perioperative cohort, especially in women, which might contribute to more heart failure events. The loss of effective atrial contraction and the associated increase in ventricular rate result in an increase in left atrial pressure, which manifests clinically as dyspnea and exercise intolerance.
Myocardial ischemia represents one of the most important origins of acute heart failure. Women with MI are more likely to develop heart failure, and even a minimal elevation of the perioperative troponin level is associated with a worse prognosis. 3 The term “myocardial injury after noncardiac surgery (MINS)” has been advocated, 29 emphasizing that patients may have up to a 10-fold higher risk of congestive heart failure although more than half of MINS patients would not fulfill the conventional diagnosis of MI. 29 Additionally, MINS without ischemia has been shown to be associated with 30-day mortality in the large prospective cohort study VISION. 30 Recently, it has been demonstrated that coronary microvascular disease and ischemia are among the key mechanisms of diastolic heart failure. 31 In our study population, elderly women had more perioperative MI than younger women, and perioperative MI might facilitate the development of cardiac dysfunction.
Except for the comorbidities increasing the risk of heart failure, basic research 32 supports the idea that estrogen deficiency is a main contributor in the development of heart failure in the post-menopausal state. Activation of the renin-angiotensin-aldosterone system (RAAS) occurs in response to low estrogen levels after menopause, coincident with a decline in NO usage and increased collagen synthesis. In accordance with this, a more favorable treatment effect of sacubitril-valsartan (valsartan is a RAAS inhibitor) was observed in women than in men in a sub-analysis of the PARAGON-HF study. 33
This study had some limitations. It was a single-center, retrospective cohort study, and the medical history and cardiac endpoint events were captured from the electronic medical record. Thus, there is potential for reporting and ascertainment bias. The cohort was established a decade ago, and diagnosis for some cardiac outcomes, such as definitions of MI, have been updated since then. Details of in-hospital medical management for cardiovascular disease were not available for review; therefore, we cannot exclude the possibility that these medications may account for some variation in the occurrence of cardiac morbidity and mortality. Low incidence of some complications limited the quality of the analysis. Although we stressed older age as an important perioperative risk factor and showed different associations for men and women, our use of an age cut-off instead of treating age as a continuous variable might have weakened the analysis. Studies with a prospective design and a large population might improve this analysis.
In summary, we observed not only an elevated perioperative cardiovascular risk for elderly patients in general but also different correlations of advanced age with adverse cardiac events for women and men in this large, single-center cohort of patients who underwent intra-abdominal surgery. We cannot overstate the importance of evaluation and risk stratification of patients before surgery. Elderly patients need more careful preparation for elective surgery, and tailored strategies should be considered according to the sex of the patient.