
Abstract
Objective
This study aimed to compare the clinical features of pulmonary cryptococcosis (PC) in patients with and without central nervous system (CNS) involvement.
Methods
We retrospectively reviewed demographics, presenting symptoms, radiographic features, and laboratory findings of patients diagnosed with PC in 28 hospitals from 2010 to 2019. Risk factors for CNS involvement were analyzed using logistic regression models.
Result
A total of 440 patients were included, and 36 (8.2%) had CNS involvement. Significant differences in fever, headache, and chills occurred between the two groups (overall and with/without CNS involvement) for fever (17.8% [78/440]; 52.8% vs. 14.6% of patients, respectively), headache (4.5% [20/440]; 55.6% vs. 0% of patients, respectively), and chills (4.3% [19/440]; 13.9% vs. 3.5% of patients, respectively). The common imaging manifestation was nodules (66.4%). Multivariate analysis showed that cavitation (adjusted odds ratio [AOR] = 3.552), fever (AOR = 4.182), and headache were risk factors for CNS involvement. Routine blood tests showed no differences between the groups, whereas in cerebrospinal fluid the white blood cell count increased significantly and glucose decreased significantly.
Conclusion
In patients with PC, the risk of CNS involvement increases in patients with headache, fever, and cavitation; these unique clinical features may be helpful in the diagnosis.
Introduction
Cryptococcus is a fatal pathogenic fungus that can easily infect patients through the respiratory tract. The common clinical manifestation is pulmonary infection, 1 which may cause pulmonary cryptococcosis (PC). PC is a common disease, and cryptococcosis has become the second most common mycosis in China. 2 Cryptococcus is an opportunistic pathogenic fungus that is prone to infect immunocompromised patients, such as patients with acquired immunodeficiency disease (AIDS). 3 Studies show that Cryptococcus can also infect immunocompetent patients. 4 Previously, the diagnosis of PC was limited to clinical symptoms and imaging findings. However, its symptoms and imaging findings are similar to those of lung cancer, tuberculosis, bacterial pneumonia, and other pulmonary fungal diseases 1 and, therefore, the misdiagnosis rate is very high.
Cryptococcus may infect the central nervous system (CNS). The incidence of CNS infections in patients with cryptococcosis was reported, in one study, to be 83.4% (7315/8769) in China. 5 PC is prone to infect the CNS, leading to meningitis. 6 Cryptococcal meningitis has high morbidity and mortality, 7 and delayed diagnosis of cryptococcal meningitis is an independent risk factor for death. 8 In this study, we retrospectively analyzed clinical and pathological data of patients with PC, and we identified independent risk factors to predict CNS involvement. Early detection, diagnosis, and treatment may benefit patients.
Materials and Methods
Patients
We retrospectively analyzed records of patients diagnosed with PC in 28 hospitals from 2010 to 2019. In total, 440 patients were identified from hospital records. Our diagnostic criteria were as follows: Cryptococcus was found or cultured in blood, pleural effusion (consistent with the clinical infection site), or pathological lung tissue collected from a normally sterile site; Cryptococcus species indicating encapsulated budding yeasts were found in specimens collected under sterile conditions from diseased tissues through histopathological examination, accompanied by corresponding tissue inflammatory reaction; CNS infection was diagnosed by a positive fungal culture for Cryptococcus from cerebrospinal fluid (CSF) or by positive CSF India ink staining; and cryptococcal antigen titration from CSF was positive. 9 Exclusion criteria were as follows: (1) incomplete medical records, or (2) cases with co-infection of other pathogens in the lungs that were identified with clear evidence. A total of 440 patients were included; all patients had undergone computed tomography (CT) imaging and laboratory examinations, and 83 patients who had a lumbar puncture also underwent laboratory tests of CSF. Detailed records of demographics, host immune status, symptoms, and laboratory tests of patients were available. The ethics boards in these hospitals determined that informed consent from these patients was not required because this study involved a retrospective review of records only.
Imaging analysis
All imaging data were analyzed by two imaging physicians (with more than 8 years of experience in radiological diagnosis). The CT images were evaluated, and various signs (nodules, slices, lumps, cavities, and halo signs) and conditions of pleural effusions were recorded in detail.
Data analysis
All data were analyzed using SPSS software (version 19.0; IBM Corp., Armonk, NY, USA). The clinical features of patients were summarized using descriptive statistical methods, and continuous data were expressed as mean ± standard deviation. The Mann–Whitney U test was used to analyze continuous variables, and the Chi-square test and Fisher’s test were used for categorical variables. Risk factors for infecting the CNS were analyzed using logistic regression models. Risk assessment was conducted by binary classification. P < 0.05 was considered to indicate a significant difference.
Results
Clinical data of patients
The study covered 440 patients with PC (295 men and 145 women) aged between 11 and 78 years, with an average age of 47.5 ± 13.4 years. Among these, 36 (8.2%) had infections involving the CNS. Results showed that the age of patients with CNS involvement was not significantly different from that of patients without CNS involvement, as shown in Table 1.
Clinical features of patients with pulmonary cryptococcosis with or without central nervous system (CNS) involvement.

*Statistically significant.
aIncluding immunocompromised patients.
bImmunocompromised states including malignant tumors, severe trauma or major surgery, organ transplantation, immune connective tissue disease, or treatment with glucocorticoids or immunosuppressive agents.
Underlying diseases
Of the 440 patients, 292 (66.4%) had no underlying diseases and were immunocompetent; 148 (33.6%) had underlying diseases; and no patients had AIDS. The underlying diseases included diabetes, cardiovascular and cerebrovascular disease, liver disease, and lung disease. Seventy (70/440, 15.9%) patients were in an immunocompromised state, and some had underlying diseases. Malignant tumors (12), severe trauma or major surgery (7), organ transplantation (8), immune connective tissue disease (19), or treatment with glucocorticoids or immunosuppressive agents (30) were considered immunocompromised states, and these differed (P < 0.05) between patients with CNS involvement (10/36, 27.8%) and those without (60/404, 14.9%), as shown in Table 1.
Clinical symptoms
The most common clinical symptom was cough (51.6%, 227/440), which occurred in 16 (44.4%) patients with CNS involvement and 211 (52.2%) patients without. Clinical symptoms also included expectoration, fever, headache, and chills. Expectoration was reported in 38.2% (168/440; 41.7% vs. 37.9% in patients with and without CNS involvement, respectively); fever was reported in 17.8% (78/440; 52.8% vs 14.6% of patients, respectively); headache was reported in 4.5% (20/440; 55.6% vs. 0% of patients, respectively); and chills were reported in 4.3% (19/440; 13.9% vs. 3.5% of patients, respectively). Some patients had no obvious symptoms (36.8%, 162/440; 13.9% vs. 38.9% of patients with and without CNS involvement) and no differences were found in other symptoms between the two groups, as shown in Table 1. Multivariate analysis showed that headache and fever (adjusted odds ratio [AOR] = 4.182; P < 0.01) were risk factors for CNS involvement, as shown in Table 2. Because all patients with headache had CNS involvement, the AOR was not calculated.
Risk factors for central nervous system involvement in patients with pulmonary cryptococcosis.
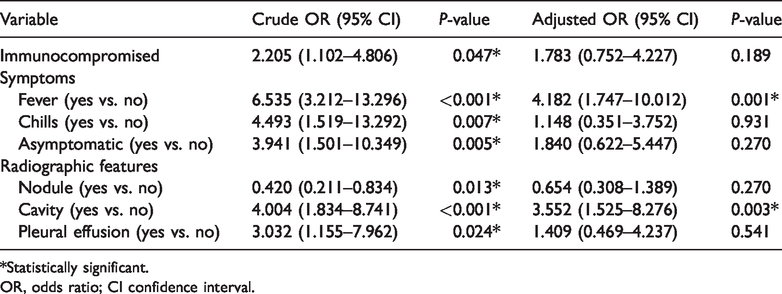
*Statistically significant.
OR, odds ratio; CI confidence interval.
Radiographic features
The most common imaging manifestation was nodules, occurring in 292 cases, followed by patchy consolidation (90/440). Among patients with CNS involvement, 13/36 (36.1%) had cavitation and 6/36 (16.7%) had pleural effusion. In patients with and without CNS involvement, the presence of nodules (47.2% vs. 68.1%; P < 0.001), cavitation (36.1% vs. 9.6%; P < 0.001), and pleural effusion (16.7% vs. 6.2%; P = 0.019) differed significantly. We found no significant differences in other imaging manifestations, as shown in Table 1. Multivariate analysis showed that cavity (AOR = 3.552; P = 0.003) was a risk factor for CNS involvement, as shown in Table 2.
Laboratory results
Analysis of routine blood work showed no significant differences between the two groups. Examination of CSF showed statistical differences in CSF white blood cell count (P < 0.001) and CSF glucose level (P = 0.015) between patients with CNS involvement and those without, as shown in Table 3.
Laboratory results (mean ± SD) of patients with pulmonary cryptococcosis with or without central nervous system (CNS) involvement.

*Statistically significant.
RBC, red blood cell; HGB, hemoglobin; WBC, white blood cell; NEUT, neutrophil; LYM, lymphocyte; MONO, monocyte; HCT, hematocrit; PLT, platelets; CRP, C-reactive protein; ALB, albumin; CSF, cerebrospinal fluid.
Discussion
In the past 20 years, the incidence of PC has been increasing in China, 10 but the incidence of the disease is still underestimated. 11 PC often occurs in immunocompromised populations, especially in individuals with AIDS. Although our study included no AIDS patients, 15.9% of immunocompromised individuals suffer from the disease. We found that immunocompromised patients in our cohort were more likely than immunocompetent patients to have involvement of CNS and develop meningitis, which was similar to the findings of other studies.3,12 When immunocompromised hosts are infected with Cryptococcus, the CNS is easily infected once symptoms occur in the lungs. 13
The most common symptoms of PC found in our study sample were cough (51.6%) and expectoration (38.2%), which is similar to previous reports.13–15 Common clinical symptoms of CNS involvement are headache, fever, and chills, and the risk of CNS involvement is significantly increased when symptoms of fever and headache are present. 16 According to reports, immunocompetent patients infected with Cryptococcus pneumonia have mild or no symptoms.3,17 In this study, there were 162 asymptomatic patients, and our findings support these results.
The most common imaging manifestation in patients with PC is nodules (66.4%), which is similar to other reports. 14 Pleural effusion is a rare imaging manifestation associated with cryptococcosis. Patients with meningitis and compromised immunity are prone to develop pleural effusion, 18 and cryptococcal antigens may stimulate the pleura to produce pleural effusion. 19 Statistical analysis in our study showed that patients with cavitation were more prone to have CNS involvement. It has been reported that cavitation is more common in immunocompromised patients.20,21 Friedman et al. believed that cavitation is a long-term abnormality of lung tissues, 22 which may be more severely infected by Cryptococcus and more likely to be associated with CNS infection. These imaging manifestations play a guiding role for further diagnosis and exclusion of CNS involvement in patients with PC.
We found no significant differences in routine blood results between the two groups. The CSF WBC count was significantly increased in patients with CNS infection, reflecting an immune response of the body to Cryptococcus infection. In addition, patients with CNS infection had significantly reduced CSF glucose, which generally reflects a lowered immune response in patients. 7 Infection with Cryptococcus was negatively correlated with CSF glucose level, which reflected the severity of infections of CNS. 11
Our study has a number of limitations: first, the number of PC patients with CNS involvement was small, which may affect the analysis. Second, the imaging classification was mainly based on morphology, and data on details such as nodule size, number, and boundaries were not collected. Third, samples came from 28 hospitals, so differences existed in doctors and laboratory conditions and data. Finally, we did not conduct follow-up on the patients.
Conclusions
PC is easily misdiagnosed as other diseases, including lung cancer, and its diagnosis is based mainly on invasive tests. Immunocompromised patients are more susceptible to infections of the CNS. In patients with PC, the risk of CNS involvement increases in patients with headache, fever, and cavitation. Moreover, CSF WBC count increased, and CSF glucose level decreased significantly. In short, these unique clinical features may be helpful in the diagnosis or exclusion of CNS involvement in patients with PC; early diagnosis is essential for prognosis and treatment.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060521991001 - Supplemental material for Comparison of clinical features of pulmonary cryptococcosis with and without central nervous system involvement in China
Supplemental material, sj-pdf-1-imr-10.1177_0300060521991001 for Comparison of clinical features of pulmonary cryptococcosis with and without central nervous system involvement in China by Xinying Xue, Xuelei Zang, Lifeng Wang, Dongliang Lin, Tianjiao Jiang, Jie Gao, Chongchong Wu, Xidong Ma, Hui Deng, Dingxia Shen and Lei Pan in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Outstanding top talent (2019YXBJ1), Capital's Funds for Health Improvement and Research (2020-2Z-2086), Excellent talents in Beijing “Youth top team” (2019YXBJ2) and “YangFang” plan of Beijing Municipal Hospital Administration (XMLX202115).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Fund Youth Project (81700007) and Beijing National Natural Science Foundation (2019A10).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.