
Abstract
Objective
To describe the proportions of different osseous diagnoses in older patients with temporomandibular disorders (TMD) and to analyze the symptoms, disc position, occluding pairs, and facial skeletal characteristics of patients with bilateral osteoarthrosis (BOA) and bilateral normal joints (BNJ).
Methods
This retrospective cross-sectional study constituted 88 older patients (age ≥60 years). The osseous diagnosis, symptoms, disc position, occluding pairs, and facial skeletal characteristics were evaluated. Variables in BOA patients and BNJ patients were compared using the t-test and chi-square test.
Results
Forty-eight patients had BOA, 7 had unilateral osteoarthrosis, 11 had intermediate osteoarthrosis, and 22 had BNJ. The prevalence of disc displacement without reduction (DDw/oR) in BOA patients was significantly higher than in BNJ patients. BOA patients exhibited greater ANB angle, PP-MP, U1-NPo, L1-NPo, and facial convexity angle; shorter posterior cranial base; and decreased ramus height.
Conclusion
BOA patients with associated DDw/oR had more complaints of orofacial pain and exhibited a shorter posterior cranial base, and greater mandibular retrusion, anterior tooth protrusion, and protruded profile than BNJ patients.
Keywords
Introduction
Temporomandibular disorders (TMD) represent a group of clinical conditions involving masticatory muscles and the temporomandibular joint (TMJ), and their associated structures. The major symptoms are joint noise, articular and/or muscle pain, and mandibular dysfunction. 1 Numerous studies have examined the prevalence of TMDs, and indicated that the affected percentage of the population ranges between 40% and 60%. 2 A few studies have examined the prevalence in the older population, with a reported prevalence of at least one symptom in this population of between 40% and 80%.3,4
Most studies of older patients with TMD have focused on the signs and symptoms, and a diagnosis was often made by questionnaires and/or clinical examinations, which might have impaired the reliability of the diagnosis.5,6 Radiographic studies of TMJ disorders in older patients are limited. According to panoramic radiographs, 38% (315/830) of Swedish older women were diagnosed with temporomandibular joint osteoarthrosis (TMJOA). 7 A total of 41.9% (126/301) of older Japanese people were diagnosed with TMJOA using magnetic resonance imaging (MRI), 8 and 70% (21/30) of older Germans were diagnosed with TMJOA using gadolinium-enhanced MRI. 9 To the best of our knowledge, information on TMD in older people is not well understood because of the limited number and poor designs of previous studies.
A smaller and clockwise-rotated mandible is somehow related to TMD. 10 Similarly, dolichofacial features are significantly associated with TMD signs among the older Vietnamese population, who show an increased ANB angle, upper gonial angle, and Frankfort horizontal-mandibular plane (FH-MP) angle in cephalometry. 11 However, studies of TMD and facial skeletal characteristics have focused mainly on teenagers and young adults, and fewer studies have assessed this relationship in older patients.
Both the number and proportion of older people are increasing, which has become a topic of great concern. The signs and symptoms of TMD could compromise a patient’s physical function and mental well-being and significantly affect the health-related quality of life in older people. Therefore, this study focused on this special group (older patients with TMD) and aimed to compensate for existing studies and draw special attention to this group. The objective was to investigate the proportions of different osseous diagnoses, and to analyze the differences in disc positions and facial skeletal characteristics of patients with bilateral osteoarthrosis (BOA) vs patients with bilateral normal joints (BNJ).
Materials and methods
Subjects
This retrospective study of case notes and radiographs was approved by the Institutional Review Board of the West China Hospital of Stomatology (Approval no., WCHSIRB-D-2018-033). All patients seeking treatment were informed of the possibility that their records might be used for teaching and research purposes, and oral informed consent was obtained. All of the patients’ personal information was de-identified. The study was performed in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) research guidelines. 12
For the analysis, we acquired the patients’ data and radiographs consecutively from January 2017 to October 2019 from our radiology database. The medical records and radiological data were electronically available and easy to access during this period in our hospital, and the radiographic data were mostly complete. The occluding pairs of each patient were calculated from the dental cast recorded at their first visit. The inclusion criteria were as follows: (1) patients registered in our TMJ department with no history of TMJ therapeutic or surgical intervention; (2) patients diagnosed with TMD according to the Diagnostic Criteria for Temporomandibular Disorders, Axis I; 13 (3) patients aged 60 years or older; and (4) patients for whom pretreatment records with high-quality cephalograms were available. Exclusion criteria were (1) patients with craniofacial syndromes, clefts, trauma, or deformity secondary to systemic disease, such as rheumatoid arthritis; (2) patients with previous orthodontic or orthognathic treatment; and (3) incomplete radiographic data. A flowchart of the patients’ enrollment is shown in Figure 1.

Flowchart of the patients who met the study inclusion criteria.
Data collection
The patients’ examinations and diagnoses of TMD were performed by at least two experienced specialists. Cone-beam computed tomography and MRI were used for the diagnosis of osteoarthrosis and disc displacement if the patient had a least one subjective or objective symptom. Data concerning age, gender and comorbidities (hypertension, diabetes, ulcer disease, liver disease, thyroid disease, and any tumor) were obtained from the patient’s medical records. A patient might have more than one comorbidity.
Symptoms
The following patients’ subjective symptoms were collected from their medical records: orofacial pain, TMJ sounds, and abnormal mandibular movement. Orofacial pain was considered present if the patient self-reported orofacial pain, and TMJ sounds were considered present if a click or crepitus was reported. Abnormal mandibular movement was considered present if the patient reported limited mouth opening (less than 36 mm), or closed, lateral, or protrusive movement parafunction. The duration between the initial occurrence of symptoms and the diagnosis was recorded. For patients who exhibited more than one symptom, the duration was determined according to the symptom with the longest duration. The objective symptoms were collected from the patients’ medical records, which were examined by the same experienced specialists.
Osseous diagnosis
The osseous diagnoses of bilateral TMJs were evaluated using cone-beam computed tomography (J Morita Mfg. Corp., Kyoto, Japan). The osseous diagnosis on each side was classified as normal, intermediate for osteoarthrosis, and osteoarthrosis according to the criteria proposed by Ahmad. 14
Disc position
Bilateral TMJ disc positions were evaluated using MRI performed in the sagittal (maximum intercuspal and maximum-opening positions) and coronal (closed) planes using a 1.5-T MRI scanner (Philips Healthcare, Best, the Netherlands) with TMJ surface coils. The disc position was characterized as normal disc position, disc displacement with reduction (DDwR), and disc displacement without reduction (DDw/oR) according to the classification criteria for the disc position. 15
Normal disc position
Normal disc position was defined as the intermediate zone of the disc interposed between the condyle and articular eminence in both positions.
Disc displacement with reduction (DDwR)
DDwR was defined as an anteriorly displaced disc when the posterior band of the disc was located anterior to the 11:30 o’clock position and the intermediate zone of the disc was anterior to the condylar head in the closed position. Additionally, the disc was reduced on full mouth opening.
Disc displacement without reduction (DDw/oR)
DDw/oR was defined as an anteriorly displaced disc that was not reduced on full mouth opening.
Occluding pairs
The occluding tooth pairs, defined as pairs of upper and lower teeth that came into contact in centric occlusion, were calculated using both the clinical oral examination records and the silicon bite registration. 16 Bridge abutments and pontics were included for the calculations. We excluded removable dentures, teeth indicated for extraction, and pontics indicated for removal. 16 Posterior occluding pairs (range, 0–10) were defined as pairs of molars (including the third molars) and premolars that came into contact in centric occlusion. Anterior occluding pairs (range, 0–6) were defined as pairs of corresponding canines and incisors.
Cephalometry
Cephalograms at the first visit with teeth in centric occlusion were collected from the database of the radiology department. The images were analyzed using digital measurement software (Uceph, version 780, Chengdu, China) by independent observers who were blinded to the patients’ diagnoses. The reference plane was the Frankfort horizontal plane, and there were six angular measurements: ANB, SN-MP, PP-MP, U1-NA, L1-NB, and facial convexity angle (N′-Sn-Pg′) and 10 linear measurements: anterior cranial base (S-N), posterior cranial base (S-Ar), ramus height (Ar-Go), mandibular body length (Go-Me), facial depth (N-Go), posterior facial height (S-Go), anterior facial height (N-Me), U1-facial plane (U1-NPo), L1-facial plane (L1-NPo), and Pg′-NB (Figure 2). 17

Cephalometric landmarks used in this study.
Reliability
To classify the osseous diagnosis and disc position, two independent specialists evaluated the imaging results. Any doubt about the classification was evaluated decisively by a third specialist.
To determine the reliability of cephalometry, we tested the interobserver and intraobserver reliability. For interobserver reliability, 20 randomly-selected cephalograms were measured by the two observers, and the intraclass correlation coefficient (ICC) was calculated. To determine the intraobserver reliability, 20 randomly-selected cephalograms were first measured by each examiner. After a washout period of approximately 1 month, the same cephalograms were measured again by the observers, and the ICC was also calculated. All examiners with an ICC higher than 0.8 were qualified to measure cephalograms.
Statistical analysis
Patients with BOA were classified as the BOA group, and patients with BNJ were classified as the BNJ group. The values for the angular and linear cephalometric measurements in each group were evaluated and compared using SPSS (version 24.0 for Windows; IBM Corp., Armonk, NY, USA). The t-test was used when the data were normally distributed, and the Mann–Whitney U-test was used when the data were not normally distributed. Possible differences in the proportions for the patients’ genders, disc positions, and occluding pairs were tested with the chi-square and Fisher’s exact tests. All statistical tests were two-sided, and P values < 0.05 were considered significant.
Results
Reliability
The kappa coefficients for the osseous diagnosis and disc positions were 0.837 (P < 0.001) and 0.919 (P < 0.001), respectively. The interobserver ICC for cephalometry was 0.992 (P < 0.001), and the intraobserver ICC for each observer was 0.996 (P < 0.001) and 0.997 (P < 0.001), respectively.
Patients’ characteristics
Eighty-eight patients with a mean ± standard deviation (SD) age of 67.48 ± 6.72 years (57 women and 31 men) were included in this study. We excluded 18 unilateral and intermediate TMJOA cases because of the limited number, and ambiguity in the diagnosis, leaving 70 patients in the final analysis. There were 48 patients with BOA, followed by 22 with BNJ, and 10 with bilateral intermediate TMJOA. Four patients had unilateral TMJOA and a normal joint on the contralateral side; three patients had unilateral TMJOA and a joint intermediate for TMJOA on the contralateral side; and one patient had unilateral intermediate TMJOA and a normal joint on the contralateral side (Table 1). We excluded 18 unilateral and intermediate TMJOA cases because of the limited number and ambiguity in the diagnosis, leaving 70 patients in the final analysis. Fifty-five patients with TMD showed condylar osseous changes, and 20/70 patients had comorbidities.
Proportion of osseous diagnosis by gender.

There was no statistically significant difference for age, gender distribution, or comorbidities between the BOA group and BNJ group (P = 0.550, 0.684, and 0.332, respectively). There was also no statistically significant difference in the anterior, posterior, or total occluding pairs between the two groups (Table 2).
Differences in age, comorbidities, symptoms, duration, and occluding pairs between BNJ and BOA patients.
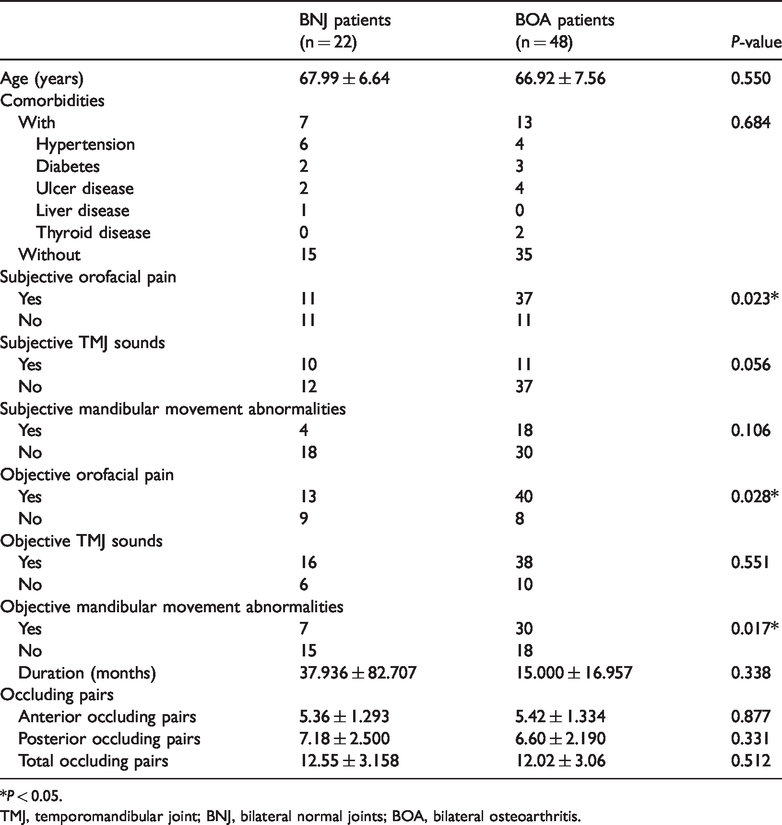
*P < 0.05.
TMJ, temporomandibular joint; BNJ, bilateral normal joints; BOA, bilateral osteoarthritis.
The presence of subjective and objective orofacial pain, and objective mandibular movement abnormalities in the BOA group were significantly higher than in the BNJ group (P < 0.05). There was no statistically significant difference in the presence of subjective TMJ sounds or self-reported abnormalities in mandibular movement. There was also no statistically significant difference in the duration of symptoms (Table 2).
The prevalence of DDwR in the BNJ group (16/22) was significantly higher than in the BOA group (P < 0.001). In contrast, the prevalence of bilateral DDw/oR and unilateral DDwR with DDw/oR in the contralateral TMJ in the BNJ group (1/22 and 1/22, respectively) was significantly lower in the BNJ group than in the BOA group (11/48 and 30/48, respectively, P < 0.001; Table 3).
Proportion of each disc position in BNJ and BOA patients.

*P < 0.05.
BNJ, bilateral normal joints; BOA, bilateral osteoarthritis; DDwR, disc displacement with reduction; DDw/oR, disc displacement without reduction; TMJ, temporomandibular joint; df, degrees of freedom.
Compared with the BNJ patients, BOA patients had a significantly greater ANB angle, PP-MP angle, L1-NB angle, U1-NPo distance, and L1-NPo distance; a shorter posterior cranial base (S-Ar), ramus height (Ar-Go), facial depth (N-Go), and posterior facial height (S-Go); and a smaller facial convexity angle (N′-Sn-Pg′; all, P < 0.05). There was no significant difference in any other cephalometric measurement between the two groups (Table 4, Figure 3).
Cephalometric analyses between BNJ and BOA patients.

*P < 0.05.
BNJ, bilateral normal joints; BOA, bilateral osteoarthritis; S, sella; N, nasion; Ar, articulare; Go, gonion; A, point A; B, point B; Me, menton; Pog, pogonion; N′, soft tissue nasion; Pg′, soft tissue pogonion; MP, mandibular plane; PP, palatal plane; U1, long axis of the central upper incisor; L1, long axis of the central lower incisor.
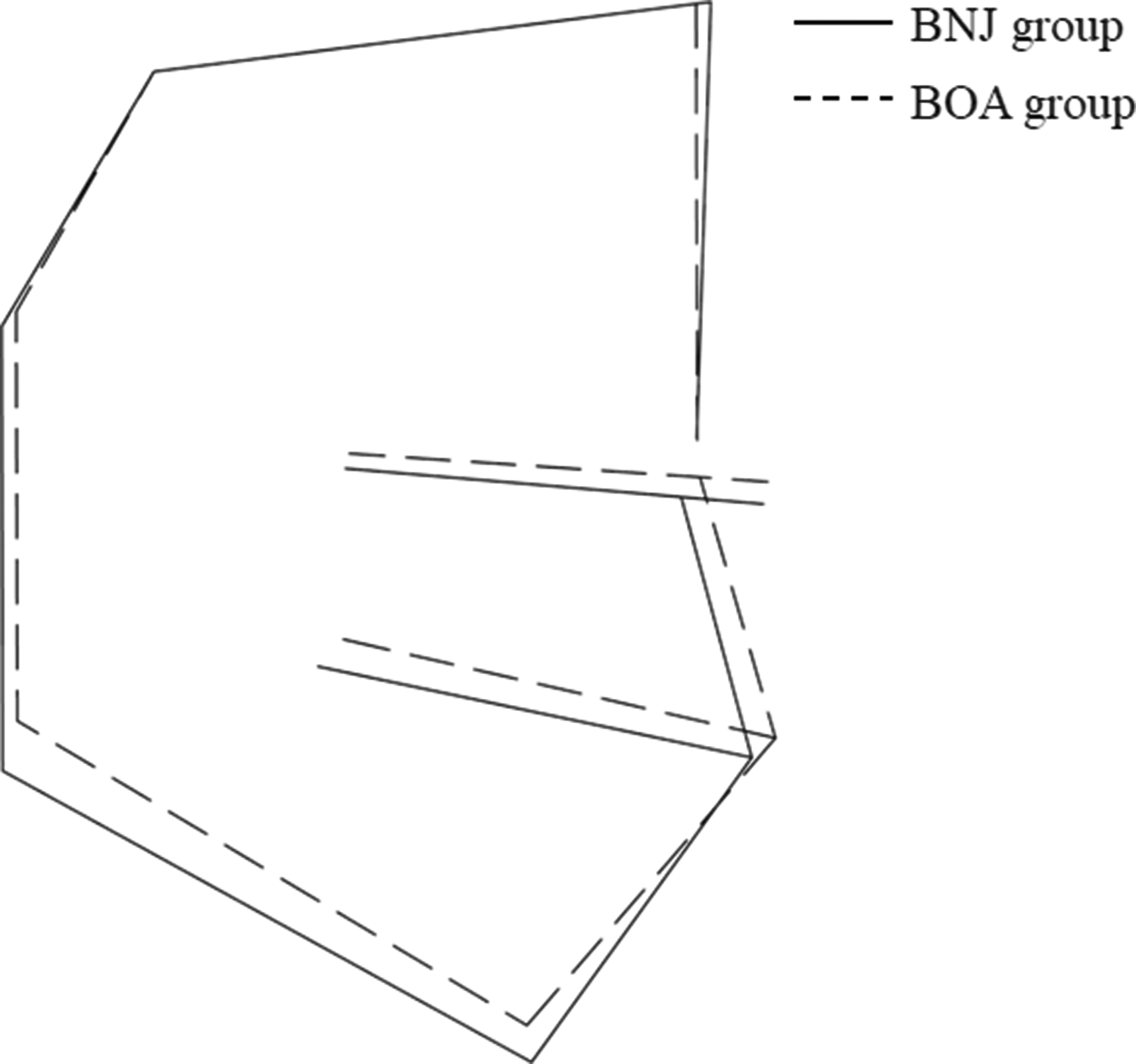
The mean cephalometric profilograms of the BNJ group (solid line) and BOA group (broken line).
Discussion
There was a high prevalence of TMD in the older population in this study, among whom TMJOA was commonly found. We investigated the proportions of different osseous diagnoses in these older patients with TMD and analyzed the differences in disc position, occluding pairs, and facial skeletal characteristics between BNJ patients and BOA patients. Compared with BNJ patients, BOA patients were more likely to have orofacial pain and a severely displaced disc. Both BOA and BNJ patients had a retruded mandible compared with Chinese norms, 18 and BOA patients had a shorter posterior cranial base, a more retruded and clockwise-rotated mandible, greater protrusion of the anterior teeth, and a more protruded lateral profile.
In the current study, 55 older TMD patients showed condylar osseous changes, which was significantly higher than the rate reported in younger TMD patients. 19 This result was consistent with the findings of previous studies in the general population,20,21 which suggests that aging might compromise the repair and remodeling capacity of the joint, and that TMJOA develops as individuals age.
DDw/oR is related to TMJOA in children and adolescents. 22 When there is no disk tissue between the temporal eminence and the condylar surface, changes in the cartilage and synovial membrane might lead to cartilage breakdown. When cartilage breakdown and bone degeneration exceed the repair rate, TMJOA might be detected clinically and radiologically. 23 Lei et al. 24 reported that in adolescents and young adults, the prevalence of early-stage TMJOA increased from 24.20% (30/124) to 60.60% (40/60) 1 month after closed lock TMJ occurred. In our study, a similar relationship between DDw/oR and TMJOA was found in older patients, suggesting an etiologic role of DDw/oR in the prevalence of TMJOA. Early diagnosis and treatment of DDw/oR might be helpful in the prevention of TMJOA.
In this study, there was no statistically significant difference in occluding pairs between BOA and BNJ patients. The overall dentition status of the patients who sought treatment for TMD in this study was relatively better than that of the general Chinese older population, 25 possibly because of selection bias. The prevalence of comorbidities was 20/70 in this cohort, which was lower than the general Chinese older population (43.62%, 5107/11707), suggesting that patients in this study had relatively better general condition. 26 Commonly, older people have concurrent systemic diseases with more severe symptoms affecting other areas of the body; therefore, they may be less likely to seek treatment for TMD because their TMD complaints do not outweigh their general health issues.
The posterior cranial base size was shorter in the BOA patients compared with the BNJ patients in this study, which was similar to results in previous studies showing that DDw/oR patients had a smaller posterior cranial base.27,28 Because craniofacial growth is mostly complete in the twenties, and BOA patients do not have chronic symptoms, it is possible that short posterior cranial base length might predispose to DDw/oR. However, TMJOA could begin in early life with asymptomatic osseous changes. 29 The possibility that craniofacial changes are consequences of TMJOA cannot be denied, currently. Although existing cross-sectional studies claimed that growth is a major reason for subsequent unfavorable TMJ loads 30 and compromised condylar development, further comprehensive longitudinal investigations are needed.
One limitation of this study was that detailed radiographic findings, such as osteophytes, subchondral cysts, and loss of joint space were not analyzed owing to the limited sample size. While this study might provide a framework for future research concerning older TMD patients, the sample size must be increased to enhance statistical power and precision, and develop our results further.
Conclusion
There was a high prevalence of TMJOA in the older TMD patients in this study, with severely displaced discs, resulting in more complaints of orofacial pain and mandibular movement abnormalities. TMJOA was associated with a shorter posterior cranial base and a retruded and clockwise-rotated mandible, and this relationship requires further verification.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Innovative Spark Project of Sichuan University (2018SCUH0082), the Technology Innovation Project of Science and Technology Bureau of Chengdu (2019-YF05–00508-SN), and the National Students’ Innovation and Entrepreneurship Training Program (202010610191 and 202010611511).