
Abstract
Objective
To study the safety and feasibility of implementation of precise radiotherapy with inducement of an apnea-like condition.
Methods
Two patients with lung tumors underwent precise radiotherapy under an apnea-like condition. The apnea-like condition was induced 11 times between the two patients for tumor localization and treatment. The changes in the blood oxygen saturation, blood pressure, heart rate, and end-tidal carbon dioxide during the apnea-like periods were observed, and the incidence of adverse reactions was recorded.
Results
The average apnea-like time was 6.2 minutes (range, 3–9 minutes), and the average radiotherapy time was 4.6 minutes (range, 1–7 minutes). The lowest blood oxygen saturation level was 97%, with a change of <1%. The heart rate and average arterial blood pressure increased during the apnea-like periods. Contact sores appeared on the patients’ posterior pharyngeal wall after the first apnea-like period; no other adverse events occurred.
Conclusion
Precise radiotherapy under an apnea-like condition is safe and feasible for patients with lung tumors.
Introduction
Precise radiotherapy with inducement of an apnea-like condition is the latest technology in the field of radiotherapy. 1 In 2009, this technique was first carried out in the proton therapy center in Munich, Germany. 2 It has since been safely carried out on thousands of patients. The development of modern medical precision therapy has made this technology possible.3–5 Precise radiotherapy under an apnea-like condition causes respiratory movements to completely disappear through the use of muscle relaxants under general anesthesia. 6 Because the two layers of splanchnic pleura stay close to each other, the lung remains still and the relative position of the tumor does not move. Radiotherapy can then be carried out while ensuring an oxygen supply to the patient. This allows for accurate localization of the tumor, an increased radiation dose to the tumor, and protection of the normal tissue. 7
Materials and methods
Patients
Patient 1 was an 80-year-old man. Two years after surgical treatment of colon cancer, re-examination revealed lung cancer. A biopsy was performed and the patient was confirmed to have a solitary pulmonary metastasis of colon cancer. He had an American Society of Anesthesiologists (ASA) physical status of III (severe systemic disease but not life-threatening) and cardiac function level of II.
Patient 2 was a 52-year-old man. He was hospitalized because of a 2-week history of hemoptysis. After a comprehensive examination, he was confirmed to have lung cancer. He had an ASA physical status of II (mild systemic disease) 8 and cardiac function level of II. Preoperative evaluation showed that both patients could tolerate general anesthesia and precise radiotherapy under an apnea-like condition.
Therapeutic method
Image-guided radiation therapy
Each patient’s skin marks were aligned with the room lasers in the treatment room, and two-dimensional (2D) kV orthogonal imaging was performed with an on-board imaging system (Varian Medical Systems, Palo Alto, CA, USA). The patient was then positioned on a translational couch and shifted to align the biopsy clip with the acquired images using the 2D/2D matching tool in the on-board imaging system. Finally, three-dimensional cone-beam computed tomography (CT) images were fused to confirm the clip and surrounding soft tissue.
Apnea-like procedure
Intramuscular atropine (0.5 mg) was administered before the operation. After entering the radiotherapy room, the venous channel was opened and the patient was placed in the radiotherapy position on the treatment table to allow for localization of the tumor. Anesthesia was started after 5 minutes of preoxygenation. Phencyclidine hydrochloride (0.5 mg), midazolam (0.04 mg/kg), etomidate (0.15 mg/kg), remifentanil (0.5 µg/kg), and cisatracurium besylate (0.25 mg/kg) were sequentially administered.
After the patient’s respiratory movements had disappeared, a laryngeal mask airway (LMA) was inserted into the laryngopharynx. After insertion of the LMA, the position of the LMA was secured by taping its integral bite block to the facial skin. The LMA was then connected to an anesthesia machine to control the patient’s respiration. Anesthesia was maintained by continuous infusion of etomidate and remifentanil. The lungs were mechanically ventilated with a constant oxygen flow rate of 4 L/minute through the LMA (tidal volume of 6 mL/minute, respiratory rate of 12 breaths/minute, and positive end-expiratory pressure of 6 cm to increase oxygenation).
The heart rate, blood pressure, blood oxygen saturation (SpO2), and end-tidal carbon dioxide (ETCO2) were continuously monitored and recorded every 2 minutes. After the radiotherapy, the anesthesiologist entered the radiotherapy room and a ventilator was connected to the patient. To allow for gradual discharge of the accumulated carbon dioxide, the tidal volume was 8 mL/minute, the respiratory rate was 12 breaths/minute, and the positive end-expiratory pressure was 6 cm. The patient was changed to controlled breathing, the anesthetics were discontinued, and the patient was sent to the recovery room. While waking up, the patient was intermittently given midazolam according to the changes in the heart rate and blood pressure to ensure that the vital signs remained stable. When the patient’s breathing recovered, atropine, neostigmine, and flumazenil were given as antagonists. After the patient’s conscious had returned, the stability of the vital signs was confirmed and the patient returned to the ward.
Six apnea-like procedures were performed for Patient 1 during the treatment period, including one apnea-like procedure during the CT scan to allow for localization of the tumor. The next day, the patient began receiving radiotherapy on a daily basis with five apnea-like procedures in total (Table 1). Five apnea-like procedures were performed for Patient 2 during the treatment period, including one apnea-like procedure during the CT scan to allow for localization of the tumor. The next day, the patient began receiving radiotherapy on a daily basis with four apnea-like procedures in total (Table 2).
Detailed data during radiotherapy under the apnea-like condition in Patient 1.
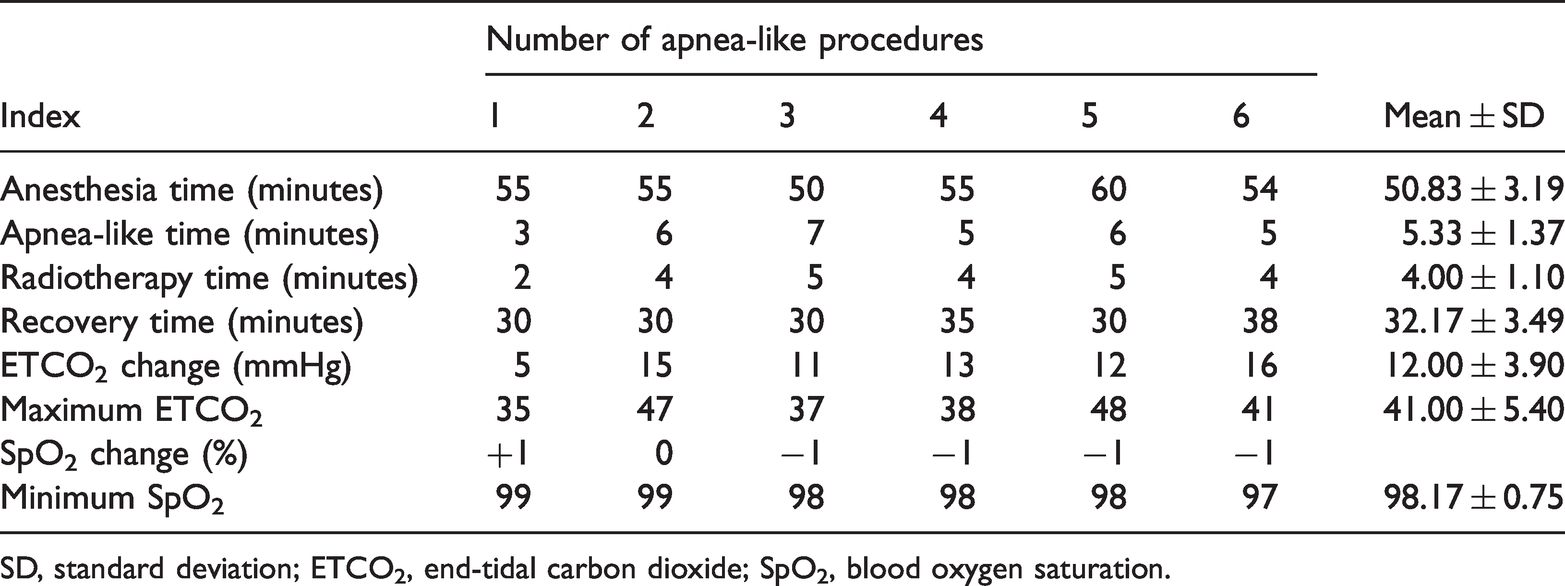
SD, standard deviation; ETCO2, end-tidal carbon dioxide; SpO2, blood oxygen saturation.
Detailed data during radiotherapy under the apnea-like condition in Patient 2.
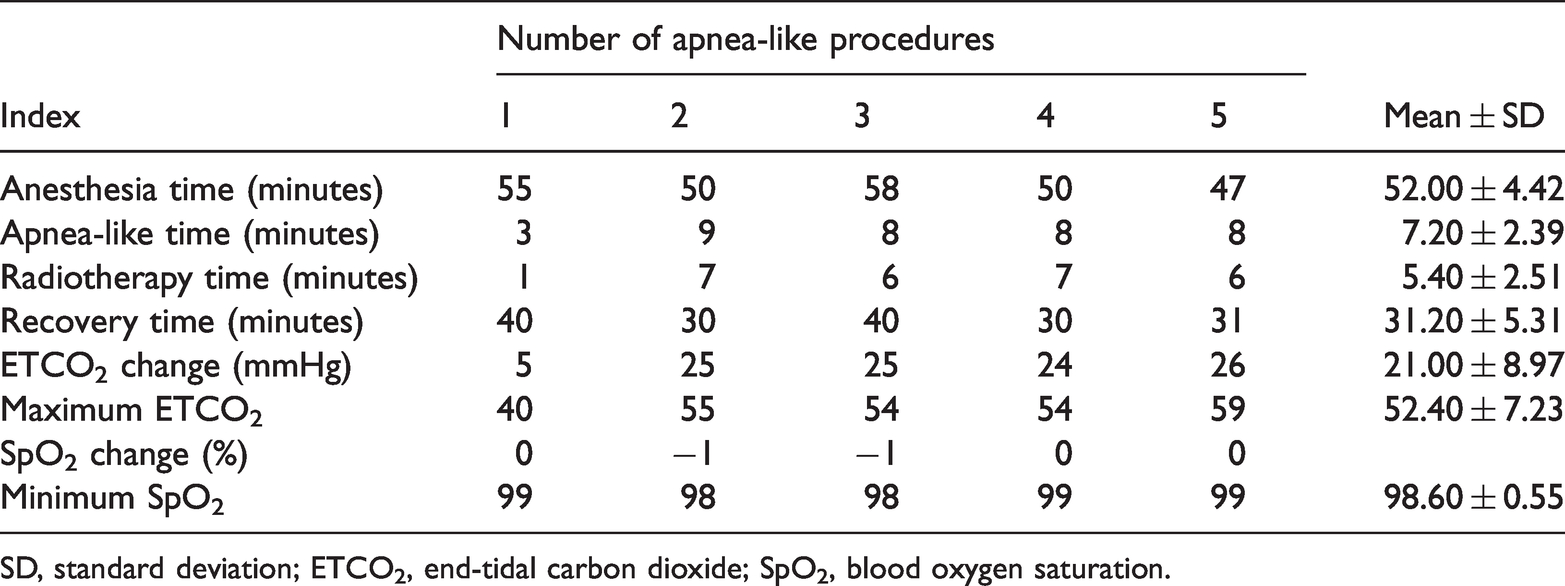
SD, standard deviation; ETCO2, end-tidal carbon dioxide; SpO2, blood oxygen saturation.
We only performed this treatment for two patients because patients with a significant cough, pain, or anxiety or with abdominal or shallow breathing patterns are not suitable for this technique.
This study was approved by the ethics committee of Wuwei Cancer Hospital of Gansu Province (No. 2016001). Written informed consent for publication of the report was obtained from the patients.
Results
The detailed data obtained during radiotherapy under the apnea-like condition are shown in Tables 1 and 2.
The average apnea-like time of the two patients was 6.2 minutes (range, 3–9 minutes), and the average radiotherapy time was 4.6 minutes (range, 1–7 minutes). The change in the SpO2 was <1%, and the lowest SpO2 was 97%. The average increase in the ETCO2 during the apnea-like period was 3.5 mmHg, and the highest ETCO2 was 59 mmHg (this occurred at the eighth minute under the apnea-like condition). The average anesthesia time was 53.5 minutes (range, 47–60 minutes), and the average recovery time was 33.1 minutes (range, 30–40 minutes). During the apnea-like period, the heart rate and the average arterial blood pressure were increased. After the first apnea-like procedure, contact sores appeared in the patients’ posterior pharyngeal wall; no other adverse events or side effects occurred.
Discussion
With the rapid development of CT and three-dimensional imaging technology, precise radiotherapy has become the mainstream technique in radiotherapy and is now the direction of future development. 9 The basic requirement of precise radiotherapy is to achieve a high dose in the target area and reduce the radiation to the surrounding normal tissues as much as possible; this will improve the gain ratio of the treatment. 10 Shifting of organs caused by respiratory movements results in deviation of thoracic and abdominal tumors with respiration; the tumors may even deviate outside of the radiation area established in the radiotherapy plan. 11
Therefore, breathing control has become a research area of particular interest. Scholars have proposed many methods with which to reduce tumor displacement caused by respiratory movement in radiotherapy, such as breath-holding techniques, respiratory gating technology, four-dimensional radiotherapy technology, 12 and real-time tumor tracking technology. However, all these methods have specific limitations, such as low accuracy, expensive equipment, and patient–ventilator asynchrony. 13 Precise radiotherapy under an apnea-like condition can stop all respiratory movements, and the relative position of the tumor no longer moves because muscle relaxants are administered under general anesthesia. 14 The radiotherapy can be carried out while ensuring an oxygen supply to the patient using a special oxygen supply method. This technique allows for accurate localization of the tumor, an increased radiation dose to the tumor, and protection of the normal tissue. Moreover, it can reduce the radiotherapy time and hospitalization duration, increase bed turnover, and decrease medical expenses. 15
Under normal circumstances, the oxygen reserve in a normal adults is completely depleted within 5 minutes of apnea; this is followed by asystole. 16 In our two patients, we conducted radiotherapy under general anesthesia and an apnea-like condition and used a special oxygen supply method to ensure no lack of oxygen during the apnea-like condition. Our data showed only an increase in the ETCO2 during treatment; there was almost no change in the SpO2. The blood pressure and heart rate remained normal. The number of radiotherapy procedures was reduced to five, and the duration of hospitalization was reduced from 6–8 weeks to 2 weeks.
This technology was first used in Germany in 2009, and it is now widely used in the proton therapy center in Munich, Germany. Research from this facility has shown that general anesthesia under an apnea-like condition is safe. 2 The apnea-like condition was implemented a total of 3025 times, and no adverse events occurred. 2 Oxygen and carbon dioxide exchange during respiration occurs primarily through diffusion, during which transport is driven by a concentration gradient. 17 The partial pressure of oxygen is much greater than the partial pressure of carbon dioxide. The basic principle of this technology is that oxygen is easier to diffuse in the lungs than carbon dioxide. Even without breathing, oxygen will diffuse into the alveoli because of the concentration gradient. With constant oxygen flow and pressure, the patient can maintain oxygenation without breathing; the oxygen is supplied through tracheal intubation. In the absence of respiration, the ETCO2 level will increase by 2 to 4 mmHg/minute. If the apnea-like time is short, there should be no negative effect on the patient.
This technique can greatly reduce the radiation field to avoid damage to normal tissue. This allows higher doses to the tumors and increases the opportunities for local tumor control. Several respiratory synchronization systems based on different types of organ motion detectors are currently used in radiotherapy.18–21 Tumor motion is tracked using direct (e.g., diagnostic X-ray imaging) or indirect tumor position detection. The indirect method estimates tumor displacement through chest wall motion, monitors the amount of air in the lungs, and measures changes in airflow temperature or changes in the cross-sectional area of the chest cavity.
Previous studies have adopted tracheal intubation, which is safer than laryngeal masks. However, the patient’s compliance and tolerance might be poorer, and the patient may not be able to tolerate repeated tracheal intubations. Previous studies have also shown that the movement range of thoracic and abdominal tumors during ordinary radiotherapy is 2 to 4 cm, while the movement range during precise radiotherapy under the apnea-like condition is only 0.1 to 0.2 cm. 17 The radiation-induced damage to the normal tissue was very mild, allowing the radiation dose to be increased. Additionally, the radiotherapy times and hospitalization duration are reduced. Therefore, precise radiotherapy under the apnea-like condition has great advantages in radiotherapy of thoracic and abdominal tumors, which are greatly affected by respiratory movement.
Careful comparisons of the efficacy and cost of precision radiotherapy are critical to defining the value of new medical technologies. Although the radiotherapy time and hospital stay of these two patients were greatly reduced, more clinical cases are needed to further confirm the overall benefit, including in patients with different stages of lung cancer.
Conclusion
Lung tumors can be more accurately located after breathing is stopped. Therefore, the suppressed target motion excludes normal lung tissues from the high-dose region. Precise radiotherapy will be more helpful for heavy ion and proton therapy.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The First Batch of Science and Technology Projects (WW160111).