
Abstract
Objective
To explore the relationship between temperament and character traits in Cloninger’s psychobiological theory and mental disorders.
Results
The pooled effect sizes obtained from 149 studies showed that high harm avoidance (related to 22/24 diagnostic categories), low self-directedness (21/23), low cooperativeness (17/23), high self-transcendence (14/23), low reward dependence (11/24), high novelty-seeking (10/24), low novelty-seeking (7/24), high persistence (2/23), low persistence (2/23) and high reward dependence (2/24) were related to psychopathology.
Conclusions
All traits provided unique psychobiological tools for differential diagnosis of mental disorders. However, high harm avoidance and low self-directedness played a canonical role in psychopathology. Despite the study limitations, additional studies are warranted to evaluate the differential diagnoses suggested by the present model.
Keywords
Introduction
Personality is one of the most challenging concepts in the fields of psychiatry and behavioural sciences, and has always generated debate about the relative merit of different theories and perspectives.1,2 Psychobiological theories of personality are based on Gray’s (1977) concepts of behavioural activation and inhibition systems. 3 The model developed by Cloninger (1986) is one of the most important psychobiological models; it includes the two domains of temperament and character, with seven subscales for clinical analysis.4,5 Over the last three decades, this temperament and character model has gradually attracted the attention of researchers and is now widely used.6–8 Cloninger’s original model introduced three temperament traits: harm avoidance (HA; a tendency to negative emotionality, such as excessive worrying, shyness, fearfulness, pessimism and becoming easily fatigued); novelty-seeking (NS; a tendency for exploratory activity in response to novel stimulation, impulsive decision making or behaviours, and avoidance of frustration) and reward dependence (RD; a tendency to verbal signals of social support and approval). 9 The trait of persistence (Ps; a tendency to perseverance and resilience despite fatigue or frustration), which was originally part of RD, was later separated into a new dimension. Although these four temperamental traits are affected by biological factors, Cloninger presented three other factors that are completely influenced by environmental conditions. 10 These factors are character traits that develop under the influence of the environmental context and improve intrapersonal and interpersonal functions. These character traits comprise self-directedness (SD; the skill and ability to regulate and adapt behaviour to achieve personal goals and values), cooperativeness (Co; a degree of general agreement and adjustment in interpersonal relationships) and self-transcendence (ST; the expansion of personal boundaries, such as spiritual ideas). 10
Cloninger’s temperament and character model uses a dimensional approach to personality evaluation. 11 In the last decade, the dimensional approach has represented normal and abnormal personality traits associated with psychopathology as two ends of a continuum. 12 In accordance with this dimensional approach, which has been recognized by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), mental health and psychopathology are not two separate and independent entities. 13 However, the dimensional approach assumes that not only abnormal personality but also psychopathology is generally situated on a personality continuum.14,15 This assumption highlights the need to examine the relationship between normal personality traits and psychopathology in the temperament and character model.
Although studies on the temperament and character model in psychopathology are few and scattered, previous reviews have provided interesting results.16–22 For example, Kampman and Poutanen (2011) found that high HA is associated with depressive traits, symptoms and treatment responses. 16 Other reviews and meta-analyses have also consistently emphasized the core role of high HA in mood and anxiety disorders such as social anxiety disorder (SAD), panic disorder (PD), obsessive–compulsive disorder (OCD), major depressive disorder (MDD), bipolar disorder (BD), psychotic conditions such as schizophrenia (SCZ), and eating disorders (ED), regardless of subgroups.17–22 In reviews that have examined character traits, low SD consistently appears in some diagnostic categories, such as MDD, BD, SAD, OCD, PD, post-traumatic stress disorder (PTSD), substance use disorder (SUD), SCZ and ED, regardless of subgroups.17,19,22 Despite the heterogeneity of findings related to other temperament and character traits, some studies have indicated the importance of high NS in alcohol use disorder (AUD) 23 and bulimia nervosa (BN),17,21 low NS in SAD, OCD, MDD and anorexia nervosa (AN),20,21 low RD in MDD and SCZ, 21 high Ps in BD and AN,17,20 low Ps in SCZ 21 and low Co in OCD and PD. 22 Although this body of research provides useful information, some limitations should be noted. First, these reviews have focused solely on one or more specific diagnostic categories. Second, some reviews examined temperament traits but not character dimensions. Third, the findings of some relatively more comprehensive reviews were not based on a meta-analysis and measurable effect sizes. Fourth, to our knowledge, no reviews or meta-analyses have examined the relationship between temperament and character traits and mental disorders, such as personality disorders, sleep disorders, and sexual dysfunction and somatoform disorders. Finally, a comprehensive and integrated map of the relationship between temperament and character traits and a wide range of mental disorders is lacking.
Drawing on the findings and limitations of previous reviews, we aimed to provide a comprehensive and integrated map of the association between the temperament and character traits of Cloninger’s psychobiological theory and psychopathology. Therefore, the present meta-analysis included all mental disorders, including previously neglected diagnostic categories, such as personality disorders, sleep disorders, sexual dysfunction and somatoform disorders. Character traits and temperaments for all diagnostic categories were analysed and measurable effect sizes for all diagnostic categories calculated. Additionally, we attempted to provide a coherent picture of the differential diagnosis of mental disorders using temperament and character traits. Drawing on previous review findings and our team’s experience in this area, several hypotheses were generated: i) there is a relationship between low SD and all diagnostic categories; ii) high HA is related to all diagnostic categories, except cluster B personality disorders, SUD and AUD; iii) high NS is correlated with cluster B personality disorders, SUD, AUD and BN, and there is a relationship between low NS and clusters A and C personality disorders, anxiety disorders, MDD and AN; iv) low RD is related to cluster A personality disorders, SCZ and MDD; v) there is a relationship between high Ps and obsessive–compulsive personality disorder (OCPD), AN and BN and between low Ps and MDD and SCZ; vi) low Co is related to all personality and anxiety disorders; vii) high ST is correlated with SCZ, SUD and all personality disorders; and viii) temperament and character traits have the potential to facilitate the differential diagnosis of mental disorders.
Methods
This meta-analysis was registered with PROSPERO (CRD42019133214) and the Kurdistan University of Medical Sciences, Sanandaj, Iran (MUK- 98724) (ethical approval number: IR.MUK.REC.1398.169). To investigate and determine the extensive associations between the temperament and character traits of Cloninger’s theory and psychopathology, the search had to cover all target diagnostic categories. The systematic review and meta-analysis followed the instructions in the 27-item checklist of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 24 in the selection of sources and databases, search strategies and selection criteria, quality assessment of studies and data extraction.
Sources, databases and search strategies
The meta-analysis included all articles published in English from January 1990 to April 2019. Systematic searches were performed of the international databases Cochrane, Web of Science, Scopus, PubMed, ProQuest, and Google Scholar. Author and reference searches were also performed to ensure that all articles related to the present objectives were identified.
Using previous reviews related to the study aims, suitable search keywords were determined by two members of the research team (AH and SK). Systematic searches of titles/abstracts were performed using a keyword list. Therefore, the same keywords were used to search for articles in all databases. Because of the wide range of keywords, searches related to each mental disorder category (personality disorders, anxiety disorders, mood disorders, thought disorders, sleep disorders, sexual disorders, EDs, OCD and related conditions, trauma-related disorders, somatoform disorder and related conditions, and alcohol/substance-related disorders) were carried out separately. A detailed keyword list is shown in Supplementary material 1.
Inclusion and exclusion criteria
All original articles published in academic journals from January 1990 to April 2019 were reviewed (total = 6933; database search = 6819; manual search = 114). The inclusion criteria were English-language articles (excluded n = 23) and studies on adults aged ≥18 years (excluded n = 441). In addition to duplicate records (n = 1655) and studies that did not involve temperament and character traits or mental disorders (n = 1550), the exclusion criteria were i) conference abstracts (n = 62) and articles without full text or unavailable full text (n = 35); ii) qualitative reports, dissertations and unpublished papers, experimental studies and other studies with an unsuitable/unrelated design (n = 1789); iii) studies containing non-standard interviews and instruments (according to the DSM and International Classification of Diseases) for assessing mental disorders or that did not use any versions of questionnaires related to Cloninger’s theory, such as the Temperament and Character Inventory (TCI), Temperament and Character Inventory-Revised (TCI-R), and Tridimensional Personality Questionnaire (TPQ) to assess temperament and character (n = 342); iv) studies that examined temperament/character traits and mental disorders but did not report relationships between these variables (n = 531); v) studies with non-human samples (n = 10) and those with results for a single population that were published separately in more than one article (n = 6); vi) studies related to other temperament theories (n = 181); vii) non-applicable case–control/correlation studies, such as those with less than three or more quantitative studies for each diagnostic category (n = 74); viii) studies on a non-specific disorder or that did not report subgroups (n = 11); ix) studies with no control group (i.e., participants without the main disorder but with/without other psychiatric disorders) and studies containing normative controls (n = 22); x) sectional or longitudinal studies with no reported correlations or means (standard deviations) for the baseline data (n = 37) and xi) reports with low-quality methodology (n = 15) based on the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement. These were studies that failed to report details of the objectives and methods, such as design and setting, procedures, samples and sampling, data sources, tools, variables, statistical methods, results, discussion and limitations. Thus, in line with the study objectives, studies with a cutoff point of ≤7 on the STROBE scoring sheet were excluded.
Although studies with non-original data, such as reviews and meta-analyses, were excluded from the analysis, the references of these studies were searched to ensure that all studies that met the present objectives were identified. Few studies used case–control designs, except some studies on borderline personality disorder (BPD) and antisocial personality disorder (ASPD). Thus, only correlational studies of personality disorder symptoms were analysed, and case–control studies were excluded. Although there were more than three case–control studies related to BPD and ASPD, to homogenize the data for all personality disorders, only correlation studies related to these two disorders were included in the meta-analysis. There were enough case–control studies on the other diagnostic categories to perform the meta-analysis. Finally, 149 articles were included in the meta-analysis.
Evaluation of study quality
The quality of studies was assessed using the STROBE checklist. 25 This 21-item checklist assesses the quality of a range of study types, including cross-sectional studies such as correlation, case–control, and causal–comparative designs (Supplementary material 2a). Two members of the research team (AH and SK) independently conducted the qualitative evaluation of the articles. Any disagreement between the two researchers was resolved through discussion with another researcher (KR).
Data extraction
Initially, a data extraction table was designed to organize the categorization and recording of the collected data. After evaluation of study quality and the exclusion of low-quality papers, the data from each study were entered into a table designed to record the results. The process of data synthesis included tabulation and detailed descriptions of the findings of each study and the organization of studies according to the following: author list, year, geographical region, and samples, including sample size and mean age (or age range) of participants, study design, statistical methods, research instruments, findings (including correlations or mean differences related to the current diagnosis), limitations and evidence level.
Data synthesis and analysis
Several meta-analyses were performed to calculate i) the pooled effect size of the correlation coefficients between each of the temperament/character traits (NS, HA, RD, Ps, SD, Co and ST) and personality disorder symptoms; and ii) the standardized mean difference (Cohen’s d) of the temperament and character traits between cases with different types of mental disorders and controls. Owing to the lack of coverage of some of the TCI/TPQ subscales in some studies, the number of studies entered into the meta-analyses related to each of the temperament and character traits was unequal. Studies related to personality disorder symptoms were combined according to sample size and correlations between variables. The unit of analysis was an individual study, and effect sizes in these meta-analyses were obtained using the Fisher z-transformation of correlation coefficients. Estimates of the correlation coefficients in individual studies were calculated for each temperament and character trait. In contrast, studies related to other mental disorders were combined according to sample size, mean and standard deviation of the variables in the case and control groups. Pooled effect sizes for group differences (cases vs. controls) are presented with 95% confidence intervals (95% CI). Finally, effect sizes (Fisher’s z for personality disorders and Cohen’s d obtained from case–control studies related to other mental disorders) were transformed into correlation coefficients. Thus, the temperament and character traits related to all diagnostic categories were compared using the same effect sizes. All hypotheses were tested at a p-value of <0.05 using the Comprehensive Meta-Analysis (CMA.2) software (Biostat Inc., Englewood, NJ, USA).
Egger’s test was used to detect possible publication bias. Because of heterogeneity (significant I2 or >50% in 87% of the studies), pooled estimates of the correlations and the standardized mean difference were calculated for all disorders using the random-effects method. 26 We studied the heterogeneity of the study samples using the I2 statistic for a 95% CI. A p-value <0.05 for I2 >50% was considered to indicate significant heterogeneity. The resulting pooled z-transformed correlation coefficients were back-transformed (z to r transformation) to the level of original coefficients to facilitate interpretation of the results. Additionally, the pooled standardized mean differences obtained from the case–control studies were transformed into correlation coefficients. These correlations were used to obtain a final model derived from effect sizes (r) of ≥0.10, according to Cohen. 27
Results
Studies included in the meta-analysis
The systematic literature search produced 6819 articles. Moreover, 114 papers were identified by author and reference searches. A total of 149 articles were entered into the meta-analysis. The study selection process based on the PRISMA checklist is shown in Figure 1. The results of the quality evaluation of articles using the STROBE checklist are shown in Supplementary material 2b. The quality of almost 90% of the articles was medium or higher. The quality of studies ranged from 9 to 20, and the median and mean were 16 and 15.1, respectively. These studies were conducted in the USA (n = 30), Italy (n = 23), Turkey (n = 13), Japan (n = 11), South Korea (n = 9), Germany (n = 6), Spain (n = 6), New Zealand (n = 6), Belgium (n = 5), Taiwan (n = 5), France (n = 4), Finland (n = 4), the UK (n = 3), Norway (n = 3), Canada (n = 3), Brazil (n = 3), the Netherlands (n = 2), Sweden (n = 2), Mexico (n = 2), Israel (n = 2), Poland (n = 1), Serbia (n = 1), Croatia (n = 1), the Czech Republic (n = 1), Iran (n = 1), India (n = 1) and South Africa (n = 1). A summary of the methods/results of the studies and the extracted information is shown in Supplementary material 3.

Flow diagram of the study selection process based on the PRISMA statement.
Figure 2 shows the final structure and system of the temperament and character traits related to psychopathology for differential diagnosis of mental disorders. The design of this figure was based on the significant correlations (r ≥ 0.10) between each of the temperament and character traits and all the diagnostic categories entered into the meta-analysis. Therefore, associations of <0.10 are not shown in this figure. The temperament and character traits are visible in dark frames and the different diagnostic categories in light frames. The different symbols and lines in this figure are used to clarify the importance of each of the temperament and character traits in related mental disorders.

Final structure and system of temperament and character traits related to psychopathology for differential diagnosis of mental disorders based on the comprehensive meta-analysis. All reported relationships have a significant effect size (r ≥ 0.10).
Twenty-four separate diagnostic classes were included in the meta-analysis. These psychiatric disorders comprised paranoid personality disorder (PPD; n = 14), schizoid personality disorder (SPD; n = 14), schizotypal personality disorder (STPD; n = 12), ASPD (n = 12), BPD (n = 14), narcissistic personality disorder (NPD; n = 14), histrionic personality disorder (HPD; n = 14), avoidant personality disorder (APD; n = 13), dependent personality disorder (DPD; n = 14), OCPD (n = 13), SAD (n = 8), PD (n = 12), generalized anxiety disorder (GAD; n = 4), OCD (n = 10), insomnia (n = 4), somatic symptom and related disorders (SSD; n = 7), MDD (n = 35), BD (n = 19), SCZ (n = 12), AUD (n = 8), SUD (n = 7), AN (n = 20), BN (n = 15) and binge ED (BED; n = 8). Mood disorders, EDs and personality disorders were the most frequently studied disorders. Following Cohen, 27 the number of effect size correlations for each TPQ/TCI dimension was as follows: HA (very large = 1; large = 5; medium = 9; small = 5; very small = 2), SD (large = 6; medium = 9; small = 6), Co (medium = 5; small = 12), NS (medium = 2; small = 14; very small = 1), ST (medium = 1; small = 13), RD (medium = 1; small = 10; very small = 2) and Ps (small = 4). Publication bias was identified for NS: SAD and MDD; HA: MDD, SCZ, BN, AN; RD: DPD; Ps: AN; SD: MDD, AN; Co: MDD, AN (p-values <0.05 for Egger’s statistic). The publication bias is shown in Table 1.
Meta-analysis results of the relationship between temperament/character traits and mental disorders

Note: The following disorders were included in the systematic review: sexual dysfunction, poor sleep quality, parasomnias, daytime sleepiness, OSA, RLS, PTSD, adjustment disorder, GAD (only Ps and the character traits), specific phobia, agoraphobia, selective mutism, ASAD, hoarding disorder, trichotillomania, hair-pulling disorder, excoriation disorder, skin-picking disorder, BDD, cyclothymic disorder, dysthymia, PMS, and factitious disorder. However, because of the small number of studies, these disorders were not included in the meta-analysis.
AN, anorexia nervosa; APD, avoidant personality disorder; ASAD, adult separation anxiety disorder; ASPD, antisocial personality disorder; AUD, alcohol use disorder; SUD, substance use disorder; BED, binge eating disorder; BD, bipolar disorder; BDD, body dysmorphic disorder; BN, bulimia nervosa; BPD, borderline personality disorder; Co, cooperativeness; DPD, dependent personality disorder; GAD, generalized anxiety disorder; HA, harm avoidance; HPD, histrionic personality disorder; MDD, major depressive disorder; NPD, narcissistic personality disorder; NS, novelty-seeking; OCD, obsessive–compulsive disorder; OCPD, obsessive–compulsive personality disorder; OSA, obstructive sleep apnoea; PD, panic disorder; PMS, premenstrual syndrome; PPD, paranoid personality disorder; Ps, persistence; PTSD, post-traumatic stress disorder; RD, reward dependence; RLS, restless legs syndrome; SAD, social anxiety disorder; SCZ, schizophrenia; SD, self-directedness; SPD, schizoid personality disorder; SSD, somatic symptom and related disorders; ST, self-transcendence; STPD, schizotypal personality disorder; TCI, temperament and character inventory.
Relationship of temperament and character traits with mental disorders
Table 1 shows the meta-analysis results of the relationship between temperament and character traits and all mental disorders. The number of studies and participants, pooled effect sizes (Fisher’s z for personality disorders and Cohen’s d for other mental disorders, transformed to correlation coefficients) with 95% CI, the standard z score, and p-values are presented separately for each mental disorder. The significant relationships in Table 1 can be summarized as follows. NS was related to 17 diagnostic categories (positively: PPD, ASPD, BPD, NPD, HPD, BD, AUD, SUD, BN, BED; negatively: SPD, APD, SAD, GAD, OCD, MDD, AN). HA was positively related to all the diagnostic categories (except HPD and SUD). RD was related to 13 diagnostic categories (positively: HPD and DPD; negatively: PPD, SPD, STPD, ASPD, NPD, APD, GAD, MDD, SCZ, AN, BN). Ps was related to 4 diagnostic categories (positively: OCPD and AN; negatively: MDD and SCZ). SD was negatively related to all diagnostic categories (except insomnia and AUD). Co was related to 17 diagnostic categories (all negatively: PPD, SPD, STPD, ASPD, BPD, NPD, APD, OCPD, SAD, OCD, MDD, BD, SCZ, SUD, AN, BN, BED), and ST was related to 14 diagnostic categories (all positively: PPD, SPD, STPD, ASPD, BPD, NPD, HPD, DPD, OCPD, insomnia (non-significant), BD, SCZ, SUD, BN).
Differential diagnosis of mental disorders by temperament and character traits
Table 2 presents a summary of the meta-analysis findings. Following Cohen, 27 the significant relationships are shown according to five effect size (r) categories: <0.10 (very small), ≥0.10 but <0.30 (small), ≥0.30 but <0.50 (medium), ≥0.50 but <0.70 (large) and ≥0.70 (very large). The largest effect sizes were found for high HA (GAD, SAD, PD, OCD, APD, MDD and SCZ), low SD (SAD, PD, OCD, SCZ, MDD and BN) and low Co (OCD). In Table 2, publication bias is shown by the * symbol. The final psychopathology model was derived from effect sizes (r) ≥0.10 in the current meta-analysis. Differential diagnoses of mental disorders using the temperament and character traits of Cloninger’s psychobiological theory are shown in Figure 2.
Summary of the meta-analysis findings.
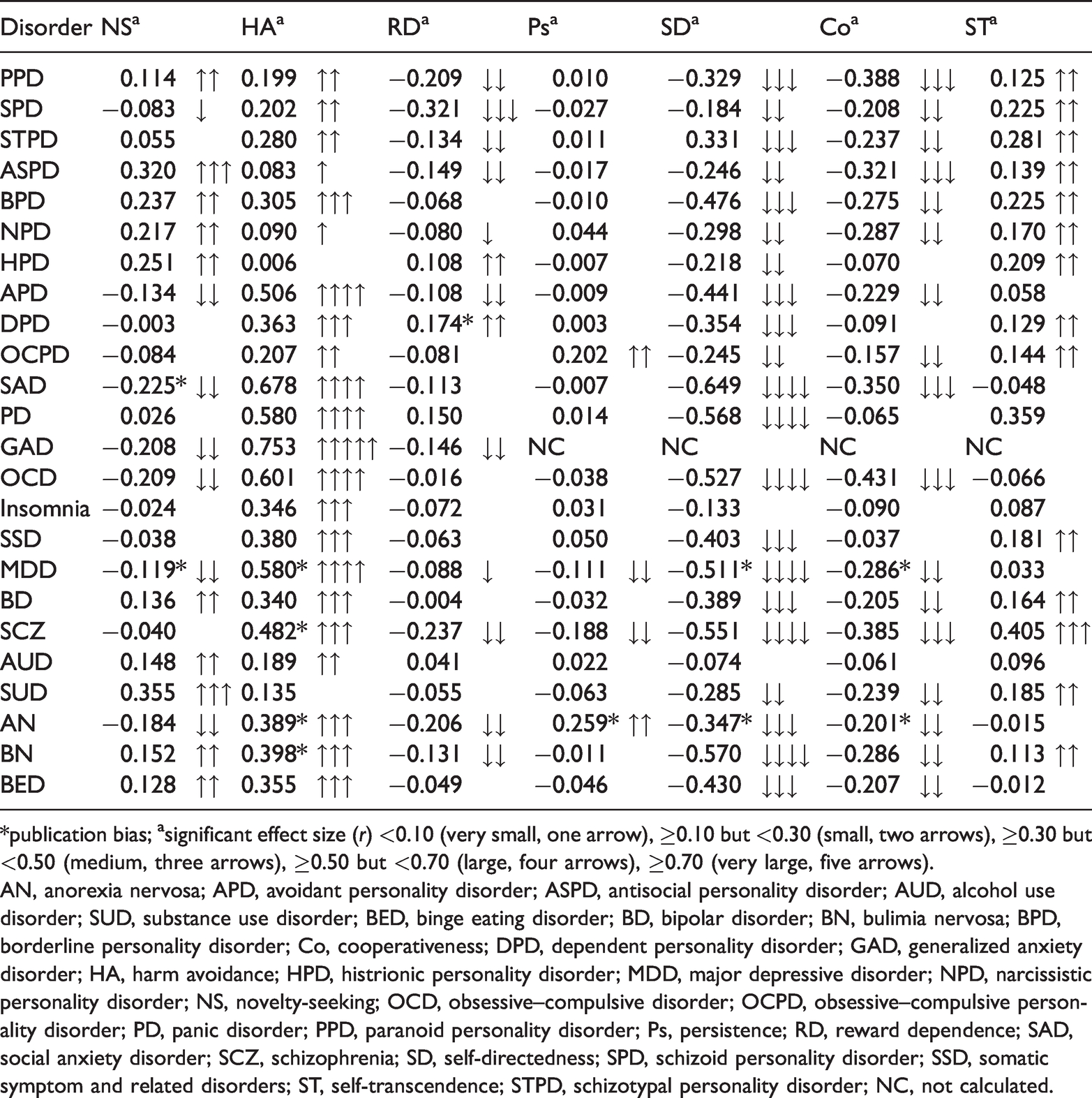
*publication bias; asignificant effect size (r) <0.10 (very small, one arrow), ≥0.10 but <0.30 (small, two arrows), ≥0.30 but <0.50 (medium, three arrows), ≥0.50 but <0.70 (large, four arrows), ≥0.70 (very large, five arrows).
AN, anorexia nervosa; APD, avoidant personality disorder; ASPD, antisocial personality disorder; AUD, alcohol use disorder; SUD, substance use disorder; BED, binge eating disorder; BD, bipolar disorder; BN, bulimia nervosa; BPD, borderline personality disorder; Co, cooperativeness; DPD, dependent personality disorder; GAD, generalized anxiety disorder; HA, harm avoidance; HPD, histrionic personality disorder; MDD, major depressive disorder; NPD, narcissistic personality disorder; NS, novelty-seeking; OCD, obsessive–compulsive disorder; OCPD, obsessive–compulsive personality disorder; PD, panic disorder; PPD, paranoid personality disorder; Ps, persistence; RD, reward dependence; SAD, social anxiety disorder; SCZ, schizophrenia; SD, self-directedness; SPD, schizoid personality disorder; SSD, somatic symptom and related disorders; ST, self-transcendence; STPD, schizotypal personality disorder; NC, not calculated.
Discussion
The aim of the present study was to explore the association between the temperament and character traits of Cloninger’s theory and mental disorders. The systematic review showed that a relatively large number of studies have examined the relationship between temperament and character traits and all mental disorders. The key findings of this systematic review and meta-analysis are as follows:
Although many associations were found, very few studies have examined trauma-related disorders such as PTSD, sleep disorders, sexual dysfunction and some anxiety disorders (e.g., GAD). There are extensive, complex and distinct relationships between each of the temperament and character traits and the different types of mental disorders. HA and SD are canonical traits and the core traits associated with psychopathology. Compared with HA and SD, NS and Co are secondary core traits associated with psychopathology. RD and ST are important traits related to SCZ and cluster A personality disorders. Compared with other temperament and character traits, Ps may show the weakest association with psychopathology.
Consistent with previous findings,17–22 the most important finding of the present meta-analysis was that HA and SD play a fundamental role in psychopathology. HA is a biological trait associated with the behavioural inhibition system, and seems to have a strong relationship with psychopathology. This trait substantially hinders an individual’s ability to modulate anxiety responses. Although HA has been proposed as an independent trait of other temperament and character traits, it may have a negative effect on SD. Conversely, low SD may facilitate psychopathology if combined with high levels of HA. This finding has already been well documented in a review study by Fassino et al. 22 The findings for each temperament and character trait are discussed below.
Novelty-seeking (NS)
The present meta-analysis findings support the third hypothesis that NS is positively related to all cluster B personality disorders and PPD. NS showed the strongest relationship with ASPD, and showed a weaker negative relationship with APD and SPD. These findings are consistent with the claims of Cloninger et al.9,10 Cluster B personality disorders are directly related to impulsivity, which is a lower-order NS trait. Both NS and impulsivity are strongly influenced by dopaminergic activity.28,29 Previous reports have also reported a negative relationship between NS behaviours and the Five Factor Model (FFM) agreeableness/conscientiousness.29–31 However, because of the lack of previous review studies on personality disorders, the present findings are novel.
Of the anxiety disorders, OCD, SAD and GAD showed a strong negative relationship with NS, whereas there was no significant relationship between NS and PD. These findings are consistent with a previous review by Kampman et al. 20 of studies on OCD, SAD and PD. Regarding GAD, previous reviews have been unable to provide a detailed analysis because of the relative lack of studies. However, we tried to examine the relationship between this disorder and temperamental traits, including NS. The present analysis confirmed that there was a negative relationship between GAD and NS. Regarding mood disorders, NS was negatively related to MDD and positively related to BD. This indicates a difference in the biological roots of the two disorders. Previous reviews21,22 have also associated low NS with MDD, but have linked high NS with BD. The present findings showed that NS is positively associated with drug-related disorders (SUD and AUD) and some EDs, including BN and BED. Finally, there was a negative relationship between NS and AN. The present findings on the associations between temperament and drug-related disorders and EDs are consistent with previous reviews.17,18,21,23
Harm avoidance (HA)
The second hypothesis was also supported: HA was positively related to all diagnostic categories (except HPD and SUD). This supports the claims of Fassino et al. 22 that HA is the biological core of personality and is associated with psychopathology. However, the HA effect sizes for cluster B personality disorders (except BPD) were small; this could be explained by the high levels of NS in this cluster. The largest effect sizes for HA were related to GAD, SAD, OCD, PD, MDD, APD and SCZ, in that order. These findings are consistent with previous reviews related to anxiety disorders, mood disorders, thought disorders and other axis I diagnostic categories.16–22,32 Some disorders, such as STPD, DPD, OCPD, PD, SSD and insomnia, showed a positive relationship with HA but no significant relationship with NS. These findings are also novel, and could be used to inform therapeutic interventions for some personality disorders, insomnia disorder and somatoform illnesses. Although the present study provides new information about the association between temperament and SSD, our recent comprehensive review explains the relationship between temperament/character traits and somatoform disorders. 33
HA was associated with many psychopathological disorders; a particularly interesting finding was its relationship with GAD. The correlation between HA and GAD was the only one that had a very large effect size (≥0.70) of all the anxiety disorder–diagnostic category associations. HA is strongly influenced by GABAergic activity and GABA neurotransmitter effects. 28 This neurotransmitter is a canonical biomarker in the modulation of anxiety responses, and impairment in GABA function is often associated with intense feelings of fear and anxiety. 34 SUD showed no significant relationship with HA, and (compared with other disorders) AUD was only moderately related to HA. This is consistent with a previous review by Howard et al. 23 These heterogeneous results for the correlations between HA and SUD and between HA and AUD could also be explained by the difference between type I and type II personality disorders. Type I alcoholism, which is influenced by genetic and environmental factors and begins after the age of 25 years, is associated with HA. Conversely, type II alcoholism, which is genetic and begins before the age of 25 years, is associated with NS. 35 A review by Oreland et al. 36 indicates the genetic and temperamental roots of types of alcoholism.
Reward dependence (RD)
The fourth hypothesis was that there would be a negative relationship between RD and symptoms of cluster A personality disorders, SCZ and MDD. Although the findings confirmed this hypothesis, the effect size associated with MDD was very small. Additionally, RD was negatively associated with some eating and anxiety disorders. The largest effect sizes for RD were for SPD, SCZ, PPD, AN, ASPD, GAD, STPD and BN, in that order. Therefore, people with cluster A personality disorders, EDs and schizoaffective disorders seem to be most vulnerable to RD. Although we found no previous comprehensive reviews or meta-analyses with which to compare our results, these findings are consistent with previous reviews of EDs and schizoaffective disorders.17,21 RD is associated with a lack of sensitivity to social reward and social detachment.9,10 Although RD is an independent psychobiological factor, the avoidant attachment style and social distance characteristics of these disorders are likely to be associated with severe HA. 37 According to Cloninger, 9 high HA and RD simultaneously lead to passive avoidance and dependent demanding. DPD and HPD were both positively associated with RD. This is consistent with the original model proposed by Cloninger. 9 Attention-seeking in HPD and a tendency to dependence, extreme intimacy, social attachment and need for affirmation in DPD are likely to be behavioural manifestations of RD.
Persistence (Ps)
In support of the fifth hypothesis, high Ps was associated with OCPD, AN and BN, and low Ps was associated with MDD and SCZ. Therefore, the results showed a positive relationship between Ps and AN and OCPD and a negative relationship between Ps and SCZ and MDD. Contrary to expectation, no significant relationship was found between Ps and BN. Although we found no previous reviews of OCPD, approximately 60% of individual studies found a significant positive relationship between OCPD and Ps. However, previous reviews have reported an association between AN and this temperamental trait.21,22 Although a review by Miettunen and Raevuori 21 found an association between low Ps and SCZ, findings from studies of patients with MDD are not in line with the present results.19,21,22 Ps has been studied less than other temperaments because it is a subscale of RD in the TPQ. This may have led to biases related to RD in studies that have used the TPQ.
Self-directedness (SD)
The first hypothesis predicted a negative relationship between low SD and all diagnostic categories. The findings showed that SD was negatively related to all diagnostic categories, except insomnia and AUD. This finding is consistent with evidence from previous reviews and meta-analyses17,19,22 and confirms the canonical role of SD in psychopathology. However, there is little understanding of the relationships between character traits and sleep disorders and AUD. A review by Oreland et al. 36 mainly focused on temperamental traits related to AUD rather than character traits such as SD. Regarding other diagnostic categories, the largest effect sizes for SD in the present study were related to SAD, BN, PD, SCZ, OCD, BPD, APD and SSD, in that order. Therefore, anxiety and schizoaffective disorders, personality disorders, EDs and somatoform disorders seem to have the most SD abnormalities. Both SD and HA seem to play a central role in the development and progression of mental disorders. 22 Low levels of SD indicate low self-esteem and identity problems, and an inability to devise long-term goals and accept responsibility. 28 SD is one of the strongest correlates of the FFM conscientiousness dimension. 29 SD is related to emotional dysregulation, which may explain its association with development and progression of mental disorders. 38 It is possible that we found no relationship between SD and insomnia and AUD because of the small number of studies on these disorders included in the analysis. Future reviews that include more studies on these disorders may provide different results.
Cooperativeness (Co)
The sixth hypothesis was that low Co is related to all personality and anxiety disorders. Our results showed that Co was negatively related to all personality and anxiety disorders, except HPD, DPD and PD. Generally, Co was negatively related to the 17 diagnostic categories. The largest effect sizes were related to OCD, PPD, SCZ, SAD and ASPD, in that order. Therefore, abnormalities associated with this character trait are not focused on a specific diagnostic category. This suggests that the Co dimension is impaired in most mental disorders, regardless of the type of diagnosis. Co represents interpersonal relationships and functions such as empathy and intimacy. The factor is one of the strongest correlates of FFM agreeableness. 29 A review by Fassino et al. 22 indicated the important role of Co in a wide range of mental disorders. It should be noted that the number of studies that featured Co and diagnostic categories was very small: OCD (n = 5), PD (n = 5), SAD (n = 4), SSD (n = 3), SUD (n = 7), AUD (n = 6) and insomnia (n = 4). Therefore, additional studies are needed to further investigate these associations.
Self-transcendence (ST)
The seventh hypothesis predicted that high ST would be associated with SCZ, SUD and all personality disorders. This hypothesis was mostly confirmed, although there was no association between ST and APD. ST was positively related to several diagnostic categories. The largest effect sizes were related to SCZ, STPD, SPD, BPD and HPD, in that order. Although the relationship between this character trait and PD was not statistically significant, the effect size was substantial. ST has been studied less than the other six components of Cloninger’s theory. Therefore, our analysis of this trait was not informed by many studies. However, the present results emphasize the key role of this factor in personality and thought disorders compared with other diagnostic categories. ST, especially if associated with SD and Co, can express maturity and spirituality. Conversely, when it is associated with low SD and Co, it can indicated a serious personality disturbance. 28 ST mainly manifests in magical thinking, dissociative tendencies and dysfunctional strategies to overcome fear and worry. Like other character dimensions, this factor requires further study.
Methodological considerations and limitations
Almost all the studies included in the present meta-analysis were cross-sectional and showed moderate heterogeneity (Supplementary material 3). Because of the relatively small number of longitudinal studies, it is not possible to infer causal relationships between temperament/character traits and psychopathology. Additionally, illness and/or its treatment may change a person’s temperament. The meta-analysis of personality disorders relied on correlational studies, whereas other psychiatric disorders examined in case–control studies were analysed using the standard mean difference. Although the extracted model is based on the same effect sizes (r) of ≥0.10, 27 this unavoidable discrepancy in data analysis should be noted. The case–control studies of personality disorders were excluded because of their limited number. Although this allowed more concordance with the dimensional approach (without a cutoff point) of DSM-5, case–control studies provide more valuable results than correlational studies. In fact, the samples in the personality disorder studies were a combination of general and clinical populations. The use of case–control studies containing samples with a definite diagnosis of personality disorder may provide more valid findings. Another limitation is the comorbidity between personality disorders and other mental disorders. Psychiatric disorders are not usually independent but are often comorbid with personality disorders.39,40 This may reflect the complex relationship between temperamental traits and mental disorders. In the present meta-analysis, nearly two-thirds of studies did not consider personality disorders comorbid with other mental disorders. The co-occurrence of personality disorders with other psychiatric conditions may lead to severe bias in research findings and conclusions. This may prompt temperament and character trait abnormalities caused by personality disorders to be wrongly attributed to other psychiatric conditions.41–43 This problem characterizes other psychiatric comorbidities such as depression, SCZ, and AUD and SUD. Therefore, future studies should focus on analysing mental disorders that show no comorbidity with personality disorders. In this study, we did not analyse temperament and character traits in men and women separately. Because the results of case–control studies are affected by gender differences, gender-specific analyses could prevent potential biases. In particular, most of the studies in the field of EDs and alcohol/drug abuse disorders focused on either the female or male population.
There was little significant publication bias, and the effect sizes (r) ≥0.10 used in the proposed model indicated relatively strong and significant relationships. However, it should be noted that there was significant publication bias associated with MDD and AN. Because of the small number of adequate studies, some disorders (e.g., PTSD and various sleep and sexual disorders) were not included in the meta-analysis and the final model. Additionally, some disorders that were included in the analysis had few studies, especially on character dimensions. Therefore, further studies are needed to confirm the present findings for SAD, PD, GAD, OCD, insomnia, SSD, AUD, SUD and BED. Future meta-analyses are needed with a larger number of studies to address the challenges encountered in the present study.
Conclusions
Generally, a large number of studies (mainly cross-sectional studies) have focused on the association between the temperament and character traits of Cloninger’s theory and mental disorders. Studies have particularly investigated mood disorders, EDs, personality disorders, SCZ and some anxiety disorders, such as PD. There are far fewer studies on trauma-related disorders, sleep and sexual disorders, alcohol/drug abuse disorders, somatoform disorders, OCD and some anxiety disorders. The results of this meta-analysis indicate that HA and SD (associated with approximately 90% of mental disorders) are core personality traits associated with psychopathology. High levels of HA may engender psychopathology if combined with low SD. Other temperament and character traits related to psychopathology include NS and Co (associated with approximately 70% of mental disorders), ST (associated with approximately 55% of mental disorders), RD (associated with approximately 50% of mental disorders) and Ps (associated with approximately 15% of mental disorders). These results indicate that the character dimensions (particularly SD and Co) are a useful tool that indicates the presence and severity of psychopathology. However, all temperament dimensions (regardless of whether the relationship between temperament and mental disorders is positive or negative) are unique psychobiological tools for the differential diagnosis of a wide range of mental disorders.
Although the meta-analyses produced relatively large effect sizes for most mental disorders, publication bias related to some disorders and low evidence levels for more than 80% of the studies are important challenges. Lack of access to many case–control studies of personality disorders and participant heterogeneity (evaluation of the severity of symptoms in clinical and non-clinical samples) are other important limitations. In addition, most of the studies in this meta-analysis were conducted in only a few countries and so are not representative of the global population. However, the evidence-based model used in this study could provide a basis for future studies. Subsequent studies could focus on disorders that have received less research attention and therefore were not included in the present model. The mental disorders mentioned in the above discussion of the study limitations could be the focus of future analysis. Biomarkers are important in the pharmacotherapy of psychopathology. Therefore, additional studies are warranted that evaluate the differential diagnoses in the current model.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211070766 - Supplemental material for Comprehensive meta-analysis of associations between temperament and character traits in Cloninger’s psychobiological theory and mental disorders
Supplemental material, sj-pdf-1-imr-10.1177_03000605211070766 for Comprehensive meta-analysis of associations between temperament and character traits in Cloninger’s psychobiological theory and mental disorders by Saeid Komasi, Farzin Rezaei, Azad Hemmati, Khaled Rahmani, Federico Amianto and Jouko Miettunen in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211070766 - Supplemental material for Comprehensive meta-analysis of associations between temperament and character traits in Cloninger’s psychobiological theory and mental disorders
Supplemental material, sj-pdf-2-imr-10.1177_03000605211070766 for Comprehensive meta-analysis of associations between temperament and character traits in Cloninger’s psychobiological theory and mental disorders by Saeid Komasi, Farzin Rezaei, Azad Hemmati, Khaled Rahmani, Federico Amianto and Jouko Miettunen in Journal of International Medical Research
Footnotes
Availability of data and materials
Data sharing is not applicable, as no new data were collected (all referenced studies are in the public domain).
Acknowledgements
This article is part of Mr. Saeid Komasi’s Ph.D. thesis, entitled Review and reconsideration of Hierarchical Taxonomy of Psychopathology (HiTOP) model with an emphasis on psychobiological models in the explanation of somatoform disorders. This author has received financial support and sponsorship from the Neurosciences Research Center and the Vice-Chancellor for Research and Technology of Kurdistan University of Medical Sciences, Sanandaj, Iran (ID: 98724).
Authors’ contributions
All authors collaboratively designed and conducted the study. The search process, analysis of the data and the writing of the manuscript were carried out by SK with support from FR, AH and KR, who supported the study and the writing process with ideas and feedback. The critical review process was performed by FA and JM. All authors have read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: The project was funded by the Kurdistan University of Medical Sciences, Sanandaj, Iran (ID: 98724).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.