
Abstract
Objective
To examine the prognostic factors and features of post-traumatic endophthalmitis.
Methods
This retrospective study enrolled adult patients (>18 years old) diagnosed with post-traumatic endophthalmitis. Their medical records were reviewed and the patient demographic characteristics, features of injury, management, outcomes and microbiology data were analysed.
Results
A total of 131 eyes from 131 patients were enrolled. Post-traumatic endophthalmitis was more common in male patients (122 of 131 patients: 93.1%), in those aged 30–44 years (51 of 131 patients: 38.9%), in those injured with a metallic object (86 of 131 patients; 65.6%), in those with a penetrating injury (90 of 131 patients; 68.7%) and those that were injured at work (106 of 131 patients; 80.9%). The mean ± SD time of presentation to the hospital and developing endophthalmitis was 40.60 ± 19.32 h and 5.19 ± 2.55 days, respectively. Of the cultures, 84 of 131 (64.1%) were negative and 22 of 131 (16.8%) were positive for Staphylococcus species. Patients with delayed presentation, an intraocular foreign body, traumatic cataract, retinal detachment, larger wounds, positive smears and cultures and work-related injuries had worse outcomes.
Conclusion
Immediate presentation to an ophthalmic centre and timely diagnosis and intervention may lead to better outcomes.
Introduction
Post-traumatic endophthalmitis occurs in 4–16% of open-globe injuries accounting for 25–30% of all cases of endophthalmitis. 1 Endophthalmitis following open-globe injuries is uncommon, but the poor visual outcome and its vision-threatening nature make it a significant entity. Compared with postoperative endophthalmitis, the incidence of post-traumatic endophthalmitis is 10-times higher and its prognosis is worse due to more virulent organisms and concurrent damage.1,2
Due to the lack of relevant studies in the Middle East in recent years, the present study examined the prognostic factors and features of post-traumatic endophthalmitis either at presentation (i.e. before repair) or after primary repair surgery. The study describes the demographic information, characteristics of injury, clinical presentation, management, microbiological results and their relationship with final outcomes in adult patients (>18 years old) presenting to Farabi Eye Hospital, Tehran.
Patients and methods
Patient population
This retrospective study enrolled consecutive adult patients (>18 years old) diagnosed with post-traumatic endophthalmitis between January 2015 and December 2019 at Farabi Eye Hospital, which is the largest ophthalmic centre in Iran. The total number of cases with open-globe injury during the same period was extracted to calculate the incidence of post-traumatic endophthalmitis. Patients with incomplete medical records and inadequate follow-up visits (<9 months) were excluded from the study.
Based on the medical history and examination, an orbital computed tomography scan was performed to rule out the presence of an intraocular foreign body (IOFB) in high-risk patients. Open-globe injury was diagnosed via slit-lamp or intraoperative examination. Endophthalmitis diagnosis was clinically and occasionally confirmed with the presence of a microorganism in microbiological evaluations.
An appropriate surgical plan was scheduled for IOFB removal dependent on the location of the foreign body and the other conditions. The injuries were repaired as soon as possible using 10-0, 9-0 and 8-0 nylon sutures for corneal, limbal and scleral lacerations, respectively. Prophylactic subconjunctival 50 mg cefazolin (0.5 ml of 100 mg/ml) was injected at the end of the primary repair. Lensectomy was undertaken if the traumatic cataract was significant. Primary intraocular lens was not implanted. Systemic antibiotics were administrated for 3 consecutive days. Routine 750 mg ciprofloxacine oral twice a day is used for adult cases of open-globe injury at Farabi Eye Hospital except in patients with oral intolerance or signs of post-traumatic endophthalmitis in whom 1 g vancomycin intravenous twice a day and 1 g ceftazidime intravenous three times a day are used. Topical 0.5% chloramphenicol (every 6 h for 1 week), 0.1% betamethasone (every 4 h on a tapering strategy for 1 month) and 2.0% homatropine (every 8 h for 1 week) were initiated after primary repair. During the postoperative visits, the signs of endophthalmitis such as poor red reflex, presence of hypopyon, vitritis, lid oedema and inappropriate pain were carefully noted. Patients with suggestive examination for endophthalmitis were scheduled for immediate pars plana vitrectomy or intravitreal injection of 1 mg/0.10 ml vancomycin and 2.25 mg/0.10 ml ceftazidime based on clinical condition and surgeon’s decision. Also, vitreous and anterior chamber samples were taken through vitrectomy or standard aspiration technique for microbiological examination.
This research was undertaken in accordance with the Declaration of Helsinki and approved by the Farabi Eye Hospital Institutional Review Board (no. 99-35267). Written informed consent was provided by the study participants for the publication of this report.
Data collection
The medical records of patients were reviewed and the patient demographics, features of injury, characteristics of injuring object, management, outcome and microbiology data were analysed. Slit-lamp examination and visual acuity measurements were undertaken for all of the patients. A detailed medical history was taken to classify the trauma mechanism in which globe rupture was defined as an injury by blunt trauma, whereas penetrating or perforating injury originated from a sharp object. Open-globe injury was defined as a full-thickness laceration in the eyeball including the cornea, sclera or both. The classification was made according to the Ocular Trauma Classification System. 3 The reporting of this study conforms with the STROBE guidelines. 4
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA). For eyes with a visual acuity of ≥20/800, logMAR was calculated and used for statistical analysis. If visual acuity was <20/800, following measurements of logMAR were used: counting fingers = 2.3, hand motion = 2.6, light perception = 2.9 and no light perception (NLP) = 3.1. Data are presented as mean ± SD, median (range) and frequency (%). Independent samples t-test and analysis of variance were used to compare the different groups. A P-value <0.05 was considered statistically significant.
Results
A total of 163 eyes from 163 adult patients were considered for inclusion in this retrospective study. After excluding 32 patients due to incomplete medical records and inadequate follow-up visits (<9 months), 131 eyes from 131 patients were enrolled in this study. Table 1 shows the demographic and clinical characteristics of the patients. Post-traumatic endophthalmitis was more common in male patients (122 of 131 patients: 93.1%). The mean ± SD age of the patients was 40.03 ± 15.39 years (range, 19–86 years). The mechanism of injury was penetrating injury in 68.7% (90 of 131 patients) and IOFB in 31.3% (41 of 131 patients). None of patients experienced globe rupture or a perforating injury. The total number of open-globe injuries during the same time period was 1523 (709 patients with a penetrating injury, 217 patients with an IOFB, 482 patients with a globe rupture and 115 patients with a perforating injury) giving an incidence rate for post-traumatic endophthalmitis of 8.6% (131 of 1523 patients).
Demographic and clinical characteristics of patients (n = 131) diagnosed with post-traumatic endophthalmitis.

Data presented as n of patients (%).
IOFB, intraocular foreign body.
In 36 of 131 patients (27.5%), the findings of post-traumatic endophthalmitis were noted at presentation and in the other 95 of 131 patients (72.5%) the post-traumatic endophthalmitis occurred after hospitalization and during the course of the disease. The maximum time for the development of endophthalmitis was 63 days (mean ± SD, 5.19 ± 2.55 days). The mean ± SD time of presentation to hospital was 40.60 ± 19.32 h (range, 1–168 h). The mean ± SD time to intervention since presentation to hospital (e.g. primary repair and vitrectomy) was 4.96 ± 2.53 h (range, 1–12 h). The mean ± SD admission duration was 4.56 ± 1.56 days (range, 2–11 days).
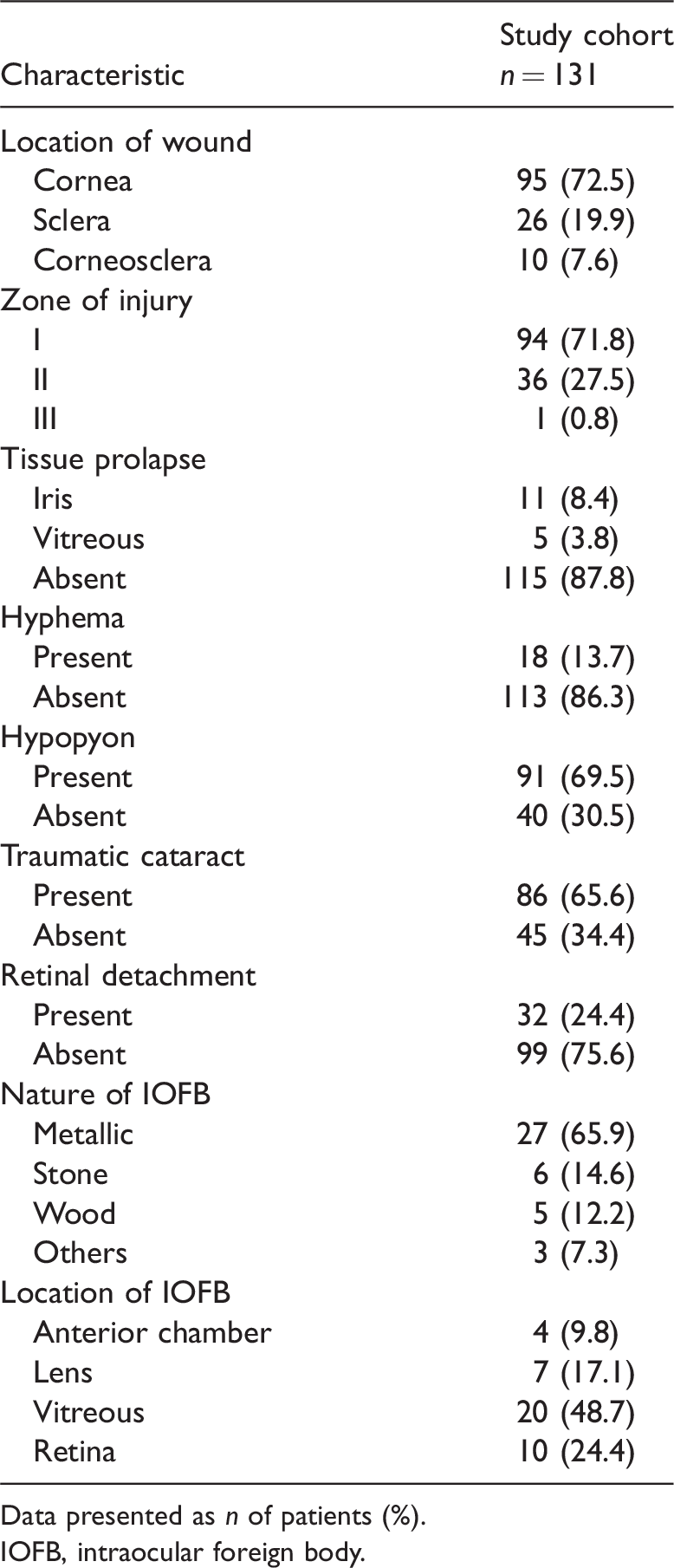
The details of the injuries are presented in Table 2. Corneal, sclera and corneoscleral lacerations were observed in 95 (72.5%), 26 (19.8%) and 10 (7.6%) patients, respectively. Iris or vitreous prolapse, hyphema, hypopyon and traumatic cataract were detected in 16 (12.2%), 18 (13.7%), 91 (69.5%) and 86 (65.6%) of patients, respectively. Among the 86 patients with traumatic cataract, 11 patients had dislocated traumatic cataract and four patients had lens fragment drop. In cases of IOFB, 27 eyes had a metallic foreign body, whereas wood and stone were found in five and six eyes, respectively.
Injury characteristics of patients (n = 131) diagnosed with post-traumatic endophthalmitis.
Data presented as n of patients (%).
IOFB, intraocular foreign body.
The microbiological results and surgical treatment used are shown in Table 3. 96 of 131 (73.3%) smears were negative. The most common reported result of a positive smear was gram positive cocci (16 of 131; 12.2%). Of the cultures, 84 of 131 (64.1%) were negative and 22 of 131 (16.8%) were positive for Staphylococcus species. 121of 131 patients (92.4%) experienced primary repair and 115 of 131 (87.8%) underwent vitrectomy. Silicone oil tamponade was performed for all of patients with concomitant rhegmatogenous retinal detachment (RRD). Among the six patients that underwent penetrating keratoplasty, four eyes had severe corneal melting and two eyes were complicated with significant corneal tissue loss. Only one eye in this current series underwent evisceration.
Microbiological results and the different surgical strategies used in patients (n = 131) diagnosed with post-traumatic endophthalmitis.

Data presented as n of patients (%).
Table 4 demonstrates the association between different factors and final visual outcome. Among the analysed parameters, patients with delayed presentation, IOFB, traumatic cataract, retinal detachment, larger wounds, positive smears and cultures and those with work-related injuries had significantly worse outcomes (P < 0.05 for all comparisons). No significant differences were observed for sex, laterality, nature of the injuring object, location and zone of injury, tissue prolapse, hyphema and hypopyon.
Association between different factors and final visual outcome in patients (n = 131) diagnosed with post-traumatic endophthalmitis.

Data presented as mean ± SD.
IOFB, intraocular foreign body.
NS, no significant between-group difference (P ≥ 0.05); independent samples t-test and analysis of variance were used to compare the groups.
Discussion
The incidence of post-traumatic endophthalmitis was 8.6% in the current study. Previous studies have reported an approximate incidence rate of 2–54%.5–7 This wide range may be associated with heterogeneous sample sizes of different studies. Various mechanisms of trauma may also lead to different incidences of post-traumatic endophthalmitis: 3–30% and 1–61% incidence rates have been reported after penetrating injuries and IOFB, repectively.8–11 This current study showed a 12.7% (90 patients with endophthalmitis out of 709 patients with a penetrating injury) and 18.9% (41 patients with endophthalmitis out of 217 patients with an IOFB) incidence of endophthalmitis after penetrating injury and IOFB, respectively. A higher rate of post-traumatic endophthalmitis in patients with an IOFB compared with a penetrating injury was expected and compatible with previous studies.8–11 None of the patients experienced post-traumatic endophthalmitis following globe rupture or perforating injury in the current study. This finding might have been related to the coverage of the conjunctiva on wounds in globe rupture, which can act as a mechanical barrier preventing the penetration of organisms. Since the majority of perforating injuries are caused by high-velocity projectiles, such as bullets, the thermal property of the object can sterilize the entrance site and decrease the risk of post-traumatic endophthalmitis.
According to a previous report, 12 post-traumatic endophthalmitis is more common in men, which was consistent with the current study. The male:female ratio was 13.6:1 in this current study, showing a significantly higher frequency of post-traumatic endophthalmitis in Iranian men. This result was expected because Iranian men undertake outdoor activities and employment more frequently than women. In this current study, 38.9% of the patients were in the 30–44 year age group.
Several risk factors have been reported for the occurrence of endophthalmitis following open-globe injuries, including the presence of IOFB, delayed primary repair, soil-contaminated injury and positive intraocular culture of a virulent organism. 13 Although primary repair can be delayed for 12–24 h, surgery is recommended as soon as possible to decrease the risk of endophthalmitis. 7 The role of tissue prolapse in developing endophthalmitis is controversial. A previous study suggested that vitreous prolapse was a risk factor for developing acute post-traumatic bacterial endophthalmitis, 10 but another study reported that uveal or vitreous prolapse did not significantly increase the risk of endophthalmitis. 13 This previous study hypothesized that it may be associated with the organism contamination of the conjunctival sac, which is usually less virulent. 13 Hyphema and prolapsed iris tissue are protective factors against endophthalmitis because they block the penetration of microorganisms into the eye. 14
Previous research has demonstrated positive cultures in 17–81% of cases of post-traumatic endophthalmitis.15–17 The source of pathogens can be either exogenous pertaining to the injuring object or the patient’s own ocular normal flora, which is associated with a better prognosis. 13 Bacteria are responsible for approximately 80–90% of culture-positive cases. 1 A positive culture was seen in 35.9% of the patients in the current study. Similar to previous studies that described gram-positive organisms such as Bacillus, Staphylococci and Streptococci as the most common pathogens of post-traumatic endophthalmitis,18–21the current study found Staphylococcus species to be the most common organisms. Moreover, fungal microorganisms are responsible for 4–14% of post-traumatic endophthalmitis, of which Candida, Aspergillus and Fusarium are the most common. 22 However, none of our cases developed fungal endophthalmitis, which is similar to a previous report. 23 According to some studies, up to one-third of the traumatized eyes may show a positive bacterial culture of intraocular fluids not leading to endophthalmitis.24,25 Thus, a positive intraocular culture does not always mean endophthalmitis and compatibility with clinical findings is necessary.
A diagnosis of post-traumatic endophthalmitis is challenging due to occasional nonspecific manifestations and must be differentiated from acute inflammatory reactions. Photophobia, tearing, increased ocular pain out of proportion to the degree of injury, developing hypopyon, fibrin reaction, vitritis and retinitis can guide physicians toward the diagnosis of post-traumatic endophthalmitis. Notably, endophthalmitis induced by Bacillus has a hyperacute course and may lead to panophthalmia within 24 h, whereas fungal endophthalmitis demonstrates a subacute behaviour. 1 Previous research demonstrated that Bacillus is an extremely poor prognostic factor that can lead to the vision of NLP. 1
The visual outcome of post-traumatic endophthalmitis is worse than postoperative patients.1,2 This finding can be attributed to more virulent pathogens and concomitant ocular damage. 26 In the current study, delayed presentation, IOFB, traumatic cataract, retinal detachments, larger wounds (≥4 mm), positive smears and cultures and work-related injuries were poor prognostic factors. In contrast, sex, laterality, the nature of the injuring object, location and zone of injury, tissue prolapse, hyphema and hypopyon did not show statistical associations with the final outcome.
Although prophylactic antibiotics provided via different routes of administration, including systemic, subconjunctival and topical, are routinely used for most open-globe injuries, there is no strong evidence or definitive guidelines for the method of prophylaxis. 7 Fluoroquinolones are the most commonly used antibiotics for prophylaxis. 12 Intravenous vancomycin and ceftazidime may be helpful in high-risk cases.27,28 Additionally, hourly instillation of fortified topical vancomycin and ceftazidime drops can boost the effect of antibiotic therapy. 28 Routine administration of prophylactic intravitreal antibiotics is not universally accepted due to the risk of retinal toxicity and complications associated with injection, especially in the presence of choroidal or retinal detachment. 7 However, there are reports that intravitreal antibiotic injection reduces the risk of endophthalmitis. 10 Especially in eyes with a soil-contaminated intraocular foreign body, the injection of intravitreal vancomycin and ceftazidime or amikacin is recommended. 29 In suspected fungal endophthalmitis, the systemic administration of fluconazole or voriconazole and intravitreal injection of amphotericin B or voriconazole should be considered. 28
In contrast to the Endophthalmitis Vitrectomy Study designed for postoperative endophthalmitis, no standard and well-defined treatment protocol is available for traumatized eyes. 1 Pars plana vitrectomy is required in approximately 90% of eyes with endophthalmitis secondary to open-globe injuries. 1 Some researchers advised vitrectomy for treatment of all cases of post-traumatic endophthalmitis and even as a prophylaxis in clinically suspected cases.7,30,31 Removing the source of infection, decreasing inflammation and a better effect of antibiotics are the theoretical advantages of this method. Nevertheless, its surgical risks and financial costs are also considerable. 7
The visual outcome of post-traumatic endophthalmitis is unfavourable.1,2 Determining the direct influence of endophthalmitis on visual prognosis is extremely difficult because the traumatized eyes are accompanied by other conditions such as tissue damage, lens disruption and retinal detachment. 26 A final visual acuity of ≥20/400 was reported in 9–50% of patients with post-traumatic endophthalmitis in previous studies.2,8,19 The anatomical success rate or, in other words, saving the globe was excellent in the current study since only one patient underwent evisceration, which was thought to be associated with the aggressive and immediate intervention undertaken in this current series.
In conclusion, post-traumatic endophthalmitis is a devastating complication following open-globe injuries. The majority of damage occurs in work-related places. Immediate presentation to ophthalmic centres and timely diagnosis and intervention may lead to better outcomes. In this current series, patients with delayed presentation, IOFB, traumatic cataract, retinal detachment, larger wounds (≥4 mm), positive smears and cultures and work-related injuries had poorer outcomes.