
Abstract
Germ cell tumors (GCTs) often occur in male testes and female ovaries. Extragonadal GCTs account for approximately 2% to 5% of all GCTs and mainly occur in the mediastinum, retroperitoneum, and pineal gland. In this study, we reported a rare case of gastric adenocarcinoma with GCT components. The patient’s serum α-fetoprotein (AFP) level was higher than normal. Abdominal computed tomography (CT) showed a 10-cm × 10-cm tumor between the spleen and the bottom of the stomach. Gastric endoscopy indicated an ulcerative lesion extending from the bottom of the stomach to the antrum. Tissue biopsy identified the tumor as an adenocarcinoma. The patient underwent abdominal tumor resection, subtotal gastrectomy, D2 lymphadenectomy, and splenectomy. Postoperative histopathology showed that the tumor was a moderately to poorly differentiated adenocarcinoma. Immunohistochemistry analysis revealed positive staining for AFP, glypican-3, and placental alkaline phosphatase. Gastric adenocarcinoma with GCT components is particularly uncommon and rarely reported. Elevated serum AFP and/or β-human chorionic gonadotropin levels, abdominal CT, histopathology, and immunohistochemistry may help diagnose GCTs. Radical surgery resection is the primary treatment method for GCTs. Adjuvant chemotherapy and radiotherapy are effective for advanced GCTs.
Keywords
Background
Germ cell tumors (GCTs) occur more often in male testes and female ovaries. 1 Extragonadal GCTs (EGGCTs) account for approximately 2% to 5% of all GCTs and mainly occur in midline locations, such as the mediastinum, retroperitoneum, and pineal gland. 2 Although EGGCTs develop anywhere in the body, 50% to 70% of cases are found in the mediastinum.1,3 Malignant gastric GCT is particularly rare and hardly reported. Although the serological and histological characteristics of EGGCTs are similar to those of GCTs, their biological behavior and clinical prognosis are different. 4 In this study, we reported an extremely rare case of gastric adenocarcinoma with GCT components and summarized the characteristics, diagnosis, treatment methods, and prognosis of EGGCTs.
Case presentation
This study was approved by the Ethics Committee and Institutional Review Board of the Second Hospital of Jilin University, Changchun, China. The patient provided written informed consent for publication of this case report and any accompanying images. The reporting of this study conforms to CARE guidelines. 5
A 67-year-old man came to our department because of an abdominal tumor found during a regular medical examination. The patient had no history of gastrointestinal diseases or any other abdominal symptoms. The patient denied any history of hypertension, heart diseases, diabetes, or drugs and food allergies. The physical abdominal examination showed a 5-cm × 5-cm mass with good mobility. The physical testicular examination did not reveal any positive findings. The patient’s carcinoembryonic antigen (normal: 0–3 ng/mL) and α-fetoprotein (AFP, normal: 0–20 ng/mL) levels were 2.21 ng/mL and 64.42 ng/mL, respectively. Other biochemical parameters, including hemoglobin, alkaline phosphatase, and β-human chorionic gonadotropin (β-HCG), were all normal. Abdominal computed tomography (CT) showed a 10-cm × 10-cm tumor between the spleen and the bottom of the stomach. The tumor compressed the surrounding intestines and the lower part of the spleen (Figure 1). CT of the thorax did not reveal mediastinal or lung tumors. Gastric endoscopy showed an ulcerative lesion extending from the bottom of the stomach to the antrum. Tissue biopsy identified the tumor as an adenocarcinoma. No tumors were found in the liver, pelvis, or small intestines during the laparotomy, and no metastatic nodules were found in the peritoneum, omentum, and mesentery roots. A 10-cm × 8-cm × 6-cm tumor was found between the stomach and spleen. With good mobility, the tumor grew close to the stomach and partially invaded the spleen. Abdominal tumor resection, subtotal gastrectomy, D2 lymphadenectomy, and splenectomy were performed. The resected tumor was oval with several vascular branches (Figure 2).

Abdominal CT examination showing a 10-cm × 10-cm tumor between the spleen and the bottom of the stomach.

The resected tumor and spleen.
The patient recovered without complications. Postoperative histopathology showed that the tumor was a moderately to poorly differentiated adenocarcinoma (Figure 3). The tumor penetrated the stomach wall and the spleen capsule and invaded the omentum. The surgical margins were negative, and the number of harvested lymph nodes was 23, including three positive lymph nodes. The final stage of this tumor was confirmed as IIIC. Immunohistochemistry revealed positive staining for AFP, glypican-3, and placental alkaline phosphatase (PLAP), as shown in Figure 4. These findings supported the diagnosis of gastric adenocarcinoma with GCT components. Doppler ultrasound examination of the bilateral testicle did not indicate any abnormalities. In addition, we did not find any microliths in the testis. The patient did not receive post-surgical treatment. The follow-up time was 1 year, and no tumor recurrence or distant metastasis was found.

Histopathology showing the oval tumor cells with clear nucleoli, small cell volume, and abundant cytoplasm (magnification, ×40), Scale bar = 100 µm.
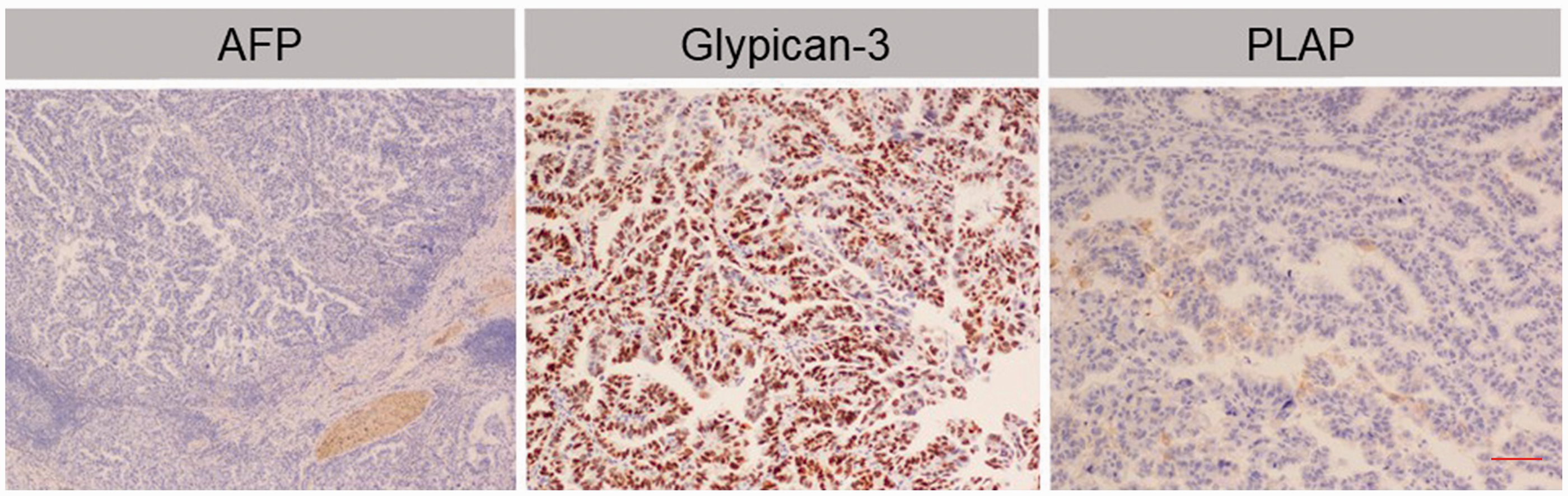
Immunohistochemistry staining of AFP, glypican-3, and PLAP (magnification, ×200).
Discussion
EGGCTs are particularly rare, accounting for 1% to 4% of all GCTs.6,7 Among EGGCTs, gastric adenocarcinoma with GCT components is extremely rare and hardly reported. GCTs are classified into seminoma and nonseminomatous types based on pathological features. Nonseminomatous GCTs are further classified into embryonic carcinoma, teratoma, choriocarcinoma, endodermal sinus tumor, and mixed GCTs. 7 EGGCTs are either benign or malignant, and the progression of malignant EGGCTs is rapid. Patients with EGGCTs can be asymptomatic in the early stage. 8 The symptoms of EGGCTs vary depending on the site and size of the tumors. It is important to distinguish between burned-out tumors of the testis and EGGCTs. A burned-out tumor refers to the presence of a metastatic GCT with histological regression of the primary testicular tumor. 9 Microliths identified by ultrasound in the testis are associated signs of burn-out tumors. The patient in our study was asymptomatic, and the abdominal mass was found during routine health examination. Post-surgical pathology confirmed that the tumor was a moderately to poorly differentiated adenocarcinoma with GCT components. As a result, the patient was diagnosed with gastric adenocarcinoma with GCT components, not pure gastric GCT.
AFP and β-HCG are typical tumor markers of GCTs. These markers provide diagnostic and prognostic information on the tumors. Only a few patients with seminomatous GCTs show elevated β-HCG levels. However, the degree of β-HCG elevation in patients with seminomatous GCTs is usually lower than that in patients with nonseminomatous GCTs. 10 The AFP levels in patients with seminomatous GCTs are typically within the normal range. If the β-HCG is higher than 100 ng/mL or the AFP is higher than normal, the tumor may contain nonseminomatous components. 10 In this case, the AFP was higher than normal, but the β-HCG was normal. Aspiration biopsy may support the clinical diagnosis, but pathological examination is still the standard diagnostic method for EGGCTs. Immunohistochemistry examination is vital for the differential diagnosis of EGGCTs, and positive staining for AFP, glypican-3, PLAP, and CD30 is common in GCTs cases.11,12 In addition, p53 may be involved in the early development of GCTs and is a sensitive marker for some types of GCTs. 13 However, different types of GCTs have various p53 gene mutations. 14 In this study, the tumor tissues showed positive staining for AFP, glypican-3, and PLAP, but p53 was not highly expressed in the tissues of gastric adenocarcinoma with GCT components. The type of GCT might be yolk sac. Glypican-3 is strongly and diffusely expressed in yolk sac tumors but negatively or weakly expressed in other types of GCTs. 15 Furthermore, positive AFP expression supports the diagnosis of a yolk sac tumor. 15 miRNA is expected to provide a stable, accurate, and specific marker of GCTs. 16 It was previously reported that the diagnostic accuracy of AFP and β-HCG for GCTs was over 60%. Combined with the detection of miRNA in serum, the diagnostic accuracy for GCTs increased to 98%. 17
Radical surgery is still the primary treatment for GCTs. For advanced GCTs, cisplatin-based chemotherapy may improve the survival time and cure rate of patients. 18 For recurrent or cisplatin-resistant GCTs, gemcitabine combined with oxaliplatin chemotherapy is considered an effective treatment approach.19,20 Radiotherapy is a comprehensive treatment method for patients with residual tumors after chemotherapy who refuse surgery or have contraindications to surgery. 21 However, nonseminomatous GCTs are less sensitive to radiotherapy. Regular examination of serum AFP and abdominal CT after surgery may help predict tumor progression, recurrence, or metastasis.
In this article, an extremely rare case of gastric adenocarcinoma with GCT components was reported. The tumor penetrated an entire layer of the stomach wall and invaded the spleen nearby. Post-surgical histopathology and immunohistochemistry revealed a gastric adenocarcinoma with EGGCT features.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211069202 - Supplemental material for Gastric adenocarcinoma with germ cell tumor components: a rare case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605211069202 for Gastric adenocarcinoma with germ cell tumor components: a rare case report by Xu Han, Shu Wang, Hongyu He, Yao Sun and Jiannan Li in Journal of International Medical Research
Footnotes
Author contributions
XH and SW wrote the first version of the article. XH, SW, HYH, YS, and JNL participated in the conception and design of the study and drafted the article. JNL supervised the study and reviewed the article critically for intellectual content. All authors reviewed and approved the final version of the article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Department of Finance of Jilin Province (#3D5197434429), Department of Education of Jilin Province (#2021LC019), Youth Program of the National Natural Science Foundation of China (#3A4205367429), and Education Project of Jilin University (#419070600046).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.