
Abstract
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is a congenital disorder characterized by congenital absence of both the uterus and vagina. Some patients require surgery to create a neovagina, however, the preservation of a nonfunctional rudimentary uterus after surgery may lead to long-term complications. Herein, a rare case of a giant hysteromyoma after vaginoplasty, in a 31-year-old Chinese female patient who was diagnosed with MRKH syndrome, is reported. The patient, who had undergone vaginal reconstruction 4 years previously, presented with abdominal distension for the previous 2 weeks. Transabdominal ultrasonography showed a firm mass of approximately 10 × 10 cm in the lower abdomen. The patient subsequently underwent an exploratory laparotomy, and a leiomyoma from her rudimentary uterus was removed. Beside this case, seven cases, published between 2004 and 2020, were identified during a literature search. Findings of the present and previously published cases suggest that gynaecologists should pay particular attention to the risks of pelvic complications in female patients with MRKH syndrome who have previously undergone surgery, and select appropriate therapeutic methods.
Keywords
Introduction
Congenital absence of both the uterus and vagina is termed Müllerian aplasia, or Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome, and affects at least 1 in 5000 females.1,2 Although rare, it is the second most common cause of primary amenorrhea, after gonadal dysgenesis. 3 MRKH syndrome is a class 1 Müllerian duct anomaly and can be divided into two types: type I (56–72% of cases), characterized by symmetric muscular buds and normal fallopian tubes; and type II (28–44% of cases), characterised by asymmetric muscular buds, abnormal fallopian tubes, and other congenital anomalies. 4 Approaches used to create a functional vagina include surgical vaginoplasty and non-surgical dilation therapy, and although it remains unclear which treatment is best, surgical vaginoplasty is considered to be an effective solution. 5 Complications after surgical or invasive procedures may be inevitable, 6 however, and mainly include dyspareunia, urinary duct obstruction, vaginal duct stenosis and infection. In some cases, the uterine remnants in patients with MRKH syndrome may also lead to unexpected complications, including fibroids, adenomyosis and pelvic pain.7,8 Here, a rare clinical case of leiomyoma after vaginoplasty in a female patient with MRKH syndrome is described. Additionally, the authors emphasize the necessity of intraoperative exploration and evaluation of the nonfunctional rudimentary uterus during vaginoplasty in women with MRKH syndrome, unless only bowel vaginoplasties are implemented in an external approach.
Case report
Ethical approval was obtained from the Ethics Committee of the Shandong Provincial Hospital, Jinan, China, in accordance with the ethical guidelines of the 1975 Declaration of Helsinki (as revised in 2013). Written informed consent was obtained from the patient for publication of this manuscript and any accompanying images, and the reporting of this case conforms to CARE guidelines. 9
A 31-year-old married female patient was admitted to the gynaecology ward of Shandong Provincial Hospital in March 2018, due to abdominal distension for the previous 2 weeks. There was no significant history of cyclical vaginal bleeding, or of urinary or bowel complaints. The patient had sought medical advice at Shandong Provincial Hospital 4 years previously due to amenorrhea and infertility. Further examination at that time showed an aplastic vagina and uterus. She was phenotypically female and had normal secondary sexual characteristics: well-developed breasts (Tanner stage 5) and female external genitalia. The clitoris and labia majora appeared normal. However, her labia minora showed local depigmentation. Her pubic hair showed female-type distribution. Chromosome analysis revealed a normal female karyotype (46, XX), and an endocrine evaluation showed an intact hypothalamic-pituitary-ovarian axis. She had no known allergies, and did not smoke, drink alcohol, or use illicit substances. Her family medical history was unknown. Abdominal ultrasonography revealed a complete urinary system with normal morphology. She was then diagnosed with MRKH syndrome (type I) and received a bowel vaginoplasty at Shandong Provincial Hospital in 2014.
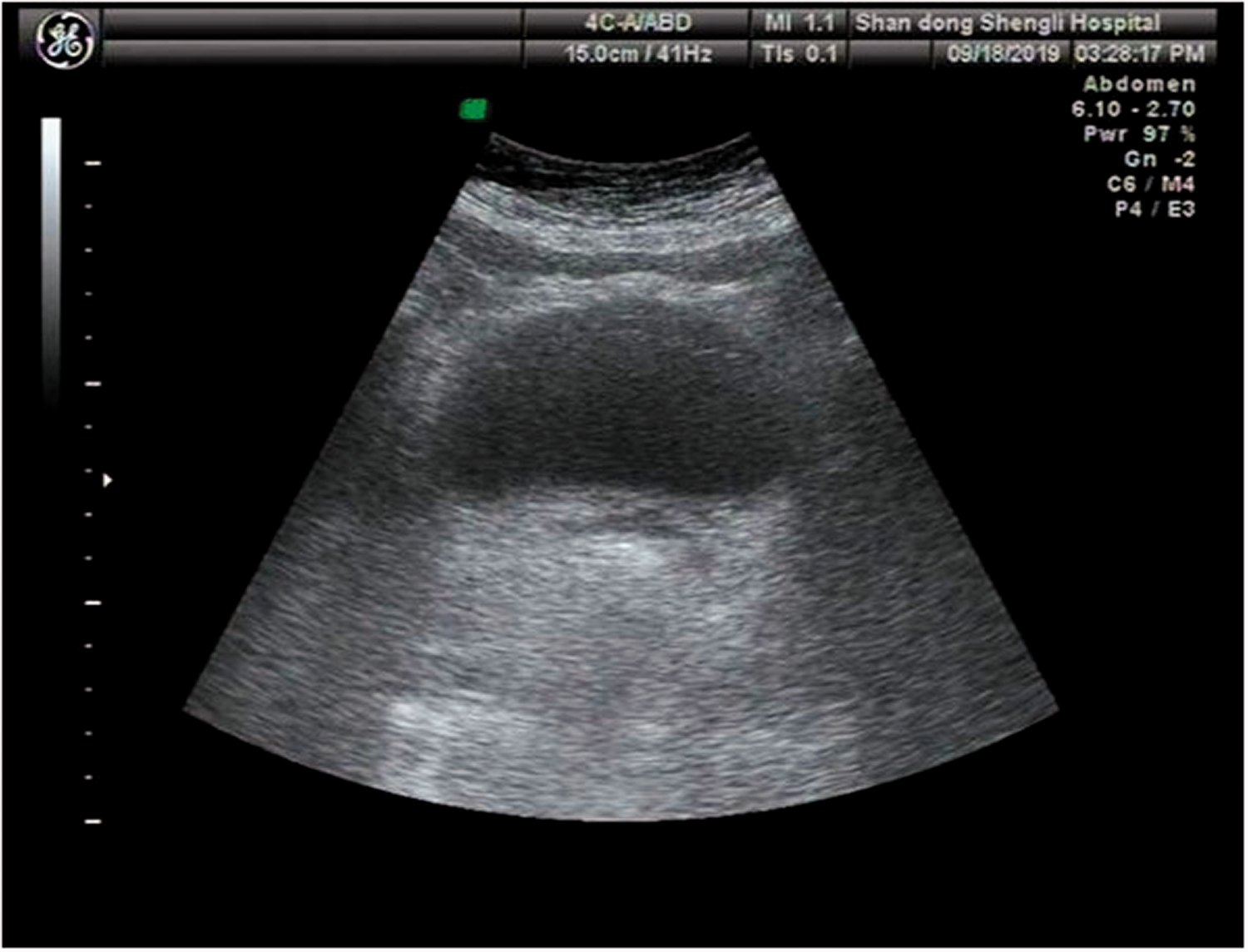
A speculum examination during a routine outpatient follow-up appointment, less than 1 month prior to admission, revealed a blind vaginal pouch 7-cm deep and the absence of the cervix. On bimanual examination, an irregular, firm, 10-cm mobile mass arising from the pelvis was palpable. Transabdominal ultrasonography revealed a well-defined hypoechoic mass in the pelvis with a heterogeneous echo inside, measuring 10.8 × 9.6 cm. The inferior border of the mass reached a cervix-like structure (Figure 1). After consultation, the patient was primarily diagnosed with hysteromyoma. The patient then underwent a laparotomy, and during surgery, a large pelvic mass with an intact capsule was seen arising from the right rudimentary uterus (Figure 2). The mass was enucleated after opening the thin cyst wall, and the excised mass was revealed to have the appearance of a whorled white-coloured muscle-like tissue (Figure 3). The pathological diagnosis was leiomyoma (Figure 4), based on the presence of smooth muscle cells showing a long fusiform parallel arrangement with complete capsule microscopically. During the surgical exploration, an asymmetric fusiform uterus was found in the pelvic peritoneum. The rudimentary uterus was normal in size, and was connected to structured ovaries via 5 cm-long fallopian tubes. The operation was ultimately successful, and the pelvic mass, bilateral rudimentary uterus and fallopian tubes were removed.

Transabdominal ultrasonography image from a 31-year-old Chinese female patient with Mayer-Rokitansky-Küster-Hauser syndrome, showing a hypoechoic mass in the pelvis, measuring 10.8 × 9.6 cm.

Representative image of the surgical exploration showing a large pelvic mass with an intact capsule arising from the right rudimentary uterus of a 31-year-old Chinese female patient with Mayer-Rokitansky-Küster-Hauser syndrome.

Representative image of the excised mass from a 31-year-old Chinese female patient with Mayer-Rokitansky-Küster-Hauser syndrome, with thin cyst wall removed showing white muscle-like tissue with a whorled appearance.
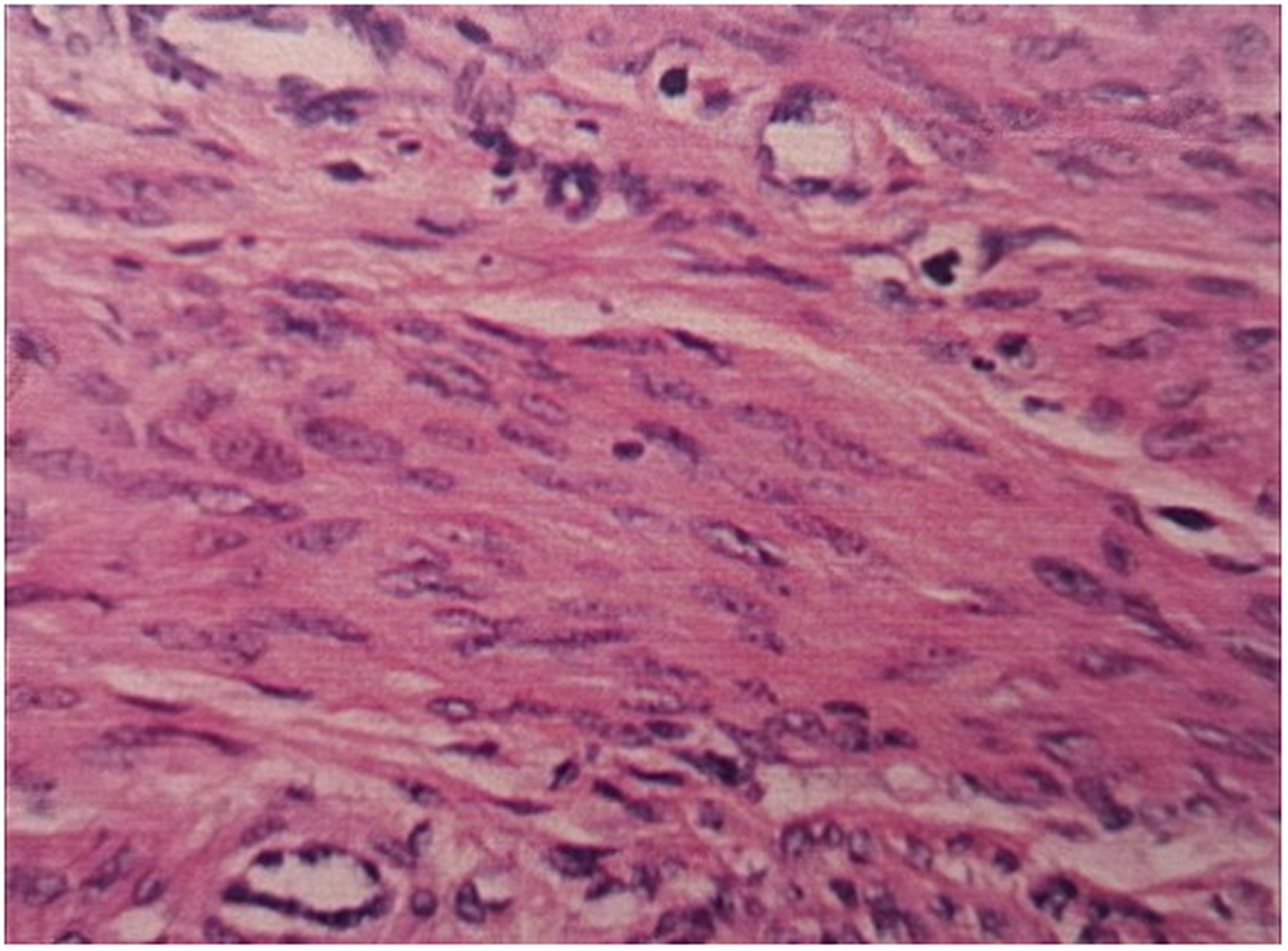
Representative histopathology image of a haematoxylin and eosin-stained pelvic mass section from a 31-year-old Chinese female patient with Mayer-Rokitansky-Küster-Hauser syndrome, showing smooth muscle cells show a long fusiform parallel arrangement with complete capsule microscopically (original magnification, ×400).
The patient recovered and was discharged without incident. No sign of recurrence was found at the 1-year postoperative check-up (Figure 5), and the patient was free from lower abdominal symptoms.
Transabdominal ultrasonography image from a Chinese female patient with Mayer-Rokitansky-Küster-Hauser syndrome, at a 1-year postoperative follow-up assessment after surgery to remove a large pelvic mass.
Discussion
Herein, the case of a large leiomyoma raised from the rudimentary uterus in a female patient with MRKH syndrome is reported. The special feature of this patient was that she had previously undergone bowel vaginoplasty and retained the rudimentary uterus where the leiomyoma had formed. Thus, the remaining rudimentary uterus had led to complications several years later that finally resulted in this patient having to undergo a second operation. A comprehensive search of PubMed and Web of Science databases, using phrases such as ‘Mayer-Rokitansky-Küster-Hauser’, ‘MRKH’, and ‘vaginoplasty’, either alone or in combination, revealed that reports of leiomyomas in female patients with MRKH syndrome who had received vaginoplasty are not unique. Published studies show that leiomyomas may occur in the nonfunctional rudimentary uteri of female patients with MRKH syndrome, even if they had undergone an exploration during vaginoplasty,10–13 while there are few reports of hysteromyoma growing as fast as the present case in such a short time after surgery. Thus, the present authors suspect that they had failed to detect the growing hysteromyoma in an initial examination.
The best treatment for vaginal agenesis in MRKH syndrome currently remains unclear, however, it has been reported that non-surgical methods, mainly vaginal dilatation techniques, should be considered a first-line option before any surgical intervention. 14 Once the dilation fails or is inappropriate due to previous scarring or an absent vaginal dimple, surgical vaginoplasty may be considered. Surgical reconstruction methods include surgical creation of a neovaginal space between the bladder and rectum, bowel vaginoplasty, vulvaginoplasty and surgical traction.15,16 However, there are no guidelines on whether the rudimentary uteri should be saved during surgery. Published reports regarding the course of patients with MRKH syndrome, whose rudimentary uteri were preserved during vaginoplasty, are summarised in Table 1.17–22
Summary of present and published cases of patients with MRKH syndrome whose rudimentary uterus was preserved during vaginoplasty.

CT, computed tomography; MRI, magnetic resonance imaging; MRKH, Mayer-Rokitansky-Küster-Hauser; USG, ultrasonography; UN, unknown; NA, not available.
In the present literature review, the Abbe-McIndoe operation was one of the most commonly used methods of vaginal reconstruction (performed in two cases).17,18 Williams' vaginoplasty was performed in three cases,19,20 Vecchietti’s vaginoplasty in one case, 21 and Davidov’s vaginoplasty in one case. 22 Oestrogen levels were normal in almost all cases,17,19–21 except in one peri-menopausal patient, and cyclic endometrial changes were found by ultrasound in some patients’ rudimentary uteri before they received vaginoplasty.17,21 These patients preserved their uterus either because the vaginoplasty was performed via an external approach, or no abnormality was found during surgical exploration until hysteromyoma was detected by postoperative imaging examination or new symptoms appeared. Inconspicuous symptoms, such as mild abdominal pain and abdominal distension were reported in most cases, however, emergency abdominal surgery may also result, due to acute torsion of the uterine remnant leiomyoma. 21 Laparotomy was the most commonly reported surgery in the present literature review, especially in cases of giant uterine leiomyoma with the complicated nature of its feeding arteries,18,20 and in emergency abdominal surgery. 21 All patients underwent hysterectomies.
Some patients with MRKH syndrome have small rudimentary Müllerian bulbs that result from abnormal development of the Müllerian duct during embryogenesis. Oppelt et al., 23 reported that 82% (239/290) of patients have uterine remnants, including bilateral rudimentary remnants and a plastic uterine horn. Most of the uterine remnants or small rudimentary Müllerian bulbs lack endometrial activity, and the rudimentary uteri are usually composed of smooth muscle cells, which may lead to leiomyomas. Around 2–7% of patients with MRKH syndrome have a functional endometrium in the rudimentary uteri, 5 and the presence of endometrium in rudimentary uteri may lead to pelvic pain. Of 48 females with MRKH syndrome, 48% (23) were found to have uterine remnants, and 46% (22) reported pelvic pain. 24 The presence of endometrium was also found to be associated with pelvic pain (risk ratio 2.3; 95% confidence interval 1.2, 4.7) in females with MRKH syndrome. 24 Moreover, in some patients with a functional rudimentary uterus, pregnancy may be achieved by uterine and cervical reconstruction, creation of a neovagina and placement of a uterovaginal conduit or zygote intrafallopian transfer.25,26 However, the present review of the literature failed to uncover a case report of successful delivery from female patients with rudimentary uteri, and there are certain risks of uterine rupture during pregnancy among such cases, that may lead to catastrophic results, with a death rate of 47.6% reported at the beginning of the 20th century. 27 Considering the risk of pregnancy and complications of surgical therapy, preserving the rudimentary uteri in patients with MRKH syndrome during vaginoplasty makes little sense.
In conclusion, because of the high incidence of uterine remnants in female patients with MRKH syndrome, the risk of complications after vaginoplasty in these patients may be higher than preconceived. Females with MRKH syndrome should receive an anatomic evaluation with transabdominal ultrasonography and magnetic resonance imaging before receiving surgery, such as vaginoplasty or laparoscopic diagnosis. Once a diagnosis of MRKH syndrome with a rudimentary uterus is clarified, gynaecologists should perform a detailed examination to detect whether a hysteromyoma has occurred, or inform patients of the risk of leiomyomas and cyclic pelvic pain. Total resection of the uterine remnants should be considered if endometrial activity or hysteromyoma in the rudimentary uterus is found.
Footnotes
Acknowledgements
Written informed consent was obtained from the patient for publication of this report. The research was supported by grants from the National Natural Science Foundation of China (No. 81671434).
Author Contributions
Shikang Qiu designed, performed the study, and wrote the manuscript. Feiwang and Yonghui Zou performed the surgery together. Shikang Qiu, Yunkai Xie performed the pathologic analysis and searched all the cases and made the analysis. All authors read and approved the manuscript for publication.
Data accessibility
Data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This research was supported by a grant from the National Natural Science Foundation of China (No. 81671434).