
Abstract
The Mayer-Rokitansky-Küster-Hauser syndrome is the congenital absence or underdevelopment of the uterus and vagina even though the external genitalia, ovaries and ovarian function are normal. This condition is uncommon in Cameroon. A 23-year-old woman of the Fulbé tribe, a predominantly Islamic tribe of the northern part of Cameroon, complained of the absence of menstruation after age of puberty and lower abdominal pain occurring almost at the same period every month. She has been married polygamously for 10 years and has been having normal, satisfactory sexual intercourse. The sonographic and laparoscopic findings of this patient were consistent with Mayer-Rokitansky-Küster-Hauser syndrome. The patient was counseled for in vitro fertilization and surrogacy. Patients with Mayer-Rokitansky-Küster-Hauser syndrome typically present with primary amenorrhea during adolescence. With the existing medical technology in Cameroon, this condition is easily accessible in tertiary healthcare facilities. Patients with Mayer-Rokitansky-Küster-Hauser syndrome could become mothers through in vitro fertilization and surrogacy, but the cost is prohibitive in Cameroon.
Keywords
Background
The Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome is the congenital absence or underdevelopment of the uterus and vagina. The external genitalia, ovaries and ovarian function are normal. The prevalence of MRKH syndrome has been reported to be 1 in 5000 live female births in Caucasians. 1 The prevalence in Cameroon remains unknown. The etiology of MRKH syndrome remains unknown; however, reports on familial clustering of MRKH syndrome and its associated anomalies suggest a genetic component. 2
The MRKH syndrome has since its discovery been widely described as a defect of the development of the paramesonephric (Mullerian) system characterized by the absence or underdevelopment of the uterus and vagina, sometimes associated with anomalities of the kidneys. The patients have a normal female phenotype (outward appearance) and karyotype 46XX. 3 The two main challenges faced by patients with MRKH syndrome include how to achieve adequate or satisfactory sexual intercourse and procreation. Some of these patients have benefited from vaginal reconstructive surgery,4,5 while others have been able to become mothers through surrogacy. 6 However, in the future, women with MRKH syndrome could benefit from uterine transplant. 7 That notwithstanding, these new approaches are still not accessible to many couples in Cameroon and most low-income countries. 8 We are presenting the case of MRKH syndrome that was managed at the Department of Obstetrics and Gynecology in a low-resource tertiary hospital in Douala, Cameroon.
Case presentation
A 23-year-old woman of the Fulbé tribe, a mainly Islamic tribe of the northern region of Cameroon, came to our obstetrics and gynecology unit with a complaint of primary amenorrhea, a 5-day monthly (rhythmic) lower abdominal pain (corresponding to a probable ovulation or intra-abdominal menstruation from an active endometrium or endometriosis following intra-abdominal cryptomenorrhea). She has been married for 10 years polygamously (husband has four children with the other wife) and has been having normal, satisfactory sexual intercourse. She has no formal education and denies any breast discharge. Her breast and pubic hair distribution were normal, and there was no acne or hirsutism. The patient had mid lower abdominal pain on palpation. The vulva was normal and the vaginal length from introitus to the blind ending of the vagina was about 68 mm; the width was about 28 mm and allowed free passage of the speculum. The cervix and uterus were absent. Her body mass index (BMI) was 21 kg/m2.
Her early follicular hormonal profile (calculated from about 10 days after the monthly lower abdominal pain) was as follows: estradiol = 205 pmol/L, follicle-stimulating hormone (FSH) = 3.97 mIU/L, luteinizing hormone (LH) = 4.53 mIU/L, prolactin level = 276 pmol/L, testosterone = 0.75 µg/L, DHEAS (dehydroepiandrosterone sulfate) = 5.4 µmol/L and her Karyotype was 46XX. She is HIV and HBsAg negative.
The patient underwent trans-abdominal ultrasound scanning that showed absent uterus and two normal size ovaries (Figure 1). The kidneys, pancreas, bile ducts and liver are normal. At laparoscopy, she was found to have normal left fallopian tube with a uterine horn remnant that prolonged to the hypoplastic right mullerian duct that ended up in a normal right fallopian tube. Both ovaries were macroscopically normal and contained ovarian follicles on the cortex with a corpus luteum on the right ovary (Figures 2 and 3). The liver, gallbladder and stomach were normal. We are counseling this couple for in vitro fertilization (IVF) and surrogacy and for receiving nomégestrol acétate (Lutenyl™) 5 mg daily for the last 10 days of each month.

Sonographic image of the internal genital organs. The ovaries are present with cortical follicles.

Laparoscopic view of the pelvis in a patient with Mayer-Rokitansky-Küster-Hauser syndrome with the presence of cornual muscular bud (left side).
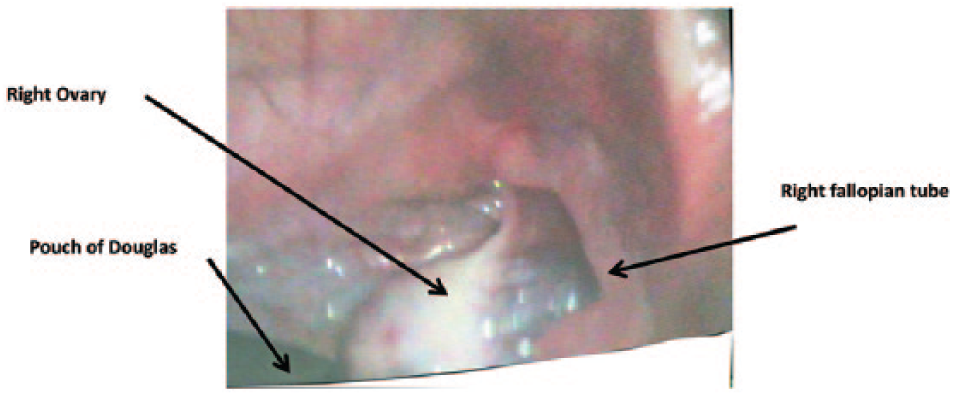
Laparoscopic view of the pelvis in a patient with Mayer-Rokitansky-Küster-Hauser syndrome with the absence of muscular bud (right side).
Discussion
Patients with MRKH syndrome typically present with primary amenorrhea during adolescence. Women with this condition have normal ovarian function and become mothers through IVF-ET and surrogacy in high-income countries. These procedures are usually too costly for Cameroonian couples; besides, most cultures reject IVF babies as abnormal. 8 The prevalence of MRKH syndrome has been reported to be 1 in 5000 live female births in Caucasians. 1 Furthermore, the etiology of MRKH syndrome remains unknown; however, reports on familial clustering of MRKH syndrome and its associated anomalies suggest a genetic component. 2 However, we did not find any familial history of MRKH syndrome in the index case.
The index case has a vaginal length of 68 mm and has been having satisfactory sexual activity. This is very unusual for a patient with MRKH syndrome who is not receiving any form of treatment because most patients with MRKH syndrome have a vaginal length of about 1–3 cm at diagnosis. However, coital (by intercourse) dilation prior to our examination may be the reason for the vaginal depth of the patient. 9 Coital dilation has recently been reported to provide promising anatomical results compared with surgery and self-dilation. 10 This non-medical (coital dilation) treatment is not widely known in Cameroon.
Therefore, it is a technique worth vulgarizing in low-income countries because it needs no special expertise to carry out the procedure as compared with primary vaginal dilation.3,11
Based on laparoscopy and MRI (magnetic resonance imaging), patients with MRKH syndrome have been classified into two groups: type 1 (isolated) including all patients with no associated abnormalities and type 2 (syndromic) considered all patients with extragenital abnormalities (this type also includes patients with MURCS (Mullerian duct aplasia–renal agenesis–cervicothoracic somite dysplasia) association). According to this classification, the index case is type 1 (isolated uterovaginal agenesis).12,13
In cases like the index case, oocyte retrieval by transvaginal sonography will be easily accessible because the ovaries are low-lying in both fossae ovarica. 14 Others have reported cases where only laparoscopic 14 or trans-abdominal 6 oocyte retrieval was possible and where ovaries were in an ectopic position.
This couple lives in the northern region of Cameroon where health facilities are rare and rudimentary. To add to this, they are of the Islamic faith and polygamous. These factors made appropriate medical attention difficult and proper diagnosis still more so. For its part, the pressure of childbirth, which could have prompted a more urgent quest for medical attention, was removed since the husband had children with the other wife.
Islamic religion accepts IVF and surrogacy provided the gametes are from both husband and wife (not donor gametes). 15 The index case had monthly (rhythmic) lower abdominal pain, indicating that she had been ovulating regularly because we did not find any endometriotic lesions at laparoscopy, but there was a corpus luteum on the right ovary. She is presently receiving nomégestrol acétate (Lutenyl™). This has been reported by others. 16
The medico-legal and ethical issues related to assisted reproductive technology (ART) and surrogacy including problems of genetic inheritance of offspring of women with MRKH syndrome are problems we have to deal with in the counseling of this patient because there is a lack of knowledge of these procedures in Cameroon. Furthermore, ART and surrogacy are not acceptable in most cultures in Cameroon. There is also no legislation regulating the practice of ART in Cameroon. We usually rely on recommendations from high-income countries. 8
In recent years, there are reports of uterine transplantation in some high-income countries. 7 This could be a future treatment modality that will be easily accepted in Cameroon.
Conclusion
Patients with MRKH syndrome typically present with primary amenorrhea during adolescence. With the existing medical technology in Cameroon, this condition is easily accessible in tertiary healthcare facilities. Patients with MRKH syndrome could become mothers through IVF and surrogacy, but the cost is high and prohibitive in Cameroon.
Footnotes
Acknowledgements
The authors thank staff of the Radiology Department, operating theater and the doctors and nurses of the Douala General Hospital for the management of this case.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.