
Abstract
Objective
To evaluate the efficacy and safety of a 1470 nm/980 nm dual-wavelength laser system used for the en-bloc resection of non-muscle invasive bladder cancer (NMIBC) compared with transurethral resection of bladder tumour (TURBT).
Methods
This retrospective study analysed the demographic and clinical data from patients diagnosed with NMIBC that were treated by either dual laser or TURBT. Intraoperative characteristics, postoperative characteristics and outcomes between the two groups were compared.
Results
This study analysed 64 patients, 32 in each group. No severe complications were identified in either group. After propensity score-matching, there were no significant differences between the two groups in terms of the demographics, clinical and tumour characteristics. There was no significant difference between the two groups in terms of specimen quality. In the laser group, intraoperative blood loss was significantly lower and significantly fewer patients required continuous bladder irrigation after surgery, compared with the TURBT group. No significant differences were observed in the catheterization time, gross haematuria time and hospitalization time. Operation time in the laser group was significantly longer compared with the TURBT group. No significant difference was found in the recurrence and progression rates between the two groups.
Conclusions
The 1470 nm/980 nm dual-wavelength laser provides a safe and effective surgical treatment option for patients with NMIBC.
Introduction
Bladder cancer ranks eleventh among the most common cancer types in the world. 1 An epidemiological study has shown that more than 430 000 patients are diagnosed with bladder cancer annually. 2 It is estimated that the lesions in approximately 75% of patients are predominantly restricted within the mucosal layer (Ta, CIS) or submucosal layer (T1). 3 As a result, this type is defined as non-muscle-invasive bladder cancer (NMIBC). 4 Despite being at a relatively early stage, NMIBC is associated with recurrence and progression, thus placing a heavy economic burden on patients as well as public healthcare welfare. 5
The most widely applied surgical procedure for NMIBC is transurethral resection of bladder cancer (TURBT), which is targeted to obtain pathological specimens to ensure an accurate diagnosis and to completely remove all visible tumour lesions. 6 Conventional TURBT surgery takes advantages of monopolar or bipolar current to remove tumour tissues using the fractioned technique, but this can lead to complications such as blood loss and obturator nerve reflex and bladder perforation. 7 In recent years, in order to avoid these complications, various lasers have been developed and used as energy sources to eradicate tumour tissues. For example, the types of lasers include holmium laser, potassium-titanyl-phosphate laser, green-light laser, 1.9 µm Vela laser and thulium:yttrium-aluminum-garnet laser.8–12 Numerous studies have demonstrated that these laser systems are safe and regarded to be appropriate alternative energy sources for the therapy of NMIBC.8–12 Meanwhile, some lasers has been shown to have a high capacity to capture relatively higher quality specimens because of the efficient seizing of detrusor muscle compared with conventional TURBT. 13 The 1470 nm/980 nm dual-wavelength laser is a newly developed technique that possesses some unique advantages. 14 The 1470 nm part has the capability for rapid resecting and vaporizing; and the 980 nm part is typically characterized by high haemostasis efficiency and non-contact haemostasis. 15 These characteristics make the 1470 nm/980 nm dual-wavelength laser a very attractive approach for clinical applications. A recently published study showed that the 1470 nm/980 nm laser is also a safe and effective tool to treat vascular lesions. 16
However, there are no published reports on the application of 1470 nm/980 nm dual-wavelength lasers for the treatment of NMIBC. This current study compared the use of the 1470 nm/980 nm laser for en-bloc resection of NMIBC with conventional TURBT to evaluate the efficiency and safety of the 1470 nm/980 nm laser.
Patients and methods
Patient cohort
This retrospective study analysed the clinical data from consecutive patients that were treated by either dual laser or TURBT at the Department of Urology, Changsha Central Hospital, Changsha, Hunan Province, China from August 2013 to July 2020. Patients were enrolled and then divided into two groups according to the surgical method. All patients had received a comprehensive preoperative evaluation. The preoperative evaluation included detailed medical history, complete physical examination, laboratory examination results, imaging examination results and results for heart and lung function. The inclusion criteria were as follows: (i) clinically diagnosed as primary bladder cancer by enhanced computed tomography (CT) of the urinary system or cystoscopy; (ii) had not previously undergone TURBT; (iii) had upper urinary tract imaging results to exclude upper urinary tract tumours; (iv) no distant metastases or other tumours. The exclusion criteria mainly depended on the pathological examination: (i) unable to stage; (ii) muscular invasive bladder cancer; (iii) non-transitional epithelial carcinoma; (iv) benign tumour tissue, non-tumour tissue or metastatic tumour tissue.
This study conformed to the Declaration of Helsinki and was approved by the Ethics Committee of Changsha Central Hospital, Hunan Province, Changsha, China (no. 2021-S0001), which waived written informed consent because of the retrospective nature of this study. The reporting of this study conforms to STROBE guidelines. 17
Surgical techniques
All TURBT surgeries were performed by the same surgeon while all dual laser surgeries were performed by an independent surgeon. Under general anaesthesia, patients were placed in the lithotomy position. For the laser group, en-bloc resection was performed with a 1470 nm/980 nm LEONARDO® DUAL 45 Laser System (Biolitec, Wien, Germany). A 24Fr laser resectoscope was used to enter the bladder through the urethra, which was customized exclusively for laser-guided surgery. The bladder was thoroughly examined, including the bladder neck, bladder triangle, posterior wall, lateral wall, anterior wall and the opening of the ureter. Once the tumour base has been determined, the tumour was carefully checked and its diameters were recorded, including the maximum tumour diameter, tumour number, tumour location and tumour appearance. The laser fibre was carefully inserted into the bladder through the laser resectoscope. At a position proximal to the base of the tumour, a circular incision was performed at a relatively safe distance, which was defined as approximately 1.0 cm. The submucosal blood vessels were subsequently exposed to the laser (30 W), avoiding direct contact and were coagulated to block the blood supply to the tumour. If there was any bleeding on the surface of the tumour, the laser was also used to staunch the flow. Another circular incision on the base of the tumour was also completed at a distance of 1.0 cm. The laser (30 W) was utilized to directly touch the mucosa along the circular incision track and then cut vertically from the mucosa layer into the space between the submucosa layer and the muscular layer. The tongue-like front of the resectoscope’s sheath and the laser fibre were used to push the tumour base in the space between two layers. If there was a tight connection between the mucosa layer and the deeper muscular layer, the laser was used to remove the muscle fibre until the incision reached the outer bladder membrane and the structure of the extra-bladder fat was exposed. The surgeon resected and pushed around the tumour in different directions until the tumour was completely removed en-bloc at the visible anatomical level. A 20F three-way catheter was routinely placed.
For the TURBT group, patients were treated according to standard TURBT routines 18 using a 25.5Fr continuous-flow resectoscope (Richard Wolf, Knittlingen, Germany). The electro-resecting power was set at 100 W and the electro-coagulating power was set to 40 W. A piece-by-piece resection to the muscular layer was performed to remove the body of the tumour gradually and steadily.
Postoperative procedures
All specimens were submitted for pathological examination. All patients in both groups underwent intravesical instillations with 50 mg epirubicin as postoperative adjuvant chemotherapy, which started within 1 h following the operation. After that, weekly intravesical instillation for 8 weeks with 50 mg epirubicin started 1–2 weeks after the operation followed by monthly intravesical instillations with 50 mg epirubicin for 1 year (a total of 18 intravesical instillations). All patients were followed up with ultrasonography and cystoscopy every 3 months for the first 2 years and every 6 months to 3 years. Recurrence-free survival (RFS) and progression-free survival (PFS) were defined as the time starting from the end of the operation to the pathological diagnosis of NMIBC and the pathological diagnosis of muscle invasive bladder cancer or metastasis, and death, respectively.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 23.0 (China IBM Co.; Beijing, China) and the R statistical package (R version 3.3.2; R Foundation for Statistical Computing, Vienna, Austria). Continuous data are presented as mean ± SD and compared using Student’s t-test. Categorical variables are presented as n of patients and were compared using χ2-test or Fisher’s exact test. Ordered categorical data were analysed using Mann–Whitney U-test. Survival data (RFS and PFS) were determined using the Kaplan–Meier method and the log-rank test. A propensity score-matched (PSM) analysis was completed using a multivariable logistic regression model based on sex and tumour location. Pairs of receiving dual-laser or TURBT patients were derived using 1:1 greedy nearest neighbour matching within a propensity score of 0.05. A P-value <0.05 was considered statistically significant.
Results
This retrospective study initially enrolled 94 patients based on the inclusion criteria and divided them into two groups according to the surgical method: dual laser group (n = 45) and TURBT group (n = 49). Following exclusion based on the criteria, 64 patients were successfully enrolled in the study, 32 in each group (Figure 1). The demographic, clinical and tumour characteristics of the patients before and after propensity score-matching are summarized in Table 1. After propensity score-matching, there were no significant differences between the two groups in terms of the demographics, clinical and tumour characteristics of the patients.
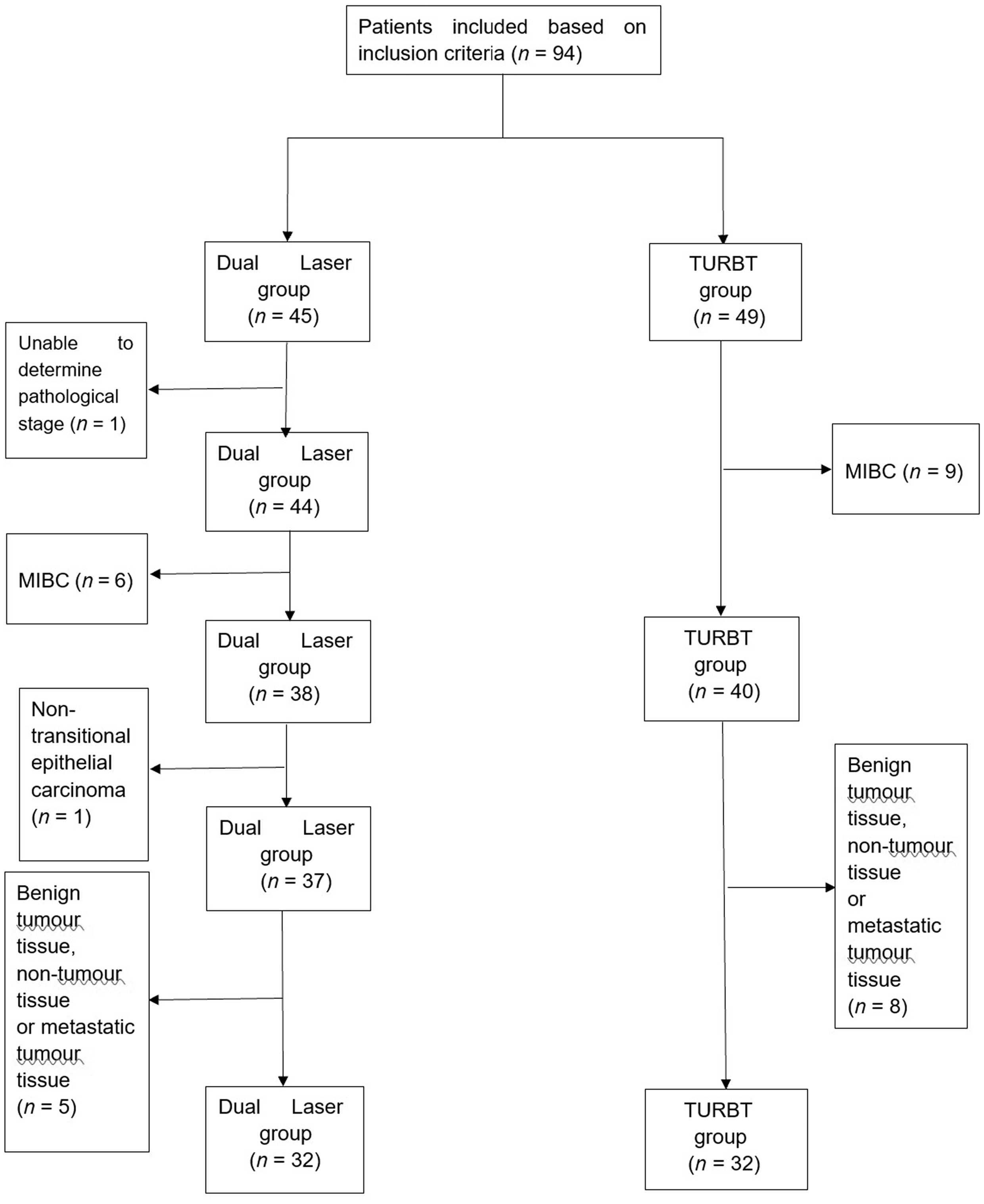
Flow diagram showing the selection procedure for the enrolment of patients to a study that compared the use of the 1470 nm/980 nm laser for en-bloc resection of non-muscle-invasive bladder cancer with conventional transurethral resection of bladder cancer (TURBT). MIBC, muscle invasive bladder cancer.
Demographic, clinical and tumour characteristics of patients (n = 64) enrolled in a study that compared the use of the 1470 nm/980 nm laser for en-bloc resection of non-muscle-invasive bladder cancer with conventional transurethral resection of bladder cancer (TURBT).

Data presented as mean + SD or n of patients (%).
aBetween-group comparisons undertaken using Student’s t-test for continuous data and χ2-test or Fisher’s exact test for categorical data; NS, no significant between-group difference (P ≥ 0.05).
PUNLMP, papillary urothelial neoplasm of low malignant potential.
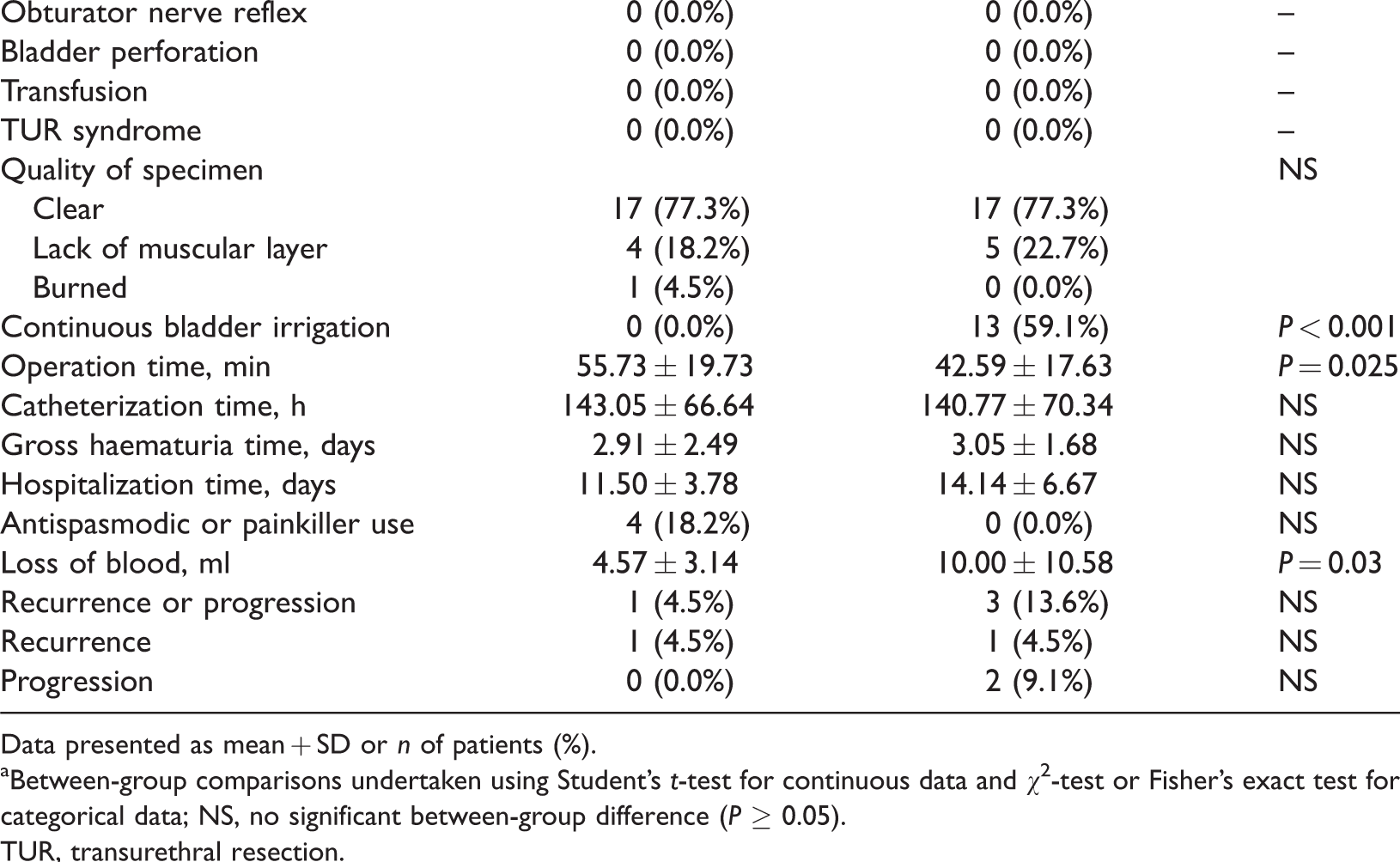
Intraoperative and postoperative data are presented in Table 2. No severe complications including obturator nerve reflex, bladder perforation and transurethral resection syndrome arose in either group and blood transfusion was not needed by any patients. There was no significant difference between the two groups in terms of the quality of the specimens. The number of patients that required continuous bladder irrigation in the laser group was significantly lower than that in the TURBT group (P < 0.001). The laser group experienced significantly less blood loss during surgery than the TURBT group (P = 0.03). There were no significant differences between the two groups in terms of catheterization time, gross haematuria time and the hospitalization time. The operation time in the laser group was significantly longer compared with the TURBT group (P = 0.025). There was no significant difference between the two groups in terms of the number of patients that needed antispasmodics or painkillers.
Intra- and postoperative characteristics of patients (n = 64) enrolled in a study that compared the use of the 1470 nm/980 nm laser for en-bloc resection of non-muscle-invasive bladder cancer with conventional transurethral resection of bladder cancer (TURBT).
Data presented as mean + SD or n of patients (%).
aBetween-group comparisons undertaken using Student’s t-test for continuous data and χ2-test or Fisher’s exact test for categorical data; NS, no significant between-group difference (P ≥ 0.05).
TUR, transurethral resection.
All patients were followed up for a median of 30.5 months after surgery. During the observation period, there were no significant differences between the two groups in terms of the rates of recurrence and progression. Two patients in the TURBT group were diagnosed with disease progression and died within 1 month of the diagnosis. As shown in Figure 2, there were no significant differences in terms of RFS or PFS between the two groups.

Kaplan–Meier survival analyses showing time to recurrence and progression in a study that compared the use of the 1470 nm/980 nm laser for en-bloc resection (group 1) of non-muscle-invasive bladder cancer with conventional transurethral resection of bladder cancer (group 2). The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
In spite of the fact that TURBT is still the most widely used technique to diagnose and treat NMIBC, the advantages of laser system in treatment of NMIBC are obvious.19–22 However, there are no published reports on the application of 1470 nm/980 nm dual-wavelength lasers for the treatment of NMIBC.
This current study demonstrated that laser resection was as safe and effective as TURBT for the treatment of NMIBC. A previous meta-analysis conducted on a total of 17 studies consisting of 2439 participants suggested that laser surgery demonstrated a lower chance of causing complications, such as obturator nerve reflex and bladder perforation. 23 During the TURBT operation, the current frequently released by the electrode loop may stimulate the obturator nerves near the inferolateral bladder wall, bladder neck and lateral prostatic urethra, thus causing the adductor muscles to contract abruptly, leading to secondary bladder perforation. 24 The 1470 nm/980 nm dual-wavelength laser system uses a specialty optical fibre to emit and transmit the laser, which is in turn absorbed by tissues and produces vaporization, cutting and coagulation effects. No current will pass through the obturator nerve; therefore, the risks of obturator nerve reflex and secondary bladder perforation are minimized. In the present study, none of the patients in the laser group showed such complications. Although there was no statistical difference in terms of complications between the two groups, it still verifies the safety of the 1470 nm/980 nm laser.
Bleeding is a severe complication that should not be ignored during bladder tumour resection. In this current study, the 1470 nm/980 nm laser system demonstrated some advantages over TURBT in reducing continuous bladder irrigation and blood loss. This was likely due to the combination of the 1470 nm and 980 nm lasers. The 1470 nm part is highly absorbed by water, so the efficiency of resecting and vaporizing tumour is relatively high. 25 This also means a thinner coagulation layer. 26 Meanwhile, the 980 nm part is typically characterized by a high haemoglobin absorption rate and low water absorption rate. 27 A high haemoglobin absorption rate makes haemostasis more efficient; and a low water absorption rate enables the laser to penetrate the water layer for non-contact haemostasis by reducing water-caused energy loss. 27 Because of the high resecting efficiency of the 1470 nm laser, it might be expected that the operation time needed for the 1470 nm/980 nm laser would be shorter than for TURBT. Intriguingly, the operation time in the 1470 nm/980 nm laser group was significantly longer than the TURBT group in the current study. It could be that the lack of sufficient skills and familiarity with this new technology may account for these results.
Many types of lasers have been reported to use en-bloc to eradicate bladder tumours.9,21,27,28 A retrospective study reported that the specimens obtained in the en-bloc way had a better presentation rate for the muscular layer. 29 It also greatly helps pathologists to stage/grade more accurately, reducing the probability of patients receiving a secondary TURBT due to poor specimen quality. 30 En-bloc resection is a circular cutting rather than a piece-by-piece cutting process. 31 The cutting plane is relatively neat and the specimens are more integrated than those achieved with TURBT. 32 Because the 1470 nm/980 nm laser resection possesses high resecting efficiency and a thin coagulation layer, and it can be used for non-contact haemostasis to prevent the muscular layer from being burnt, the quality of the specimens collected from patients in the laser group would be expected to be higher than those collected using TURBT. However, these current results demonstrated no significant difference in the quality of the specimens between the two groups. These current findings suggest that the current lack of familiarity with 1470 nm/980 nm laser en-bloc resection may have led to unnecessary cutting or coagulating time and insufficient accuracy of layer identifications, therefore affecting the quality of the pathological specimens. Another advantage of 1470 nm/980 nm laser en-bloc resection is, unlike TURBT, the tumour tissues will be cut into small pieces of approximately 5 mm, which will float in the bladder with the normal saline. However, it follows the ‘no-touch principle’, which theoretically reduces the postoperative recurrence rate. 33 In this current study, the recurrence and progression rates between the two groups were not significantly different, which was consistent with results from a previously published meta-analysis on the en-bloc treatment of bladder tumours. 34 Bladder tumours are clinically multicentric and individual recurrence varies greatly. 35 The surgeon’s judgement on the depth of tumour invasion and the completeness of tumour resection all have a significant impact on tumour recurrence and progression. While a recent article indicated that the recurrence rate after TURBT is significantly lower in patients undergoing androgen suppression therapy with 5-alpha-reductase inhibitors/androgen deprivation therapy, 36 the intraoperative and postoperative measures to prevent postoperative recurrence and progression remain to be further elucidated. Hexaminolevulinate blue light cystoscopy-assisted transurethral resection of the NMIBC may be a new noteworthy approach. 37
This current study had several limitations. First, because the 1470 nm/980 nm dual-wavelength laser is a novel energy source for the resection of bladder tumours, the number of patients was limited. This may increase the probability of statistical errors. Secondly, since the dual-wavelength laser was launched in China in 2015 and the first time Changsha Central Hospital used it was July 2017, few patients in the laser group had been followed up for at least 20 months. This could bias the current results and requires a longer follow-up period. Prospective multicentre studies are needed to reduce selection bias.
In conclusion, en-bloc resection with a 1470 nm/980 nm dual-wavelength laser system decreased intraoperative bleeding and the probability of continuous bladder irrigation without increasing the postoperative recurrence and progression rates compared with TURBT. The safety of the 1470 nm/980 nm dual-wavelength laser system in terms of complications was similar to that of TURBT. This novel technology provides an appropriate alternative treatment option for patients with NMIBC.
Footnotes
Author contributions
Y.H.W. made a substantial contribution to the concept of the work and revised the paper. J.H.F. and F.J.F. collected, analysed and interpreted the data; and wrote the manuscript. All authors read and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.