
Abstract
Objective
The aim of this study was to systematically examine the literature and assess the effects of perioperative dextrose infusion on the prevention of postoperative nausea and vomiting (PONV) in patients following laparoscopic surgery under general anesthesia.
Methods
We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs). Studies were eligible for inclusion if they evaluated the prevention of PONV with perioperative intravenous dextrose. Studies listed in PUBMED, Web of Science, and EMBASE databases published up to December 2020 were identified. Data were extracted and analyzed independently using a fixed-effects or random-effects model according to the heterogeneity.
Results
Six RCTs involving 526 patients were included. Our results showed that perioperative dextrose infusion not only reduced the incidence of PONV (risk ratio [RR] = 0.61, 95% confidence interval [CI]: 0.39–0.95; I2 = 59%) but also decreased the requirement for antiemetics compared with the control (RR = 0.53, 95% CI: 0.42–0.66; I2 = 32%). Furthermore, perioperative glucose infusion did not increase blood glucose levels compared with the control (mean difference [95% CI] = 74.55 [−20.64 to 169.73] mg/dL; I2 = 100%).
Conclusion
Our study reveals that perioperative dextrose infusion may reduce the risk of PONV after laparoscopic surgery. However, additional population-based RCTs are needed to confirm this finding.
Keywords
Introduction
The implementation of laparoscopic techniques has increased in recent decades 1 because they are associated with less postoperative pain and morbidity, a reduced length of hospital stay, and a faster recovery2,3 compared with laparotomy. However, several studies have shown that patients who undergo laparoscopic surgery under general anesthesia are notably susceptible to post-operative nausea and vomiting (PONV) because abdominal gas insufflation may stimulate mechanoreceptors in the intestine, leading to serotonin release and consequent activation of 5-HT3 receptors.4–6 PONV not only increases patient physical and psychological dissatisfaction, but it may also increase the risk of undesirable adverse effects, such as dehydration, electrolyte imbalance, bleeding, and surgical wound disruption, which leads to prolonged recovery, life-threatening aspiration, delayed hospital stays, and increased medical care costs.7,8 Despite great advances in antiemetic strategies, PONV continues to be a frequent and distressing postoperative complication after anesthesia and surgery.9,10 Therefore, treating and preventing PONV is critical to improve patient safety, accelerate postoperative recovery, reduce medical costs, and increase patient satisfaction.8,11
Currently, a variety of antiemetic drugs are used to control PONV, including antihistamines, serotonin 5-HT3 receptor antagonists, dopamine antagonists, steroids, or droperidol.12–14 However, these agents cause adverse reactions, such as hallucinations, headache, restlessness, dry mouth, extrapyramidal symptoms, excessive sedation, hypotension, and dystonic effects, and increase treatment costs.15,16 Recently published evidence suggests that perioperative dextrose infusion may control PONV, but its efficacy remains debatable.17–19 Therefore, this meta-analysis systematically assessed the effects of perioperative dextrose infusion on preventing PONV in patients after laparoscopic surgery under general anesthesia. We hope the results will increase awareness and provide suggestions for surgeons and anesthesiologists to make better treatment plans in the future.
Materials and methods
Literature retrieval strategy
A systematic literature retrieval strategy was implemented by two independent reviewers (RD and WL) using the Web of Science, Google Scholar, PubMed, and EMBASE databases from the date of their inception to 10 November 2020. Only studies reported in English were considered. The following key words were used to screen all potentially related studies: “postoperative nausea and vomiting”, “nausea”, “vomiting”, “PONV”, “dextrose”, “carbohydrate solution”, “randomized controlled trial”, and “RCT.” A manual search was performed by screening the references listed in all identified studies for additional studies. Ethical approval and informed patient consent were not applicable because this was a meta-analysis.
Inclusion and exclusion criteria
The relevant studies were included according to the following criteria: (1) intervention with perioperative dextrose infusion and control; (2) a randomized controlled trial (RCT) design; (3) laparoscopic surgery under general anesthesia; and (4) main results included the incidence of PONV, need for rescue antiemetic therapies, and postoperative blood glucose levels. The exclusion criteria were (1) non-clinical trials; (2) incomplete data; or (3) case reports, reviews, letters, or conference abstracts.
Data extraction and quality evaluation
The relevant data were independently collected from the included studies by two authors (RD and GH), including the publication year, country, first author name, interventions, sample size, and main outcomes. A quality assessment of the included articles was carried out by two reviewers (RD and XL) according to the Cochrane Handbook for Systematic Reviews of Interventions. The following items were included to evaluate the risk of bias within individual studies: random sequence generation, allocation concealment, blinding, incomplete outcome data, and free of selective reporting and other biases. When necessary, all contradictions were solved by consulting a third reviewer (XL).
Statistical analysis
All statistical analyses were performed using Review Manager (RevMan) Version 5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Dichotomous data were expressed as the risk ratio (RR) with 95% confidence intervals (CIs). Furthermore, continuous results were presented as mean differences (MDs) with 95% CIs. The meta-analysis was conducted according to the Mantel–Haenszel method with a fixed-effects model or random-effects model based on heterogeneity. Heterogeneity across studies was assessed using I2 statistics and Chi-square tests. When P < 0.05 and I2 < 50%, the fixed-effects model was used for the analysis. Otherwise, the random-effects model was applied. Funnel plots were used to evaluate publication bias. P < 0.05 was considered statistically significant.
Results
Study characteristics and quality assessment
The flowchart of the literature inclusion process and results are presented in Figure 1. Initially, 245 published articles were selected after removing duplicates from 362 studies identified in the electronic databases. Then, 227 apparently irrelevant articles were excluded after screening titles and abstracts. The remaining 18 full-text studies were reviewed carefully, and an additional 12 articles were excluded for the reasons described in Figure 1. Finally, six eligible studies17,20–24 involving 526 patients were included in this meta-analysis. The basic features of each article are shown in Table 1. Furthermore, the risk of bias in all studies according to the authors’ assessment is presented in Table 2.

Flow diagram of the selection of randomized controlled trials for inclusion in the meta-analysis.
Characteristics of the studies included in the review.

PACU: post-anesthesia care unit; PONV: postoperative nausea and vomiting.
Quality assessment of the included studies.

Incidence of PONV
As shown in Figure 2, four RCTs17,20,22,24 with 356 patients reported perioperative dextrose administration and the incidence of PONV following laparoscopic surgery under general anesthesia. Compared with the control group, there was a statistically significant reduction in the incidence of PONV in the dextrose group (RR = 0.61, 95% CI: 0.39–0.95; I2 = 59%; P = 0.03), which was pooled according to the random-effects model because of the high heterogeneity of the included studies (Figure 2).
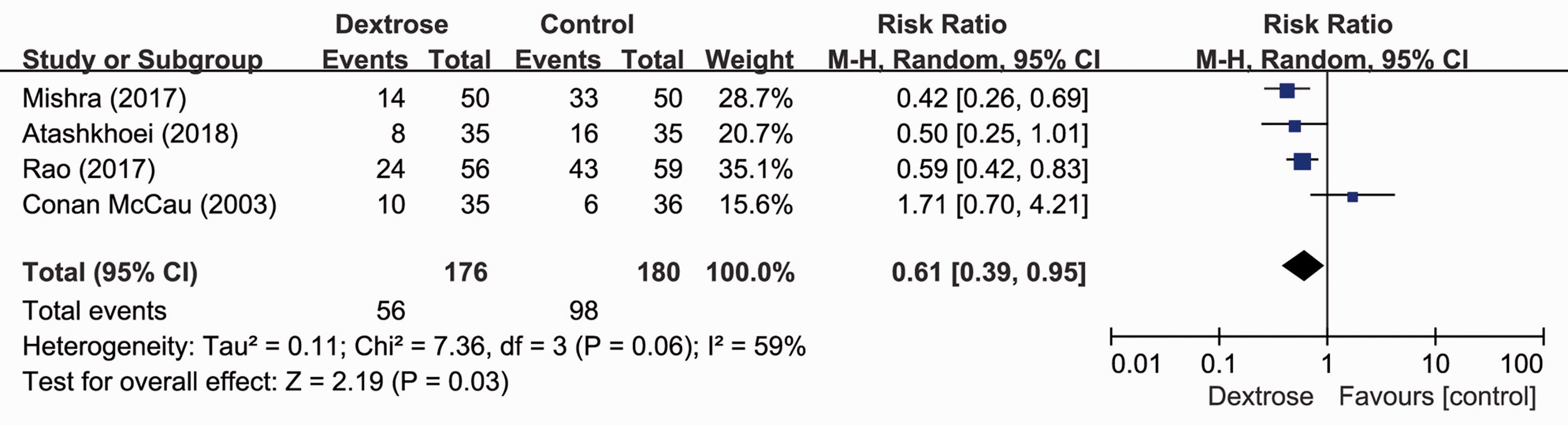
Forest plots and meta-analysis of PONV.
Requirement for antiemetics
As shown in Figure 3, there were five studies17,20,21,23,24 involving 455 patients that reported the use of antiemetic drugs (228 in the control group and 227 in the dextrose group). Compared with the control group, the pooled analysis of these studies via a fixed-effects model showed there was a statistically significant reduction in the use of antiemetic drugs in the dextrose group (RR = 0.53, 95% CI: 0.42–0.66; I2 = 32%; P < 0.00001) (Figure 3).

Forest plots and meta-analysis of the requirement for antiemetics.
Glucose levels
Three included studies20,23,24 with 306 patients reported the side effects (glucose level) after dextrose infusion. Compared with the control group, the results of our meta-analysis indicated that perioperative dextrose administration did not increase blood glucose levels (MD [95% CI] = 74.55 [−20.64–169.73] mg/dL), which was pooled according to the random-effects model because of the substantial heterogeneity (I2 = 100%) (Figure 4).

Forest plots and meta-analysis of glucose levels.
Publication bias and sensitivity analysis
A funnel plot was used to qualitatively evaluate publication bias (Figure 5). The shape of the funnel plot was partially symmetrical, indicating no significant evidence of asymmetry and no obvious evidence of publication bias. The sensitivity was evaluated, and the exclusion of any study did not impact the pooled estimates of RRs, indicating the reliability and stability of the results.

Funnel plot for detecting publication bias in the included literature.
Discussion
Currently, PONV remains a significant complication in clinical practices under general anesthesia, especially laparoscopic surgery. 25 Abdominal gas infusion may stimulate mechanoreceptors of the gastrointestinal tract, resulting in the release of serotonin and the consequent activation of 5-HT3 receptors. 26 As a result, patients undergoing laparoscopic surgery are more likely to develop PONV. Previous meta-analyses have evaluated the effects of perioperative dextrose infusion on the prevention of PONV.27,28 However, the clinical applicability of previous meta-analyses was ambiguous because they involved different types of surgery, which led to an increased risk of bias. In our meta-analysis, we assessed the effects of perioperative glucose infusion on the prevention of PONV after laparoscopic surgery. Our results indicated that intraoperative infusion of dextrose not only reduced the incidence of PONV but also decreased the need for antiemetic drugs after general anesthesia.
The results of our study were partially consistent with those of previous meta-analyses.27,28 Mishra et al. 17 reported that intraoperative infusion of dextrose after laparoscopic surgery significantly decreased the incidence of PONV. In addition, Atashkhoei et al. 24 revealed that the administration of intravenous dextrose reduced the incidence and severity of PONV in patients undergoing laparoscopic surgery and rescue antiemetic treatment. Combined with these earlier studies, our results convincingly indicated that intravenous dextrose administration during laparoscopic surgery was associated with a reduction in the incidence of PONV and antiemetic requirements.
The preoperative fasting period is the prescribed time before any operation under general anesthesia, and oral liquids or solids are not allowed during this time. We considered intravenous administration a safe and efficient method to administer dextrose to surgical patients, especially those who cannot be fed orally. The intraoperative infusion of glucose dose in 4/6 included studies20,22–24 was ≥25 g, which is equal to 500 mL of a 5% glucose solution. Our results indicated that intravenous glucose infusion did not evidently increase blood glucose levels. However, a previous study reported that ≥50 g of glucose supplementation increased blood glucose levels to >200 mg/dL after infusion. 20 Studies have shown that perioperative hyperglycemia increases the risk of surgical site infection.29,30 Therefore, the volume of dextrose administered is worth further exploration.
The mechanism by which intravenous glucose improves PONV is unclear. It may be associated with a reduction in hyperglycemia-induced gastric acid secretion. Additionally, gastric contractions and nausea may be caused by increased gastric acid secretion. 31 Studies have found that blood glucose might inhibit gastric acid secretion by regulating the vagal cholinergic pathways.32,33 Furthermore, intraoperative infusion of glucose may contribute to postoperative insulin resistance, potentially leading to PONV.34,35 Additionally, higher blood glucose levels increase plasma cholecystokinin, which regulates pain and anxiety through the brain to reduce pain and PONV.36,37 Postoperative pain is a known risk factor for PONV. 38
Our study had some strengths. First, this analysis quantitatively evaluated the efficiency of dextrose infusion in the prevention of PONV after laparoscopic surgery under general anesthesia. Second, the methodology applied in this meta-analysis was strict because all selected studies were prospective RCTs. Third, the quality of all included studies was relatively high. Fourth, the funnel plot did not show significant evidence of asymmetry, indicating the reliability and stability of the results.
Despite these important findings, our meta-analysis has several limitations. First, our analysis involved only six RCTs, and the number of participants was relatively small. Second, subgroup analyses were not carried out due to the limited number of identified studies; therefore, the source of heterogeneity could not be determined. Third, because all RCTs were restricted to the English language, important studies reported in other languages may have been missed, thereby introducing a language bias. Fourth, we investigated relatively healthy patients undergoing laparoscopic surgery. Therefore, these results cannot be extrapolated to patients with major comorbidities or diabetes mellitus. Finally, although all selected studies were RCTs, some did not describe the randomization methods, blinding procedures, or missing data, which might have led to a high risk of publication and selection bias (Figure 5).
Our analysis suggests that perioperative dextrose infusions significantly reduce the incidence of PONV and the requirement for antiemetic drugs in patients after laparoscopic surgery. However, the above evidence needs to be further verified in large, multi-center, elegantly designed RCTs.
Footnotes
Author contributions
XL and RD conceived and designed the study. WL and RD conducted the data searches. GH and RD performed the analysis and wrote the manuscript. RD revised the manuscript. XL gave the final approval of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.