
Abstract
Background
This meta-analysis was performed to evaluate the efficacy and safety of palonosetron and ondansetron in preventing postoperative nausea and vomiting (PONV) in patients undergoing laparoscopic surgery with general anesthesia.
Methods
We searched for randomized controlled clinical trials in PubMed, Embase, and The Cochrane Library.
Results
Nine studies were enrolled in this meta-analysis and showed no statistically significant difference between palonosetron and ondansetron in the prevention of PONV in the first 24 hours after surgery (relative risk [RR], 0.62; 95% confidence interval [CI], 0.35–1.10). Palonosetron more effectively prevented vomiting at various time intervals during the first 24 hours postoperatively than did ondansetron: 0–2 hours (RR, 0.45; 95% CI, 0.26–0.78), 2–6 hours (RR, 0.74; 95% CI, 0.39–1.40), and 6–24 hours (RR, 1.20; 95% CI, 0.55–2.64). No significant differences in side effects were found between palonosetron and ondansetron (RR, 0.67; 95% CI, 0.40–1.14).
Conclusion
This meta-analysis demonstrated that palonosetron is not more efficacious than ondansetron in the prevention of early PONV. However, palonosetron was more efficacious than ondansetron in the prevention of vomiting after laparoscopic surgery.
Keywords
Introduction
During the last few decades, more effective drugs have been introduced into anesthesia practice and anesthetic techniques have rapidly improved. However, postoperative nausea and vomiting (PONV) in patients undergoing laparoscopic surgery remains one of the most common problems of anesthesia, occurring at an incidence of up to 70%. 1 PONV may be related to activation of the following four vomiting centers: the vestibular system, the chemoreceptor trigger zone, the gastrointestinal vagal nervous system, and the cortical center. A variety of neurotransmitters in these four areas transmit nerve impulse information to a vomiting center in the medulla. This completes a series of visceral and physical reactions that include nausea and vomiting. PONV not only causes pain but also gives rise to dehydration, anxiety, acid–base imbalance, electrolyte imbalance, and wound dehiscence; some patients even develop esophageal tears, hernias, aspiration pneumonia, and pneumothorax. PONV can prevent postoperative recovery and utilize enormous hospital resources. 2
Many recent studies have confirmed that 5-HT3 antagonists, which are anti-emetic agents, can prevent PONV. Thus, these drugs have been widely applied for this purpose. The most common 5-HT3 antagonists currently in use include ondansetron, ramosetron, tropisetron, and granisetron. Additionally, palonosetron hydrochloride is a novel long-acting 5-HT3 receptor antagonist. In 2003, the US Food and Drug Administration approved palonosetron for the treatment of acute and delayed nausea as well as vomiting and PONV.3,4 Ondansetron and palonosetron, as first- and second-generation 5-HT3 antagonists, respectively, have been broadly used in clinical practice. These two drugs exercise inhibition via presynaptic 5-HT3 receptors in the peripheral nervous system, thus effectively preventing nausea and vomiting. Compared with ondansetron, palonosetron has a longer half-life (about 40 hours), which increases its affinity to the 5-HT3 receptor by about 30 to 100 times. However, the results of many recent studies on the efficacy of ondansetron and palonosetron in preventing PONV in patients undergoing laparoscopic surgery are controversial. Therefore, the present meta-analysis was performed to evaluate the effectiveness of ondansetron and palonosetron in the prevention of PONV in patients undergoing laparoscopic surgery.
Materials and Methods
Inclusion criteria
The inclusion criteria for this meta-analysis were as follows. (1) The study was a randomized controlled trial (RCT) using either allocation concealment or a blinding method; no language limitations were enforced. (2) The study subjects were patients undergoing laparoscopic surgery. (3) With respect to the intervention, either the experimental group received palonosetron while the control group received ondansetron, or the experimental group received palonosetron plus other drugs while the control group received ondansetron plus other drugs. (4) The measurement indices were the incidence of nausea and vomiting within 24 hours, postoperative dizziness, headache, and constipation.
Search strategy
The PubMed, Embase, and Cochrane Library databases were searched from January 1995 to June 2016. English search terms included palonosetron, nausea, vomiting, ondansetron, and laparoscopic surgery.
Literature screening and data extraction
We screened the literature based on the above-mentioned inclusion and exclusion criteria. After reading the titles and abstracts, we excluded unqualified articles. We then read the full texts of the articles that were potentially consistent with the inclusion criteria to determine their eligibility. Next, we checked the results of the included articles. Additionally, we extracted complete data from eligible RCTs. Two reviewers independently performed the above steps and cross-checked each other, consulting a third party when a disagreement was encountered. The two researchers extracted information in accordance with pre-established forms and employed a Jadad scale to evaluate the quality, specifically with regard to (1) whether the randomization method was appropriate, (2) whether randomization concealment was appropriate, (3) whether the blinding method was appropriate, and (4) whether reasons for withdrawals and dropouts were indicated.
Statistical methods
RevMan 5.1 software (Cochrane Collaboration, Copenhagen, Denmark) was used to conduct the meta-analysis. Heterogeneity of each enrolled study was evaluated using the χ2 test. When statistical homogeneity was found (P > 0.1, I2 < 50%), a fixed-effects model was used for the analysis; when statistical heterogeneity was found (P < 0.1, I2 > 50%), we analyzed the sources of heterogeneity and conducted a subgroup analysis according to potential factors that could have resulted in heterogeneity. A fixed-effects model was employed when high similarity was found among studies of subgroups and between subgroups (P > 0.1, I2 < 50%). A random-effects model was used when there was significant heterogeneity but no clinical heterogeneity or statistical significance. Descriptive analysis was used if heterogeneity between the two groups was too large. If necessary, sensitivity analysis was adopted to test the stability of the results.
Results
Basic information of included studies
In total, 64 related articles were evaluated using the above-described literature search method, and 11 were included after reading of the titles and abstracts. However, one article
5
without full text and one
6
without specific data were excluded. Therefore, nine RCTs7–15 were included in the meta-analysis (Figure 1). Basic information on these nine studies is shown in Table 1.
Flow diagram of the literature search. Characteristics and Jadad scores of the studies included in the meta-analysis.

Methodological quality assessment
Among the nine enrolled RCTs, eight used blinding methods exclusively and seven specifically used randomization. All studies provided a written record of withdrawals and dropouts and of adverse reactions to drugs. The results of the methodological quality assessments are shown in Table 1.
Outcomes
Primary outcome: PONV
PONV was recorded at different time intervals among the nine studies. The meta-analysis revealed no statistically significant difference in PONV between the palonosetron and ondansetron groups within 24 hours after surgery (relative risk [RR], 0.78; 95% confidence interval [CI], 0.50–1.24) (Figure 2). The I2 value of 76% implied significant heterogeneity. Further subgroup analyses based on different routes and doses of ondansetron and palonosetron showed little influence over the pooled results, and all of these analyses were also affected by heterogeneity.
Forest plot of relative risk of postoperative nausea and vomiting between palonosetron and ondansetron treatment.
However, the meta-analysis revealed a statistically significant difference in PONV between the palonosetron and ondansetron groups during the first 24 hours postoperatively (RR, 0.30; 95% CI, 0.15–0.60; P = 0.0006) (Figure 2).
Palonosetron was no more effective than ondansetron in the prevention of postoperative nausea during several time periods within 24 hours after surgery: 0–2 hours (RR, 0.92; 95% CI, 0.42–2.01), 2–6 hours (RR, 0.62; 95% CI, 0.27–1.42), and 6–24 hours (RR, 0.45; 95% CI, 0.20–1.03) (Figure 3). The I2 value of 38% suggested no significant heterogeneity.
Forest plot of relative risk of postoperative nausea between palonosetron and ondansetron treatment.
However, during several different time periods within the first 24 hours after surgery, palonosetron tended to be more effective than ondansetron in preventing postoperative vomiting: 0–2 hours (RR, 0.45; 95% CI, 0.26–0.78; P = 0.004), 2–6 hours (RR, 0.74; 95% CI, 0.39–1.40), and 6–24 hours (RR, 1.20; 95% CI, 0.55–2.64) (Figure 4). The I2 value of 19% indicated no significant heterogeneity. A 2013 study by Laha et al.
6
was not included in our meta-analysis because no detailed PONV outcomes were provided. Additionally, the results indicated that preoperative administration of a single intravenous dose of palonosetron was as effective as ondansetron in reducing the incidence of PONV.
Forest plot of relative risk of postoperative vomiting between palonosetron and ondansetron treatment.
Secondary outcomes: Side effects of palonosetron and ondansetron
The four studies with secondary outcomes provided full data on the side effects (e.g., headache, dizziness) of palonosetron and ondansetron after surgery. No fewer side effects were recorded for palonosetron than ondansetron (RR, 0.67; 95% CI, 0.40–1.14) (Figure 5). Moreover, no substantial heterogeneity was observed (I2 = 0%). Other studies, without offering detailed data on side effects, also revealed no statistically significant difference between palonosetron and ondansetron.
Forest plot of relative risk of side effects between palonosetron and ondansetron treatment.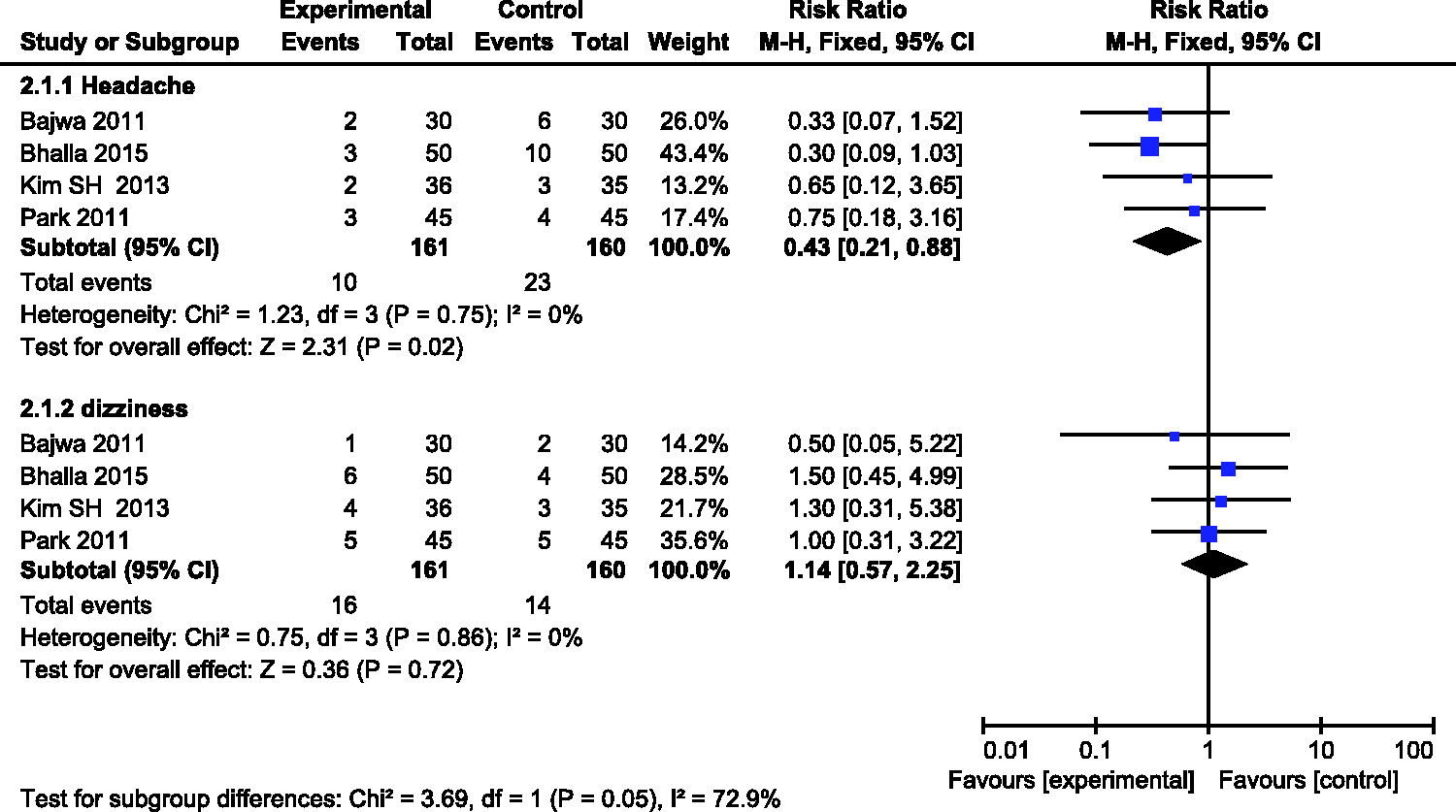
Publication bias analysis
A funnel plot analysis was conducted on all enrolled studies and showed good symmetrical results. This indicated that the meta-analysis is unlikely to have been affected by publication bias.
Discussion
This meta-analysis showed no difference between the effects of palonosetron and ondansetron in preventing PONV in patients undergoing laparoscopic surgery. Additionally, no differences were found between the two groups in the prevention of adverse reactions after laparoscopic surgery. However, palonosetron was more efficacious than ondansetron in the prevention of vomiting after laparoscopic surgery.
The PONV mechanism involves a variety of chemical mediators and receptors such as 5-HT3 receptors, dopamine, and histamine, with 5-HT3 receptors playing a major role. 16 5-HT3 receptors, mainly distributed in the central nervous system, can activate the chemoreceptor trigger zone in the small intestinal wall. Palonosetron produces a positive synergistic effect through allosteric and competitive inhibition, thus affecting the 5-HT3 receptor, while ondansetron (a first-generation 5-HT3 receptor antagonist) only selectively inhibits the 5-HT3 receptor. 17 Palonosetron suppresses activation of the presynaptic 5-HT3 receptor in the central nervous system, thus stopping signal transmission to the 5-HT3 receptor and reducing the incidence of nausea and vomiting. Ondansetron is also a 5-HT3 antagonist. This means that it can selectively bind with 5-HT3 receptors and reduce neuronal excitability in the nucleus of the solitary tract as well as in other parts of the vomiting center, thereby preventing nausea and vomiting.
The most common adverse reactions associated with PONV-preventing agents are constipation and headache, followed by diarrhea, fatigue, dizziness, and bloating. The present meta-analysis showed no significant differences in any of these adverse reactions between palonosetron and first-generation 5-HT3 receptor antagonists. Some studies have implied that 5-HT3 receptor antagonists can prolong the Q-T interval, leading to arrhythmias and even cardiac arrest. Popovic et al. 18 proved that palonosetron is safer than first-generation 5-HT3 receptor antagonists. Additionally, a recent systematic analysis 19 found no significant differences in the incidence of arrhythmias during administration, and the clinical value of electrocardiographic monitoring for all patients thus remains unclear. Therefore, further studies are needed.
Finally, although 5-HT3 receptors play an essential role in the pathogenesis of PONV, no relationship between the pathogenesis of PONV and 5-HT3 receptors was found when multiple risk factors were combined.
Several limitations of this meta-analysis should be considered. First, each study had issues regarding quality and design. Furthermore, the dosages and measurement times were not uniform. This may have given rise to clinical heterogeneity among the studies. In addition, wide differences in patients’ conditions may have been present because the inclusion criteria varied among the studies. More high-quality RCTs are needed to provide better clinical evidence with which to help clinicians make more rational clinical decisions and thus offer more precise and effective choices in the prevention of PONV in patients undergoing laparoscopic surgery.
Footnotes
Acknowledgements
The authors are grateful to You-Jing Luo, MD for her extensive support throughout the article writing process, which substantially improved the quality of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.