
Abstract
Pheochromocytoma is a rare and usually benign tumor of the adrenal glands. We report a case of a 40-year-old woman with recurrent pheochromocytoma and catecholamine cardiomyopathy. She had no history of other types of tumors or connective tissue disease. She had already undergone surgery twice to remove the pheochromocytoma, which had now recurred for the second time. A thrombus in the left ventricle was also noted upon imaging examination, which dissipated after anticoagulation therapy using dabigatran, allowing the patient to opt for an elective third surgery. This paper describes the clinical outcome of using the anticoagulant dabigatran to treat left ventricular thrombosis in this rare case of recurrent pheochromocytoma, and thus further contributing to the knowledge of the clinical management of this rare and complicated disease.
Keywords
Introduction
Pheochromocytoma, a rare tumor of the adrenal medulla, typically presents as persistent or paroxysmal hypertension, paroxysmal headache, hyperhidrosis, and tachycardia. Adrenal pheochromocytoma and secretory catecholamine paraganglioma are together referred to as pheochromocytoma, and their incidence is relatively rare, accounting for less than 0.2% of patients with hypertension. 1 Approximately 40% of reported cases of pheochromocytoma occur in relatively young individuals with a familial hereditary tendency that can be screened by genetic testing. 1 The other 60% are diagnosed by laboratory and imaging examinations. Research has shown that the abnormal secretion of catecholamines by pheochromocytomas not only leads to hypertension, but also causes coronary spasms and increased myocardial oxygen consumption. 2 The resulting metabolites directly damage cardiomyocytes and cause changes in cardiac structure and function; this phenomenon is known as catecholamine cardiomyopathy. Diagnosis is complicated owing to some cases having a series of cardiac complications that can be the initial symptoms of pheochromocytoma. 2 Only a small number of cases of catecholamine cardiomyopathy have been reported. Feng et al. 3 reported a case of a young male patient whose vital signs returned to normal after pheochromocytoma resection. His symptoms, namely heart failure and ventricular fibrillation, were well-controlled, the size of each cardiac chamber was reduced, and the ejection fraction increased to the normal level. Generally, surgical removal is the key treatment for these tumors. However, we report a case where the rare recurrence of the tumor was accompanied by a ventricular thrombus, which made surgical treatment difficult.
Case report
The patient was a 40-year-old woman with no history of tumor or connective tissue disease. Her personal and family history of disease were unremarkable. Symptoms of hyperhidrosis and palpitation first appeared in 2001. In 2003, she presented to a tertiary hospital for worsening of her symptoms, where she was diagnosed with pheochromocytoma. Physical examination revealed a blood pressure (BP) of 180/110 mmHg, and abdominal computed tomography (CT) revealed a substantial mass in the right adrenal gland. Laboratory examination showed elevated urine vanillylmandelic acid (VMA) concentration (127 µmol per 24 hours; normal range, 9.6–50 µmol per 24 hours). Therefore, right adrenal gland tumor resection was performed to remove an 8 × 8 × 8-cm3 irregular, hard mass, and pathological results confirmed the diagnosis (immunohistochemistry: chromogranin-A [++], neuron-specific enolase (NSE) [++], S-100 protein [+], adrenocorticotrophic hormone [+], proliferating cell nuclear antigen [+]). Postoperatively, her symptoms resolved, and BP stabilized at 120/80 mmHg. No reexamination was conducted after discharge.
Hyperhidrosis and palpitation recurred in June 2013. Upper abdominal CT suggested lesions occupying the inferior vena cava in the right adrenal area. In April 2014, the patient sought treatment in the same hospital where she was treated previously. Physical examination detected an elevated BP of 240/140 mmHg, and laboratory examination revealed increased urine VMA concentration (106.08 µmol per 24 hours), with increased urinary norepinephrine (5.7 × 103 nmol per 24 hours; normal range, 0.0–5.5 × 103 nmol per 24 hours). Upper abdominal CT showed a lumpy soft tissue density shadow beside the inferior vena cava, in the right adrenal gland area, which measured approximately 5.2 × 3.1 cm2. Enhanced CT showed uneven enhancement and lesion involvement in the upper pole of the right kidney along the fat gap. The lesion was larger than the previous mass, and tumor recurrence was considered. Because of the involvement of the inferior vena cava and the renal artery, the tumor was difficult to excise. She was referred to our hospital in May 2014. We suggested oral administration of sunitinib malate to control tumor progression. Inferior vena cava magnetic resonance imaging (MRI) revealed a space-occupying lesion in the right adrenal gland area accompanied by compression of the adjacent inferior vena cava. A 3.5 × 3.5 × 2-cm3 soft mass was removed from the right adrenal area, followed by pathological examination of the mass (immunohistochemistry: chromogranin A (CgA) [+], 35 H11 (−), ki-67 1% [+], NSE [−], synaptophysin (SYN) [++], vimentin [−]) (Figure 1). After surgery, sunitinib malate administration was terminated, and prednisone and phenoxybenzamine were administered orally, with instructions to the patients to take the medication exactly as prescribed. The BP was reported to be 150/80 mmHg and was accompanied by mild hyperhidrosis and fatigue. In August 2014, at our hospital, CT of the mid- and upper abdomen indicated no obvious postoperative abnormalities. In March 2015, the patient experienced severe sweating and presented to the endocrinology department. Because positron emission tomography-CT (PET-CT) showed no obvious abnormality in the surgical area, vagal nerve dysfunction was considered, and the patient recovered after comprehensive treatment with dexamethasone, phenoxybenzamine, valsartan, amlodipine, and ebastine. In February 2016, abdominal CT performed at our hospital revealed patchy enhancement of the right adrenal gland, without recurrence. Abdominal CT in January 2017, February 2018, and January 2019 showed that the change was unremarkable compared with the previous images.

Pathological photomicrographs are shown in figures a–c, and the findings supported the diagnosis of pheochromocytoma. Hematoxylin and eosin (HE) stain, ×200 (a and b); Immunohistochemical staining, × 200 (c).
In early 2019, symptoms of hyperhidrosis and palpitation reappeared. The patient underwent 131-I methoxyisobutylisonitrile imaging in July 2019, which showed that the structure of the right adrenal region was abnormal. A soft tissue density shadow was seen in the right adrenal region (Figure 2). Laboratory examination revealed that blood norepinephrine, dopamine, and adrenaline concentrations had increased to 2.36 × 104 pmol/L (normal range, 615–3240 pmol/L); 3.2 × 103 pmol/L (normal range, 0–650 pmol/L), and 880.0 pmol/L (normal range, 0–480 pmol/L), respectively. PET-CT revealed a patchy soft tissue shadow in the right adrenal region with uneven β-2-18F-fluoro-2-deoxy-D-glucose metabolism, suggesting reoccurrence of pheochromocytoma. Type B brain natriuretic peptide concentration was increased at 2.23 × 10−4 ng/L (normal range, 0–10 × 10−4 ng/L). In addition, other notable laboratory findings were elevated triglycerides: 1.87 mmol/L (normal range, 0.0–1.7 mmol/L), low density lipoprotein cholesterolemia: 3.77 mmol/L (normal range, 2.07–3.1 mmol/L), platelets: 332 × 109/L (normal range, 125–300 × 109/L), and hemoglobin: 155 g/L (normal range, 115–150 g/L), indicating the presence of hypercoagulability. Moreover, echocardiography revealed a lesion occupying the left ventricle, with no blood perfusion, combined with decreased left ventricular systolic and diastolic function (ejection fraction [EF]: 49%; early to late diastolic transmitral flow velocity [E/A]: 2.4). The mass appeared to be a thrombus; however, the pedicle was unclear (Figure 3). Cardiac MRI also showed a left ventricular middle segment nodular shadow (Figure 4). Whole-exome sequencing of all known genes was performed; however, no pheochromocytoma-associated variant was detected. A diagnosis of ventricular thrombus was considered after multi-disciplinary joint consultation with the departments of endocrinology, urology, oncology, cardiovascular surgery, and nuclear medicine in our hospital, and the patient was treated with dabigatran (110 mg orally, twice daily) as anticoagulant therapy. The size of the dense mass was reassessed by echocardiography monthly until elective surgery.

131-I methoxyisobutylisonitrile imaging showed an abnormal concentration of radioactivity in the right adrenal gland.
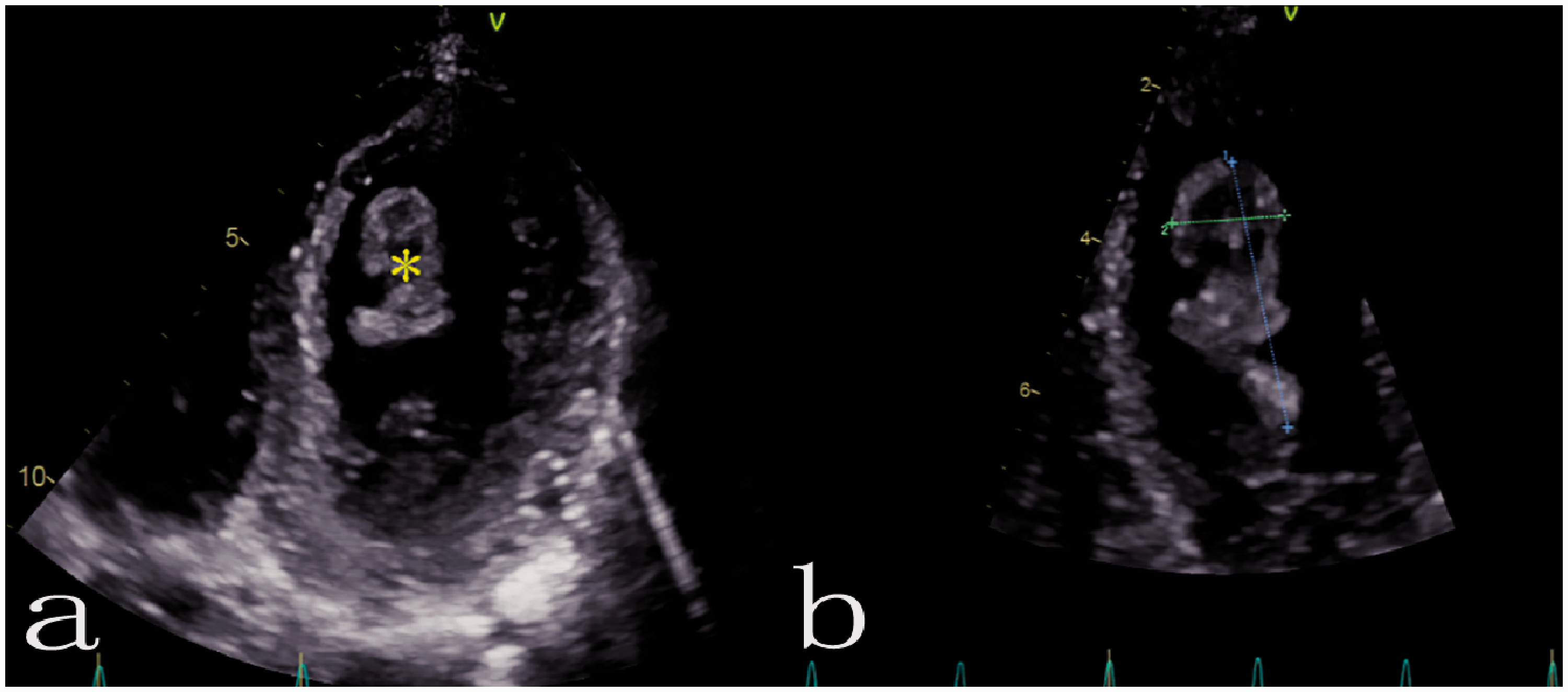
Echocardiogram showing an irregular left ventricular mass, which was a suspected thrombus (a); the thrombus dimensions are marked on the image (3.2 × 1.4 cm) (b).

Cardiac magnetic resonance imaging (MRI) showing a nodular mass in the middle left ventricle (1.9 × 1.3 cm) (a and b).
After the anticoagulation treatment, echocardiography performed in September 2019 showed no obvious regional wall motion abnormality, and the left ventricular lesion had disappeared (EF, 37%; E/A, 1.7) (Figure 5). The patient underwent surgical resection of the right adrenal gland tumor and the right kidney. Postoperatively, the symptoms of hyperhidrosis and palpitation had resolved. Echocardiography performed in April 2020 showed no thrombus in the left ventricle, and cardiac function had recovered significantly (EF, 78%; E/A, 0.9) (Figure 6).

Echocardiogram showing the absence of a thrombus after anticoagulation treatment.

Echocardiogram showing no evidence of a mass after surgical resection of the right adrenal gland tumor and right kidney (a and b).
Discussion
Mural thrombosis and systemic circulation embolism are common in patients with pheochromocytoma and catecholamine cardiomyopathy,4–6 but reports of recurrent cases are relatively rare. Our report may be a helpful addition to the body of literature on pheochromocytoma recurrence with ventricular thrombus. Shafiq et al. 7 reported a case of left ventricular thrombosis with EF retention; however, decreased ventricular wall function was revealed via echocardiography. Our patient showed a decrease in left ventricular function, but there was no obvious regional wall motion abnormality. Moreover, an interesting case reported by Pishdad et al. 8 was that of an 18-year-old female patient with neither left ventricular function nor wall movement abnormality on echocardiography, but with left ventricular thrombosis. The thrombus resolved after surgery, without anticoagulant therapy.
The incidence of left ventricular thrombosis is low in the general population, with most cases associated with cardiomyopathy. 9 However, this condition often occurs in patients with severe heart dysfunction. Characteristic imaging changes and gene variants highly-associated with primary cardiomyopathy were not found in our case. Electrocardiograms showed no significant abnormalities, and immune-related serological indices were also in the normal ranges. According to the patient's symptoms and related clinical examination findings, we eventually ruled out other causes. Slow blood flow, endothelial injury, and blood hypercoagulability were identified as the pathological mechanisms of most thrombi, including intracardial thrombi. 10 Decreased ventricular wall contractility or decreased left ventricular function often leads to slow intracavity blood movement, which increases the risk of left ventricular thrombosis. 10 In our case, the diagnosis of catecholamine cardiomyopathy was considered, accompanied by decreased left ventricular systolic and diastolic function. The increased type B brain natriuretic peptide concentration suggested that left ventricular dysfunction was the primary mechanism of the ventricular thrombosis. Although echocardiography showed that the sizes of each chamber were within the normal ranges, blood stasis resulting from increased left ventricular diameter has been considered another risk factor for left ventricular thrombosis. 9 Intermittent hypertension, which may cause endocardial damage, is also associated with thrombosis. 7 In addition, the elevated triglyceride concentration, low density lipoprotein cholesterolemia, and elevated platelets and hemoglobin indicated the presence of hypercoagulability.
Several previous studies have reported the use of drug therapy for ventricular thrombosis. Vecchio et al. 11 reported that thrombolytic therapy with tissue fibrinogen kinase and antiplatelet therapy (aspirin) were not effective. The effectiveness of heparin treatment was uncertain, and there was also an increased risk of bleeding. Oral anticoagulants, such as warfarin, were significantly effective and reduced the risk of systemic embolism in patients with left ventricular dysfunction as well as thrombosis. 12 Notably, Calkins, et al. 13 reported that in the treatment of patients with nonvalvular atrial fibrillation, the curative and preventive effect of new oral anticoagulants against venous thromboembolism was similar to that of warfarin. Additionally, new oral anticoagulants, such as dabigatran, were associated with better medication adherence and a lower risk of clinically relevant bleeding compared with warfarin. Thus, it may be safer and more effective to choose dabigatran over warfarin, for anticoagulant therapy. A similar conclusion was confirmed in Schulman's study involving 2589 patients with acute venous thromboembolism. 14 Moreover, for arterial thrombi, dabigatran was found to be effective in dissolving left ventricular thrombi of different etiologies.15–18 In our case, after the left ventricular thrombus was found, the patient had severe symptoms and intermittent elevated BP caused by the pheochromocytoma, and we chose dabigatran as anticoagulation treatment. The patient’s relatively low body weight (48 kg) was another consideration. Therefore, we chose a proper dose of anticoagulant therapy over removing the thrombus surgically, and the effectiveness of treatment was confirmed during the postoperative follow-up.
Our report may be a helpful addition to the literature; pheochromocytoma recurrences are rare and should not be overlooked. We also report that using anticoagulation therapy to treat left ventricular thrombosis may be preferable to surgical thrombus removal in such cases, providing clinical evidence for diagnosis and treatment of catecholamine cardiomyopathy with left ventricular thrombosis in patients with recurrent pheochromocytoma.
Footnotes
Ethics statement
Ethical approval was sought from the Human Ethics Committee, Xinqiao Hospital, Third Military Medical University. The need for approval was waived by the ethics committee because this was a case report that involved only one case, and approval to use the clinical data was not required. Consent for treatment was obtained. The patient agreed to the use of her imaging and clinical data for publication and academic research and provided written informed consent. This report involved no risk to the patient’s privacy.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
Renzheng Chen and Yong Wang were co-lead authors of the paper and contributed equally. Jie Yang, Xiaofeng Cheng, Jiang Wang and Lan Huang critically revised the manuscript for important intellectual content and gave final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.