
Abstract
Pulmonary large cell neuroendocrine carcinoma (LCNEC), which accounts for approximately 1% of all lung cancers, is a rare and highly aggressive malignancy with a poor prognosis. Therefore, it is important to devise an effective treatment strategy. In the treatment of locally advanced complex LCNEC, it is unique to first administer radiotherapy combined with albumin-bound paclitaxel plus carboplatin, followed by durvalumab for immune maintenance treatment after concurrent radiotherapy and chemotherapy to achieve complete remission. We report a 54-year-old man who smoked and who felt chest tightness for 2 weeks and was diagnosed as having combined pulmonary LCNEC. For patients with locally advanced pulmonary LCNEC, chemoradiotherapy increases overall survival. After surgical resection and chemoradiotherapy, our patient achieved complete remission. Durvalumab was then started to consolidate the treatment. After six courses of immune maintenance therapy, the patient developed grade 2 immune-related pneumonitis and took prednisone orally until the symptoms resolved, and then reached complete remission again. The patient achieved complete remission, which was a challenge with this rare carcinoma, through albumin-bound paclitaxel plus platinum-based chemotherapy combined with radiotherapy and durvalumab for immune maintenance therapy. This approach may provide a treatment option for locally advanced combined pulmonary LCNEC.
Keywords
Introduction
Pulmonary LCNEC, which accounts for approximately 1% of all lung cancers, is a rare, highly aggressive, and difficult-to-treat malignancy. 1 LCNEC occurs more commonly in men who are heavy smokers and does not occur in non-smoking women. The symptoms of LCNEC are not obvious; hemoptysis, cough, and post-obstructive pneumonia are rare. Sometimes, patients present with asymptomatic nodules, night sweats, or chest pain. 2 LCNEC comprises a large number of diseases, which have been categorized by the 2015 World Health Organization (WHO) as four different and distinctive subtypes according to increasing biological aggressiveness: atypical carcinoid (AC), typical carcinoid (TC), lung LCNEC, and small cell lung cancer (SCLC). 3 LCNEC is both a neuroendocrine tumor and an non-small cell lung cancer (NSCLC) tumor. However, the biological, clinical, and prognostic characteristics of LCNEC in advanced stages resemble those of SCLC. 4 LCNEC is considered combined LCNEC 5 when it is accompanied by other lung cancer components, such as squamous cell carcinoma, adenocarcinoma, giant cell carcinoma, or spindle cell carcinoma. Few studies have described combined LCNEC and the particular features. However, we report a case of combined pulmonary LCNEC that was composed of 40% LCNEC, 50% invasive adenocarcinoma, and 10% SCLC, and we discuss a suitable treatment strategy for the management of this malignancy.
Case presentation
A 54-year-old man who smoked felt chest tightness for 2 weeks, essentially without any other symptoms. He had smoked approximately 20 cigarettes per day for over 30 years and drank alcohol occasionally. He had hypertension for more than 1 year, and on admission, his blood pressure measurement was 150/91 mmHg, and blood pressure was well controlled during hospitalization. There was no unusual family history. The patient also had a hard, poorly mobile, enlarged lymph node measuring approximately 1.5 cm in the left supraclavicular fossa. The other superficial lymph nodes were not palpable. Routine blood biochemical and tumor markers showed no abnormalities. Chest computed tomography (CT) revealed a nodule in the lingual segment of the left upper lung lobe, while positron emission tomography-CT (PET-CT) revealed increased glucose metabolism in the same area, and malignancy was considered, clinically (Figure 1a–c). PET-CT also revealed that multiple lymph nodes in the supraclavicular fossa, mediastinum, and left hilar region were enlarged, and glucose metabolism was increased; lymph node metastasis was considered. On 15 January 2020, left supraclavicular fossa lymph node biopsy was performed. The pathological results showed that one lymph node had adenocarcinoma metastasis, and lung origin was considered. Immunohistochemical results revealed the following: cytokeratin (CK)5/6 (−), p40 (−), napsin A (+), thyroid transcription factor-1 (TTF-1) (+), CK20 (−), CK7 (+), Ki-67 (+), programmed death-1 PD1 (−), programmed death ligand-1 (PD-L1) (+) and >50%, and villin (−). After thoracoscopic wedge-shaped resection of the left upper lung lobe on 17 January 2020, the pathological biopsy results (Figure 2a–d) on 21 January 2020 diagnosed combined LCNEC, which was composed of 40% LCNEC, 50% invasive adenocarcinoma, and 10% SCLC. Immunohistochemical results after surgery (Figure 3a–h) revealed the following: PD-L1 (+), cluster of differentiation (CD)56 (+), chromogranin A (CgA) (+), synaptophysin (Syn) (+), napsin A (+), TTF1 (+), CD4 (+), CD8 (+), CK5/6 (−), p40 (−), CK20 (−), and PD1 (−). No gene mutations were detected. This case was staged as cT1bN3M0 IIIB.

Imaging in the clinical diagnosis (a) Chest computed tomography (CT): nodules in the upper lobe and lingual segment of the left lung. (b) Chest CT: multiple lymph nodes in the mediastinum with partial enlargement. (c) Positron emission tomography-CT (PET-CT): the nodules in the upper left lung lobe and lingual segment showed increased glucose metabolism, and cancer was considered. Multiple lymph nodes in the supraclavicular fossa, mediastinum, and left hilar region were enlarged, glucose metabolism was increased, and lymph node metastasis was considered.
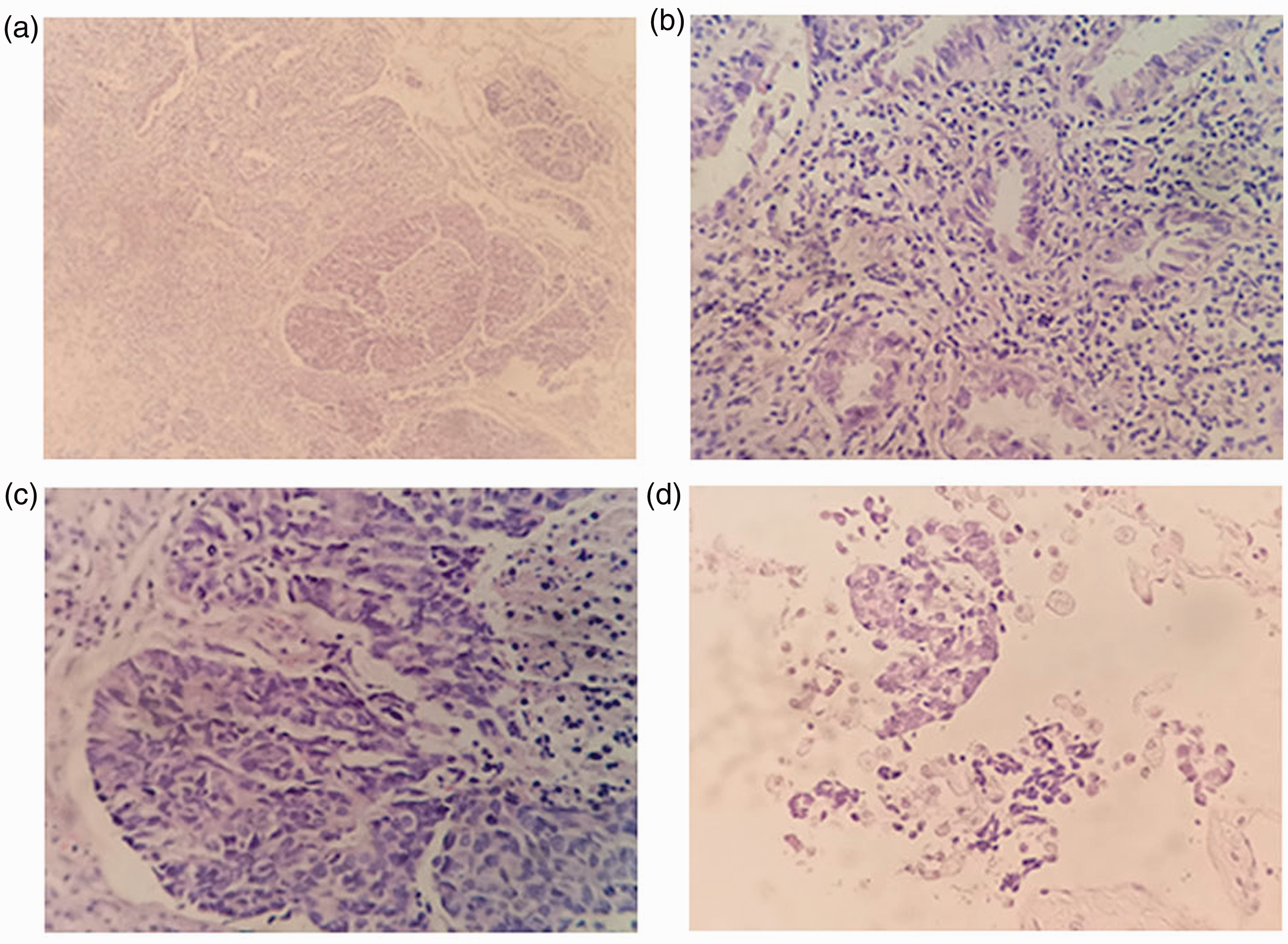
Postoperative pathological results (a) Combined large cell neuroendocrine carcinoma (LCNEC) composed mainly of LCNEC and invasive adenocarcinoma (hematoxylin and eosin (H&E) staining, × 100 magnification). (b) Invasive adenocarcinoma: 50% (H&E staining, × 400 magnification). (c) LCNEC: 40% (H&E staining, × 400 magnification). (d) Small cell carcinoma: 10% (H&E staining, × 400 magnification).

Immunohistochemical staining after surgery for (a) programmed death-ligand 1 (PD-L1), (b) cluster of differentiation (CD)56, (c) chromogranin A (CgA), (d) synaptophysin (Syn), (e) napsin A, (f) thyroid transcription factor (TTF)1, (g) CD4 (90%), and (h) CD8 (30%) was positive in the tumor cells (magnification × 400).
Regarding the treatment of this case, on 8 February 2020, we administered postoperative chemotherapy with albumin-bound paclitaxel and cisplatin (TP regimen). The patient received two courses of postoperative adjuvant chemotherapy (albumin-bound paclitaxel 260 mg/m2/day; cisplatin 75 mg/m2/day on day 1, q 3 weeks). Then, radiotherapy began on 24 February 2020 and continued to 30 April 2020, and the TP regimen (albumin-bound paclitaxel 100 mg/m2/day; cisplatin 25 mg/m2/day on days 1, 8, and 15) was used during radiotherapy. After concurrent radiotherapy and chemotherapy, the patient underwent repeat CT imaging, Combined with the current clinical manifestations at that time, findings indicated that the patient achieved complete remission on 11 May 2020 (Figure 4a). Immunotherapy was then started on 12 May 2020 to consolidate the treatment. The patient was treated with durvalumab (10 mg/kg, q 3 weeks). After six courses of immunotherapy, new and scattered nodules in both lungs were found on CT on 19 August 2020 (Figure 4b). Carcinoembryonic antigen concentrations did not exceed the normal range, and PET-CT examination results (Figure 4c) indicated that immune-related pneumonitis combined with radiation pneumonia was more likely, although metastasis was considered. Through the efforts of the multi-disciplinary treatment team comprising lung cancer specialists and using teleconsultation in the West China Hospital of Sichuan University, three possible situations were considered: progression, pseudoprogression, and immune-related pneumonitis, before pathological biopsy. A chest wall mass was found subsequently on CT, and foreign body granuloma was diagnosed by pathological biopsy.

Imaging changes during diagnosis and treatment (a) Chest computed tomography (CT) at the first complete remission. After resection of the tumor in the left upper lung lobe and lingual segment, increased soft tissue density nodules were found in bilateral hilar regions, aortic arch, anterior vena cava, aortic window, and carina, with the larger nodules measuring approximately 9 mm in the short diameter, with clear boundaries. Enhanced scan showing mild homogeneous enhancement. (b) Chest CT after the sixth immunotherapy treatment showing new segmental atelectasis in bilateral upper and lower lung lobes, increased areas of opacification and flocculent shadows, and changes after radiotherapy. (c) Positron emission tomography-CT (PET-CT) findings after the sixth immunotherapy therapy showing that both lungs contained scattered solid and sub-solid nodules, with some nodules showing increased glucose metabolism; therefore, the possibility of lung metastasis was considered. The subcutaneous soft tissue nodule near the left rib showed increased glucose metabolism, and the possibility of metastasis was considered. Multiple patchy and streaky shadows are seen in bilateral upper and lower lung lobes, with partial bronchiectasis and increased glucose metabolism. Combined with the history, the possibility of radiation pneumonia and bronchiectasis was considered. (d) Chest CT showing complete remission after treatment for immune-related pneumonitis. The images show that the radiation pneumonia has improved dramatically and that the number of pulmonary nodules also decreased dramatically.
After combining all the examination results and clinical manifestations, the diagnosis was immune-related pneumonitis with chest wall soft tissue inflammation. Durvalumab was stopped temporarily, and prednisone (1–2 mg/kg daily or equivalent) was given orally. After 2 months of prednisone treatment, the patient’s symptoms disappeared completely. Throughout treatment, the patient also had continuous hypothyroidism and continued to take thyroxine as replacement therapy. There were no other immunotoxic events. Two months after the symptoms of immune-related pneumonitis disappeared completely, complete remission was achieved again, as confirmed with CT on 18 January 2021 (Figure 4d). The patient continued to take durvalumab (10 mg/kg, q 4 weeks) for consolidation treatment from 20 January 2021, and he is being monitored to avoid recurrence of immune-related pneumonitis. During the treatment period of this case, the curative effect was evaluated every 2 months, and findings indicated complete remission; immune maintenance treatment has been continued.
All procedures involving the participation of human participants in this research conformed to the ethical standards of the agency and/or the National Research Council and the Helsinki Declaration (revised in 2013). The current study was approved by the Ethics Committee of the Second Neijiang People's Hospital. The patient provided written and verbal informed consent.
Discussion
Pulmonary LCNEC is a rare and highly aggressive malignancy with a poor prognosis. This cancer is more common in men who are heavy smokers, and it is essential to devise an effective treatment. The symptoms of LCNEC are not obvious; for example, the only symptom in this case was chest tightness. As a possible suspected etiology, carcinoid might cause coronary spasm, which could have resulted in the patient’s presenting chest pain. 6 LCNEC has been categorized by the 2015 World Health Organization (WHO) as four different and distinctive subtypes according to increasing biological aggressiveness, as noted earlier. This case was diagnosed as combined pulmonary LCNEC, which was composed of 40% LCNEC, 50% invasive adenocarcinoma, and 10% SCLC. We chose chemoradiotherapy instead of chemotherapy for this patient. Limonnik et al. 7 found that the median overall survival and the 1-, 3-, and 5-year overall survival of patients receiving chemoradiotherapy were longer than for patients receiving chemotherapy. The authors proposed that definitive chemoradiotherapy for patients with locally advanced pulmonary LCNEC was an independent predictor of increased overall survival. Currently, there is no standard treatment guideline for LCNEC, let alone combined LCNEC; treatment is inferred from the guidelines for NSCLC and SCLC. 8 Radiotherapy combined with albumin-bound paclitaxel plus carboplatin was used for the first time, in this special case, which was a relatively unique and effective treatment.
For early disease with an operable tumor, similar surgical treatment as that for NSCLC should be considered. In addition, a several studies have shown that adjuvant chemotherapy after surgical resection can improve the survival rate of early disease.9,10 In the guidelines of the American Society of Clinical Oncology (ASCO), the same regimen for NSCLC or platinum/etoposide chemotherapy is recommended for LCNEC, such as cisplatin combined with pemetrexed. 11 Similarly, a number of studies support using therapy as for SCLC in stage III or IV disease. However, more large cohort studies evaluating the biology of advanced neuroendocrine carcinoma are necessary, and these studies will help establish new treatments for LCNEC patients. 12 A European trial 13 of 29 patients treated with platinum-based/etoposide chemotherapy reported an overall response rate (ORR) of 34% and a progression-free survival (PFS) of 5.0 months (95% confidence interval (CI): 4.0–7.9 months). However, the efficacy of the cisplatin-etoposide combination in the treatment of advanced LCNEC is poor and similar to the response in patients with advanced SCLC. Likewise, Yamazaki et al. 14 performed a retrospective study of 20 patients with stage IIIA–IV LCNEC and concluded that the response rate of LCNEC to cisplatin-based chemotherapy was similar to that of SCLC. Therefore, the response of LCNEC to platinum-based chemotherapy can be similar to that of SCLC. Moreover, new and more extensive prospective trials ought to be encouraged to determine the chemotherapy methods for docetaxel, paclitaxel, gemcitabine, vinorelbine, or etoposide for the treatment of suspected pulmonary LCNEC. 15 For patients with advanced NSCLC, albumin-bound paclitaxel as a first-line therapy was effective and could significantly improve ORR versus solvent-based paclitaxel and achieve the primary end point. 16 Albumin-bound paclitaxel plus platinum-based chemotherapy was adopted for this case with 90% NSCLC and 10% SCLC.
After surgical resection and chemoradiotherapy in our patient, it was not easy to achieve complete remission even though the patient's neoplastic lesions were removed. However, no lesions or progression have been seen in CT imaging, and the patient's chest tightness symptoms were relieved significantly. In a previous study of the cell-free DNA (cfDNA) of an LCNEC patient, the most common gene mutations were tumor protein 53 (TP53); retinoblastoma (RB1); epithelial growth factor receptor (EGFR); anaplastic lymphoma kinase (ALK); Kelch-like ECH-associated protein (KEAP)1; neurofibromatosis type 1 (NF1); switch/sucrose non-fermentable (SWI/SNF)-related, matrix-associated, actin-dependent regulator of chromatin, subfamily A, member 4 (SMARCA4); and NOTCH1. 17 We did not detect any gene mutations in our case; therefore, we did not perform gene therapy even though gene therapy has a certain role in the treatment of such cases. One case of LCNEC with an EGFR mutation showed a response to EGFR-tyrosine kinase inhibitor (EGFR-TKI). The patient had an 8-month response to the EGFR-TKI, icotinib. 18
Subsequently, because of the PD-L1 (+) results of >50% in this case, durvalumab was used for consolidation therapy. Durvalumab is a selective, high-affinity monoclonal antibody against human immunoglobulin G1 (IgG1). Durvalumab can block the binding of PD-L1, PD-1, and CD80, and produce anti-tumor T cell activity. 19 The survival time of patients who receive durvalumab within 14 days after the end of chemoradiotherapy is longer than that of patients who receive durvalumab later, indicating that chemoradiotherapy has a positive effect on the efficacy of durvalumab. 20 For stage III NSCLC, the overall survival rate improved significantly with durvalumab maintenance therapy after radiotherapy and chemotherapy, and was especially prominent in the PD-L1 (+) subgroup (PD-L1 expression ≥1%). 20 In the PACIFIC study, Gray et al. 21 found that 48.2% of the patients died (44.1% in the durvalumab group and 56.5% in the placebo group). The overall survival rates in the placebo and durvalumab groups at 12, 24, and 36 months were 74.6% versus 83.1%, 55.3% versus 66.3%, and 43.5% versus 57.0%, respectively. The follow-up results of all examinations showed improvement, in accordance with previous analyses, which demonstrated the 3-year clinical benefits of durvalumab after chemoradiotherapy and further established the PACIFIC regimen as the standard of care for this population. However, Han et al. 2 proposed that even with positive PD-L1 expression, immunotherapy could be ineffective in some patients, and a possible factor was delayed immunotherapy.
After six courses of immune maintenance therapy in our case, CT identified new and scattered nodules in both lungs, suggesting progressive, pseudoprogressive, or immune-related pneumonitis. Carcinoembryonic antigen concentration did not exceed the normal range, and PET-CT examination results indicated that immune-related pneumonitis combined with radiation pneumonia was more likely, although metastasis was considered before pathological biopsy results. Another chest wall mass was found by CT, and foreign body granuloma was identified on pathological biopsy. Consultation was performed between the multi-disciplinary lung cancer treatment team and our hospital, and, combined with the results of the chest wall mass resection biopsy, immune-related pneumonitis with chest wall soft tissue inflammation was diagnosed. Durvalumab was stopped temporarily, and prednisone was taken orally for this case with grade 2 pneumonitis, which meant symptomatic, limiting the performance of activities of daily living, and intervention indicated. 22 Oral corticosteroids (prednisone or prednisolone, 1–2 mg/kg daily or equivalent) is recommended as the initial immunosuppressive therapy for grade 2 pneumonia. The patient's situation should be closely monitored, usually for at least 48 hours after the beginning of steroid treatment, and then once or twice a week. If the patient's clinical situation improves, steroids should be tapered slowly (over more than 4 to 6 weeks or longer) to minimize the risk of recurrent or flare pneumonia. 23
Limitations
Limitations exist in this study. First, we reported only one case, which was insufficient to further explore the overall survival, PFS, and other indices for this malignant disease. Second, this case was unique in that we achieved complete remission using chemoradiotherapy and immune maintenance therapy for this rare cancer. However, this is a new treatment protocol and an extrapolation of existing treatment, which could indicate a treatment for this rare malignancy, although this is not an internationally recognized standard therapeutic schedule.
Conclusion
Pulmonary LCNEC is a rare and highly aggressive malignancy without standard therapy. Our reported case is unique for this rare cancer, in that the patient achieved complete remission through albumin-bound paclitaxel plus platinum-based chemotherapy combined with radiotherapy and durvalumab as immune maintenance therapy. This approach could provide a treatment option for locally advanced combined pulmonary LCNEC.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211055387 - Supplemental material for Complete remission of combined pulmonary large cell neuroendocrine carcinoma: a case report
Supplemental material, sj-pdf-1-imr-10.1177_03000605211055387 for Complete remission of combined pulmonary large cell neuroendocrine carcinoma: a case report by Jian Xu, Qi Feng, Yong Chen, Xiu-lan Liu and Ou Jiang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211055387 - Supplemental material for Complete remission of combined pulmonary large cell neuroendocrine carcinoma: a case report
Supplemental material, sj-pdf-2-imr-10.1177_03000605211055387 for Complete remission of combined pulmonary large cell neuroendocrine carcinoma: a case report by Jian Xu, Qi Feng, Yong Chen, Xiu-lan Liu and Ou Jiang in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605211055387 - Supplemental material for Complete remission of combined pulmonary large cell neuroendocrine carcinoma: a case report
Supplemental material, sj-pdf-3-imr-10.1177_03000605211055387 for Complete remission of combined pulmonary large cell neuroendocrine carcinoma: a case report by Jian Xu, Qi Feng, Yong Chen, Xiu-lan Liu and Ou Jiang in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was supported by funding from a prospective, multi-center, multi-arm clinical study of albumin-bound paclitaxel combined with sintilimab in the treatment of patients with advanced non-small cell lung cancer (320.6750.2020-12-59).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.