
Abstract
Objective
New anti-cancer drugs promise to increased survival benefits and reduce adverse events. Trastuzumab emtansine (T-DM1) is a novel anti-human epidermal growth factor receptor 2 agent that has shown minimal cardiotoxicity in clinical trials. However, data on real-life outcomes are required.
Methods
A retrospective review of our center’s medical records was performed, including female patients aged ≥18 years with a diagnosis of metastatic breast cancer who were treated with T-DM1. Descriptive statistics were used to investigate clinical features that could increase the risk of cardiotoxicity. Cardiotoxicity was determined by comparing pre and post-T-DM1 echocardiogram results and was defined as a decrease in the left ventricular ejection fraction (LVEF) >10% to below 55%.
Results
Data from 41 female patients with a mean age of 52 ± 11.5 years were evaluated. A significant LVEF decrease (from 59% to 33%) was observed in one patient during T-DM1 treatment. Further investigation showed that this decrease was due to underlying coronary artery disease, and LVEF recovered to the baseline value after coronary revascularization.
Conclusion
T-DM1 seems to be safe in terms of cardiotoxicity. Real-life data with a larger sample size are still needed to confirm the cardiac safety of T-DM1.
Keywords
Introduction
As outcomes have improved in patients with human epidermal growth factor receptor 2-positive (HER2+) breast cancer, more attention has been directed to decreasing drug-related toxicity and to, thereby, increasing the patients’ quality of life. While HER2-targeted drugs play a significant role in reducing patients’ clinical symptoms, they can also cause serious adverse events. Cardiotoxicity is a severe side effect of anti-HER2 agents.1,2
Although the anti-HER2 agent-related cardiotoxicity pathway is not fully understood, it is different from anthracycline-associated cardiac dysfunction, which occurs after persistent structural changes in myocytes. Anti-HER2 drug-related cardiotoxicity is not dose-dependent, may not be encountered in all treated patients, and is reversible.3,4 This cardiotoxicity causes functional changes in cardiomyocytes by inhibiting the HER2 signaling pathway, which affects cell survival and cell growth and differentiation. 5 Therefore, cardiomyocytes recover after discontinuing HER2 targeted antibodies, which releases the suppression effect on HER2 signaling.
Trastuzumab, a prototype of this group, causes cardiotoxicity in up to 11.3% of breast cancer patients, although most (8.7%) have asymptomatic or mildly symptomatic left ventricular ejection fraction (LVEF) reduction. 6 However, novel HER2-targeted drugs are available, which may cause less cardiotoxicity.
Ado-trastuzumab emtansine (T-DM1) is a novel and promising anti-HER2 agent that provides benefits in progression-free and overall survival. 7 T-DM1 is a combination of trastuzumab, which is a HER2 antibody, and emtansine, which is an anti-microtubule agent. 8 First, T-DM1 binds to the HER2 ligand via trastuzumab and after endocytosis of the conjugate DM1, it separates and induces cellular apoptosis. Trastuzumab in the conjugate also affects intracellular pathways through inhibition of HER2 signaling, which causes cytotoxicity.8,9
Cardiac dysfunction is an effect of trastuzumab, but there are limited data about T-DM1-related cardiotoxicity, especially in real-life clinical patients. Therefore, the aim of this study was to retrospectively analyze the cardiac safety results from a single-center cohort comprising patients with HER2+ breast cancer who received T-DM1.
Patients and methods
Medical records were reviewed to identify female patients aged ≥18 years with a diagnosis of HER2+ metastatic breast cancer who had been treated with T-DM1 between October 2016 and October 2020. Patients who underwent regular transthoracic echocardiography (TTE) as part of their follow-up examinations at our medical center were enrolled into the study. Patients were excluded from the study if they had not regularly attended follow-up examinations or had not undergone serial echocardiographic examinations at our hospital. All patients had been given T-DM1 (3.6 mg/kg) once every 21 days until disease progression. It is recommended that cardiac function be monitored at baseline and during the 3 to 12 months of anti-HER2 treatment as well as after this period if cardiac symptoms are encountered. 10
Baseline clinical characteristics, comorbidities, previous therapies (radiotherapy, mastectomy, and medications), two-dimensional (2D) conventional TTE examinations, and cardiac symptoms, if any, were evaluated. Data were collected until 1 year of T-DM1 administration was completed or until the T-DM1 administration was stopped. Each 2D TTE result during that period was analyzed, and the LVEF results were grouped as ≥55% or below 55%. The LVEF had been calculated using a modified Simpson method on the basis of 2D TTE images. 11 In accordance with the European Society of Cardiology (ESC) criteria, cardiotoxicity was defined as a decrease in LVEF >10% to below 55%. 12 The primary outcome of this study was T-DM1-related deterioration in LVEF resulting in a value <55%.
Statistical analysis
Descriptive statistics were used to present the patient characteristics. Variables with a normal distribution were presented as the mean ± standard deviation, and variables that did not show a normal distribution were reported as the median (interquartile range). Categorical variables were summarized as the number (n) and percentage (%).
Approval for this retrospective study was granted by the Institutional Ethics Committee (approval code: 10942, date: 24 March 2020). The reporting of this study conforms to STROBE guidelines. 13 The requirement for patient consent was waived by the ethics committee because this retrospective study was conducted at a training university hospital, in which patient records can be used for scientific purposes if the patients’ privacy is respected.
Results
Eighty patients who were treated with T-DM1 between 2016 and 2020 were identified. Thirty-nine patients were excluded because of irregular control visits, discontinued follow-up by the patient, or death, which resulted in a lack of follow-up echocardiographic examinations (Figure 1). The results from 41 patients who met the inclusion criteria were evaluated. The 41 women had a mean age of 52 ± 11.45 years (range, 32 to 72 years) and comprised 46.3% who were postmenopausal, 7.3% who were peri-menopausal, and 46.3% who were premenopausal. Thirteen patients (31.7%) were ≥60 years old and six (14.6%) patients were ≥65 years old. The median number of T-DM1 cycles was 12 (13). At baseline, the median LVEF value was >55%.

Flow diagram for patient enrollment.
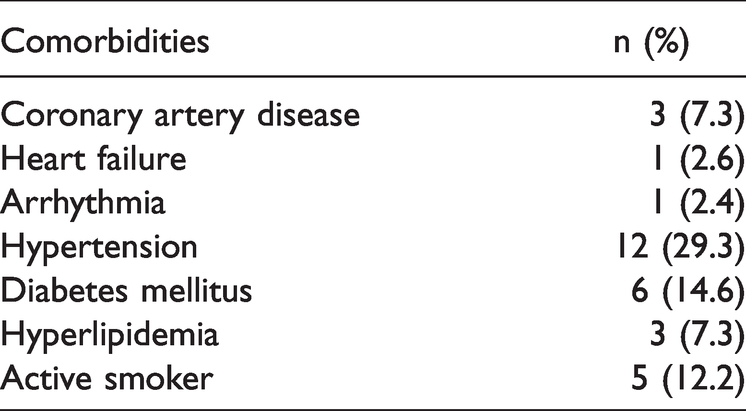
Baseline clinical characteristics are presented in Table 1. Additionally, at baseline, one patient had moderate to severe aortic stenosis, and one patient had a history of atrial septal defect repair, chronic atrial fibrillation, and severe mitral and tricuspid regurgitation.
Baseline clinical characteristics of the participants.
Mastectomy had been performed in 35 (85.4%) patients, and 14 (34.1%) patients had received radiotherapy on the left breast. Anthracycline had been previously administered to 25 (61%) patients and all patients except for one had used trastuzumab during the metastatic period before T-DM1 treatment. In three (7.3%) patients, there was a history of trastuzumab-related cardiotoxicity (TRC), from which they had fully recovered. All three patients had no baseline cardiovascular risk factors.
The first patient with a history of TRC was also the only patient with a baseline LVEF <55% in the study. She was 51 years old and her LVEF had decreased to 48% under previous trastuzumab treatment. After discontinuing the drug, her LVEF had increased to more than 55%. Trastuzumab was administered again and her LVEF decreased to 50%. Despite this reduction, trastuzumab was continued, and because of progressive disease, the treatment was changed from trastuzumab thereafter. Thus, her baseline LVEF was 50% at the beginning of T-DM1 treatment, and it did not decrease in response to T-DM1 therapy.
The second patient with a history of TRC was 48 years old and had a decrease in LVEF from 65% to 55% in response to trastuzumab. Thereafter, the drug had been discontinued, and the LVEF value increased to baseline. After re-administering trastuzumab, the patient’s LVEF decreased to 52%, and drug administration was stopped. After stopping trastuzumab, her LVEF increased to 60% before starting T-DM1 treatment, and it did not decrease in response to T-DM1.
The last patient with a history of TRC was 42 years old and had a LVEF that had decreased to 48% after trastuzumab. After discontinuing trastuzumab, the patient’s LVEF increased to 60%, and trastuzumab was initiated again. However, because of progressive metastatic involvement, the treatment was changed. At the beginning of the T-DM1 treatment, her LVEF value was normal, and it did not decrease in response to T-DM1 therapy.
The other previous therapies that were administered to patients in the study population are listed in Table 2.
Previous breast cancer therapies that were administered to the patients.

LHRH, Luteinizing hormone-releasing hormone.
T-DM1 was discontinued in one patient (2.4%) who developed a decrease in LVEF from 60% to 33% at 5 months after initiation of T-DM1 therapy. The cause was determined not to be cardiotoxicity, but rather, it was due to coronary artery disease. That patient was 72 years old and had hypertension, diabetes mellitus, hyperlipidemia, and was an active smoker. Cardiac examination results revealed obstructive coronary artery disease. After revascularization and initiation of heart failure treatment, the LVEF increased to over 55% at month 3 after surgery.
Only four of the 80 patients whose records were investigated died while receiving T-DM1 treatment. Among these four patients, none of them died because of cardiac failure. The causes of death were hepatic coma, acute renal failure, progressive neuronal involvement, and pulmonary insufficiency.
Discussion
To the best of our knowledge, this is one of the few case series to evaluate the cardiotoxicity of T-DM1 therapy in real-life clinical settings. The results showed that none of the 41 patients had a decrease in their LVEF from T-DM1 therapy. On the basis of these results, T-DM1 seems to have favorable outcomes in terms of adverse cardiac events and can be safely administered, even to patients who have baseline clinical risk factors or previous therapies that could increase the risk of cardiotoxicity.
Pondé et al. performed a pooled analysis of T-DM1 studies in HER2+ breast cancer patients to investigate outcomes regarding cardiac safety. 14 Data from 1961 patients were analyzed, and a decrease in the LVEF was detected in 2.75% of the patients. Moreover, cardiac ischemia was reported with a prevalence of 0.1% and cardiac arrhythmia was detected in 0.71% of the patients. The most striking point was that multivariate analyses showed that patient age ≥65 years (odds ratio [OR] 3.0; 95% confidence interval [CI], 1.77–5.14; p < 0.001) and baseline LVEF <55% (OR 2.62; 95% CI, 1.29–5.32; p = 0.008) were correlated with an increased risk of cardiotoxicity. Moreover, univariate analyses revealed that patients who experienced adverse cardiac events more frequently had hypertension. Finally, they concluded that T-DM1-related cardiotoxicity was reversible with a low incidence and a mild negative effect on left ventricular function, which rarely led to drug discontinuation. This pooled analysis comprised seven multi-center phase 2 or phase 3 trials, which means that the study population was highly selected and may have been healthier than real-life patients with breast cancer in out-patient clinics. When evaluating the above-mentioned studies, it should be kept in mind that the period of LVEF evaluation, concomitant or previous anti-cancer therapies, enrolled patients, and the accepted definition of cardiotoxicity may differ across studies.
Regardless of its limitations, this analysis provides important clues about the risk factors for T-DM1 cardiac adverse effects. Although 29.3% of the current study population had hypertension and 14.6% were ≥65 years old, no T-DM1-related cardiotoxicity was observed. Moreover, although there was one patient with a baseline LVEF of 50%, this patient was safely administered T-DM1, and no further decrease in the LVEF was observed. Additionally, the current cohort had risk factors such as coronary artery disease (7.3%), left ventricular hypertrophy (17.1%), diabetes mellitus (14.6%), hyperlipidemia (7.3%), active smoking (12.2%), and previous anthracycline treatment (61%), all of which are listed in the ESC guidelines as factors that increase the risk of anti-cancer therapy-related cardiotoxicity. 12
Real-life data from Michalaki et al. showed the cardiac outcomes of 36 patients who had received T-DM1. 15 No change was reported in the LVEF, but there was a significant decrease in the longitudinal and radial strain and strain rate after nine cycles of T-DM1, which indicated the clinical usefulness of speckle-tracking echocardiography in the early detection of cardiac dysfunction. Unfortunately, the speckle-tracking echocardiography records for the current study population were not available, so a strain analysis could not be performed. It would be better to compare pre- and post-T-DM1 strain values. Coppola et al. showed that anti-neoplastic-related cardiac dysfunction can be detected early by 2D strain echocardiographic imaging in mice. They concluded that the left ventricular systolic strain was decreased followed by a decrease in the LVEF. 16 Rea et al. also showed similar findings in their study that was conducted in mice, and they indicated that strain values can be used to determine drug-related cardiotoxicity earlier than conventional 2D LVEF measurements. They suggested that strain imaging could be used to detect subtle cardiac impairment. 17
It is noteworthy, however, that, owing to the potential cardiotoxic effects of T-DM1, the European Medicines Agency recommends routine evaluation of cardiac function before drug administration and at regular intervals during therapy. It is recommended that the T-DM1 treatment is discontinued if the LVEF decreases to <40% or declines to 40% to 45% with a ≥10% decrease from the pretreatment value. If T-DM1 is discontinued, echocardiography should be repeated within 3 weeks, and T-DM1 should not be initiated until the LVEF becomes sufficient. 18
Although, De Lorenzo et al. reported that T-DM1 had more of a cardiotoxic effect on murine hearts than trastuzumab and pertuzumab, there are no supporting data about the increased T-DM1 cardiotoxicity risk in humans. 19 Recent studies have shown that T-DM1 has been discontinued in a few patients because of cardiotoxicity.7,20–22 Only one patient required T-DM1 discontinuation in the current study population, which is consistent with the previous data, although the discontinuation in our study was not because of drug-related cardiotoxicity but because of an atherosclerosis-related decrease in the LVEF.
This study had some limitations. First, this was a retrospective study with a relatively small sample size. Second, the follow-up period was limited to the first year of T-DM1 therapy. Finally, strain echocardiography results were not available.
Conclusion
The results of this retrospective study provide preliminary real-life data about the cardiac safety of T-DM1, which is a novel and promising agent to treat breast cancer. T-DM1 showed no overt cardiotoxicity, and it did not cause therapy discontinuation due to cardiotoxicity even in patients with potential high risk factors. Further trials are needed with a larger sample size and a longer follow-up period, and novel sensitive echocardiographic measurements should be included to confirm the cardiac safety of T-DM1.
Footnotes
Contributing authors
Conception: A.A., A.S., A.T.S., S.D., I.H.M., O.O.; Design: A.A., M.Y., S.D., O.O.; Supervision: A.S., A.T.S., S.D., I.H.M., O.O.; Materials: A.S., M.Y., A.T.S.; Data collection and processing: A.A., A.S., M.Y., A.T.S.; Analysis and interpretation: A.A., M.Y., S.D., I.H.M.; Literature review: A.S., A.T.S., I.H.M.; Writer: A.A., M.Y., O.O.; Critical review: S.D., I.H.M., O.O.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.