
Abstract
Coronary artery aneurysms, rare lesions of Kawasaki disease (KD) and coronary atherosclerosis, are associated with severe cardiac complications. We herein describe an interesting case of coronary artery aneurysms due to exertional angina with possible underlying KD. A 26-year-old man without traditional risk factors for atherosclerosis presented with exertional chest pain and a positive exercise electrocardiogram stress test. Coronary angiography revealed total obstruction of the right coronary artery at the proximal portion, and the proximal left anterior descending artery contained a large spherical cavity filled with contrast agent; thus, the diagnosis of coronary artery aneurysms was confirmed. This was a typical coronary lesion suggestive of KD, and coronary artery bypass grafting was recommended. The diagnosis of KD may be ignored or missed in childhood, and significant cardiovascular damage may remain silent until adulthood, when severe coronary artery stenosis or thrombosis results in angina or acute myocardial infarction. Thus, to promote timely treatment and reduce morbidity and mortality, antecedent KD should be considered in the presence of angina pectoris or acute myocardial infarction in young patients without traditional risk factors for atherosclerosis.
Keywords
Introduction
Coronary artery aneurysms (CAAs) are relatively uncommon disorders, with a prevalence ranging from 0.3% to 5.3% in patients who are referred for coronary angiography. 1 Atherosclerotic aneurysms are more likely to occur in older patients with traditional risk factors. In children and adolescents, Kawasaki disease (KD) is the primary cause of CAA. 2 However, the diagnosis of KD is usually ignored or missed in childhood, and significant cardiovascular damage may remain silent until adulthood, when severe coronary artery stenosis or thrombosis results in angina or acute myocardial infarction.3,4 Thus, to promote timely treatment and reduce morbidity and mortality, antecedent KD should be considered in young patients with angina or acute myocardial infarction without traditional risk factors for atherosclerosis. We herein present an interesting case of a 26-year-old man with a history of exertional angina and possible underlying KD.
Case report
A 26-year-old man presented to our cardiology clinic with a history of exertional angina. He had recently experienced frequent bouts of laborious angina pectoris, especially when performing light physical activities. A resting electrocardiogram (ECG) revealed T-wave inversion in lead III and flat T waves in leads aVF and V1 (Figure 1(a)). An exercise ECG stress test and transthoracic echocardiography were performed. No abnormality was found on echocardiography, but the stress test was positive (Figure 1(b)–(d)) with depressed ST segments in leads I, II, aVL, and V2 to V5 and elevated ST segments in leads III, aVF, aVR, and V1 (Figure 1(c)). The patient was then admitted to our cardiovascular department for diagnostic coronary angiography (CAG). No conclusive findings were obtained from his medical history or physical examination. Upon admission to our department, his heart rate was 80 beats/minute and blood pressure was 125/80 mmHg. The serum cardiac high-sensitivity troponin T level was 0.031 ng/mL (normal value, <0.014 ng/mL), creatine kinase level was 198 U/L (normal value, <310 U/L), creatine kinase–muscle/brain level was 13 U/L (normal value, <24 U/L), triglyceride level was 1 mmol/L (normal value, 0.56–1.47 mmol/L), and low-density lipoprotein level was 1.43 mmol/L (normal value, 2.07–3.1 mmol/L). The subsequent diagnostic CAG showed total obstruction of the right coronary artery (RCA) at the proximal portion (Figure 2(a), (b)). The proximal left anterior descending artery (LAD) had a large spherical cavity filled with contrast agent (Figure 2(c); thus, the diagnosis of CAA was confirmed).

Representative images of a 26-year-old man who presented to the First Affiliated Hospital of Xi’an Jiaotong University with a history of exertional angina. (a) Electrocardiogram (ECG) on admission revealed T-wave inversion in lead III and flat T waves in leads aVF and V1 (black arrowhead). (b) Before exercise, the ECG revealed inverted T waves (red arrowhead) in lead V1 and flat T waves (red arrowhead) in lead III. (c) During exercise, the ECG revealed depressed ST segments in leads I, II, aVL, and V2 to V5 (red arrowhead) and elevated segments in leads III, aVF, aVR, and V1 and (d) At 1 minute 50 seconds after exercise, the ECG revealed sustained depressed ST segments in leads I, II, aVL, and V2 to V5 (red arrowhead) and elevated segments in leads III, aVF, aVR, and V1 (yellow arrowhead).
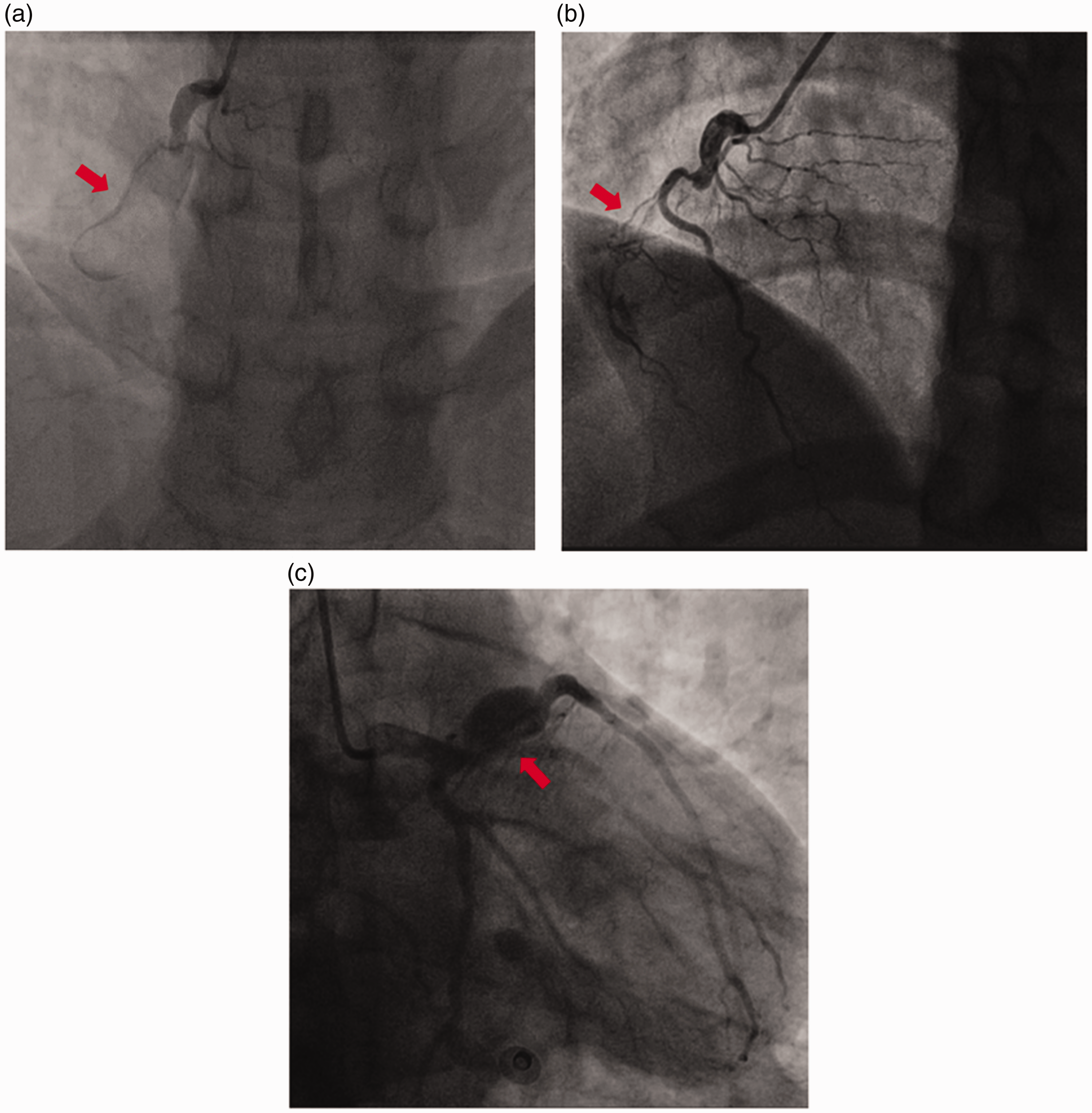
Representative images of a 26-year-old man who presented to the First Affiliated Hospital of Xi’an Jiaotong University with a history of exertional angina. (a) Coronary angiography revealed total occlusion at the proximal portion of the right coronary artery (red arrowhead), (b) total occlusion at the proximal portion of the right coronary artery with a large aneurysm shadow (red arrowhead), and (c) opening of the proximal left anterior descending artery into a large spherical cavity filled with contrast medium with slow opacification of the distal portion of the artery (red arrowhead).
The serum levels of antinuclear antibody, C3, C4, C-reactive protein, antistreptolysin O, rheumatoid factor, antineutrophil cytoplasmic antibody and the erythrocyte sedimentation rate were inconclusive. These findings did not support active vasculitis, rheumatic or immunologic diseases. Based on the typical coronary lesion, we speculated that the patient’s CAAs had probably originated from KD. Coronary artery bypass grafting was recommended because of the aneurysm-induced occlusion of the RCA and intra-aneurysm stenosis at the LAD, multi-lead ST changes exceeding the single-vessel territory on the exercise ECG, and risk of rupture and occlusion of the LAD aneurysm.
This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University. The patient provided written informed consent.
Discussion
CAAs are diffuse or localized dilatations of a single or multiple coronary arteries with >150% dilation of the largest coronary segment and saccular or spherical dilation. 5 The most frequently affected coronary artery is the RCA, followed by the proximal portion of the LAD and left circumflex artery. 6 Atherosclerosis is the essential cause of CAA in adults with traditional risk factors, whereas in adolescents, KD is the primary cause of coronary artery anomalies. 7 KD can be difficult to identify, and some cases go undiagnosed. Approximately 25% of children with untreated KD will develop CAA. As children with KD-induced CAA grow older, the risk of acute ischemic events increases.8,9 In the present case, the characteristics of the patient’s disorder were consistent with a CAA originating from KD. 10
CAG is the gold standard for the diagnosis of CAA and can provide the number, size, and location of the aneurysms. CAA can also be detected by magnetic resonance imaging, computed tomography, and transesophageal echocardiography. 5 If we had initially suspected KD upon presentation of our patient, we would have reminded an echocardiographic examination to check the proximal coronary artery, and the diagnosis might have been made earlier. Unfortunately, we did not initially suspect a CAA. This case illustrates that CAA should be considered in young patients with angina or acute myocardial infarction without traditional risk factors for atherosclerosis. The standard management protocol for patients with CAA is not well established. The management options for these patients include percutaneous stenting with covered stents, medical management with antithrombotic therapy, and surgical therapy. 11 Our patient experienced exertional chest pain and low exercise capacity. Coronary artery bypass grafting with CAA resection was considered because of the aneurysm-induced occlusion of the RCA and intra-aneurysm stenosis at the LAD, multi-lead ST changes exceeding the single-vessel territory on the exercise ECG, and risk of rupture, thrombosis, and occlusion of the LAD aneurysm. Fortunately, our patient did not develop myocardial infarction, which could have occurred secondary to the chronic occlusion of the RCA and the collateral formation.
Understandably, many cardiologists have little or no knowledge of the complications of KD vasculopathy treatment. A diagnosis of KD may be missed in approximately 5% of young adults evaluated for myocardial ischemia by angiography. 4 Thus, increased awareness of the cardiovascular sequelae of KD and their accompanying distinct treatment challenges are important. The CAG findings in this young patient revealed two coronary arteries with typical CAAs (the totally occluded RCA and a large spherical cavity of the LAD) without any coronary risk factors. These results suggest that the coronary lesions may have originated from KD. However, with the limited history of febrile illness of this patient, the coronary lesions may have also been related to many conditions other than KD despite the typical coronary artery anomalies seen on CAG.
In conclusion, the diagnosis of KD may be ignored or missed in childhood, and significant cardiovascular damage may remain silent until adulthood. Thus, to promote timely treatment and reduce morbidity and mortality, antecedent KD should be considered in the presence of angina pectoris or acute myocardial infarction in young patients without traditional risk factors for atherosclerosis.
Footnotes
Acknowledgment
Xiqiang Wang is grateful to the China Scholarship Council for providing a PhD fellowship (No: 201806280213).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
Xiqiang Wang received a PhD fellowship from the China Scholarship Council (No: 201806280213).