
Abstract
Hyperparathyroidism-induced hypercalcemic crisis is a rare presentation of primary hyperparathyroidism. Primary hyperparathyroidism is caused by uncontrolled and immoderate secretion of parathyroid hormone. The most common presentation in primary hyperparathyroidism is renal stones, soft tissue calcification, cystic bone disease, and even hypercalcemic crisis. We report a patient who presented with multiple organ dysfunction syndrome due to extreme hypercalcemia (serum calcium concentration, 4.79 mmol/L [2.15–2.25 mmol/L]) resulting from primary hyperparathyroidism (serum parathyroid hormone concentration, 2215 pg/mL). The complications in this patient were complete cardiac damage and acute kidney injury. On the basis of the hypercalcemic crisis, the patient subsequently underwent surgical resection of parathyroid adenoma. Two days after surgery, her serum calcium and parathyroid hormone concentrations were normal. The patient had a good recovery after a series of other relevant therapies. In conclusion, surgery should be taken into consideration for hyperparathyroidism.
Keywords
Introduction
Primary hyperparathyroidism (PHPT) is a common endocrine disorder. The incidence of PHPT is estimated to be 20/100,000 and more than 80% of cases are asymptomatic in the early stage. 1 Approximately 85% of PHPT is caused by a single parathyroid adenoma, multiple adenomas, or four-gland hyperplasia (15%), and is rarely caused by parathyroid carcinoma (<1%). 2 The pathogenesis of PHPT is unclear in most patients. The CCND1 and MEN1 genes contribute to the development of PHPT. Somatic mutations in MEN1 occur in 12% to 35% of sporadic adenomas, whereas rearrangement or overexpression of CCND1 can occur in 20% to 40%.3,4 In PHPT, there is loss of normal feedback suppression of serum calcium concentrations on the synthesis and secretion of parathyroid hormone (PTH). 5 This occurs because of an increased parathyroid cell mass and a reduction in the number of calcium-sensing receptor proteins in parathyroid cells. As a result, increased calcium concentrations are required to suppress PTH concentrations.
When assessing PHPT, PTH concentrations should be measured with an intact second-generation PTH assay or a third-generation assay. 6 The treatment for PHPT includes surgery and non-surgical monitoring and management. Parathyroidectomy remains the only cure for PHPT and is recommended in all symptomatic patients. Unfortunately, no currently available single drug can treat PHPT. 7
Hyperparathyroidism-induced hypercalcemic crisis (HIHC) is a rare, but life-threatening, symptom of PHPT. The course of this disease can be complicated by multiple concurrent comorbidities, including acute kidney injury, cardiac arrhythmias, severe hypovolemic shock, and various gastrointestinal disorders.8,9 Despite these challenges, patients with HIHC can be successfully treated with intensive medical support and emergent parathyroidectomy, and they have a good recovery. Severe PHPT is a rare condition. We report a patient who presented with multiple organ dysfunction syndrome due to extreme hypercalcemia resulting from PHPT. We present the following article in accordance with the CARE guideline checklist.
Case presentation
A 43-year-old woman presented to the emergency room following 2 weeks of severe subxiphoid pain and sudden oliguria for 2 days. The initial symptoms of the patient consisted of sudden onset of epigastric pain, especially in the subxiphoid area, followed by weakness, bloating, nausea, and vomiting. These symptoms became aggravated without medical treatment and the patient was admitted to the medical intensive care unit in a conscious state. She had no prior medical history of diabetes, hypertension, cerebrovascular disease, hypercalcemia, or cardiovascular disease. Her temperature, heart rate, respiratory rate, and blood pressure were normal. There was neither abnormal lung sounds nor cardiac murmur on a physical examination.
Before being admitted to our hospital, her initial laboratory examination results were remarkable, including an elevation in serum concentrations of calcium (5.5 mmol/L, normal value: 2.15–2.25 mmol/L), uric acid (773.7 μmol/L, 90–450 μmol/L), creatinine (323 μmol, 46–92 μmol), and troponin I (26.4, ng/mL, 0–0.034 ng/L). The patient was instantly transferred to our medical intensive care unit because of the hypercalcemic crisis, accompanied by myocardial damage and acute kidney injury. The patient completed a series of laboratory evaluations. A blood test showed a white blood cell count of 34.82 × 109/L (3.5–9.5 × 109/L) (89.5% neutrophils) and a platelet count of 449 × 109/L (125–350 × 109/L). The acute kidney injury was indicated by a urea concentration of 649 μmol/L (90–450 μmol/L) and a creatinine concentration of 203.7 μmol (46–92 μmol). The representative diagnostic markers of myocardial damage were as follows: troponin І concentration, 24.79 ng/mL; creatine kinase isoenzyme concentration, 66.10 ng/mL (0–2.02 ng/mL); myohemoglobin concentration, 8025 ng/mL (0–61.5 ng/mL); glutamic-oxalacetic transaminase concentration, 305 µL (14–36 µL); circulating myocardial microRNA (from an infarcted heart), 58,000 pg/mL (0–125 pg/mL), serum calcium concentration, 4.79 mmol/L (2.15–2.25 mmol/L), and serum PTH concentration, 2215 pg/mL (15–65 pg/mL).
Computed tomography showed small stones in both kidneys, sporadic inflammation of the lungs, and a 22 × 27-mm mass in the right neck near the right thyroid gland (Figure 1). Electrocardiography showed nodal tachycardia with a ventricular premature beat, and T wave changes with subendocardial myocardial infarction. The patient was advised to have myocardial enzymes tested. B-mode ultrasound showed an 18 × 15×11-mm mass, with an obscure boundary and morphological irregularity.

Neck computed tomography scan. (a) Neck computed tomography shows a mass in the arterial phase. (b) Neck computed tomography shows a mass in the venous phase. The red arrows indicate a parathyroid tumor.
On the basis of her clinical manifestations combined with biochemical parameters, she was diagnosed with myocardial damage, renal injury, shock, hypercalcemia, and PHPT. Her shock was emergently treated with aggressive intravenous fluid resuscitation, and medical dopamine and noradrenaline were used to elevate her blood pressure. She was also administered milrinone to strengthen her heart rhythm and phosphagen to nourish the myocardium. Her hypercalcemia was treated with calcitonin, bisphosphonates, glucocorticoids, furosemide, and continuous renal replacement therapy via a temporary venous catheter. However, her serum calcium concentrations remained high. She subsequently agreed to having parathyroid exploration and right parathyroidectomy after a discussion with her relatives regarding her cardiovascular and renal disorders along with multiple organ dysfunction syndrome. The patient was intubated in the operating room and a 30 × 20-mm hyperplastic parathyroid mass on the inferior aspect of the right thyroid lobe was excised during the surgery (Figure 2a). The gland was brittle and contained an irregular boundary. The tumor was dissected free from surrounding edematous tissues with difficulty. The diagnosis of right parathyroid adenoma was confirmed by a histopathological examination (Figure 2b, c, d). After the operation, the patient was immediately admitted to the intensive care unit and treated with mechanical assistance, sedation and analgesia, myocardial nutrients, anti-inflammatory medication, and nutritional support.

(a) In a resected specimen, a 30 × 20-mm parathyroid mass can be seen after excision. Histopathology of the right parathyroid adenoma at magnifications of (b) ×100, (c) × 200, and (d) × 400.
PTH and serum calcium concentrations were measured on the second day after surgery. The PTH baseline concentration of 2215 pg/ml was decreased to 66 pg/mL and the serum calcium concentration was decreased from 4.79 mmol/L to 2.66 mmol/L following resection of the parathyroid adenoma. A pathological examination of the gland identified some features of malignancy, with proliferating small round cells, including partly capsular invasion to adipose tissue, nested cells, and abundant sinusoids. The tumor was classified as an atypical parathyroid adenoma.
In the postoperative period, serum PTH and calcium concentrations rapidly decreased (Figure 3), and the patient gradually recovered over the next week. The patient was discharged 3 weeks after surgery.
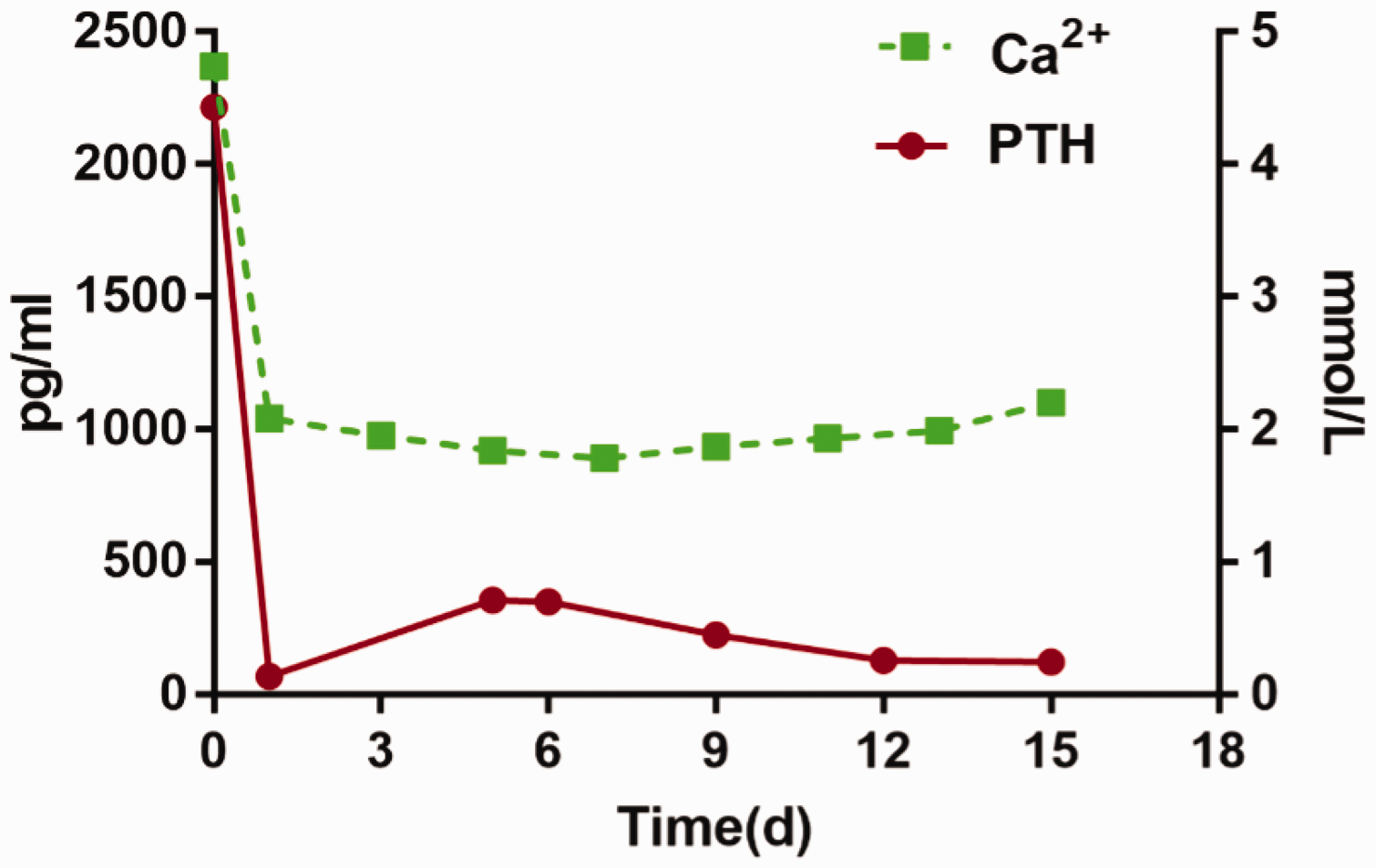
Time course of parathyroid hormone and calcium concentrations after the operation Ca, calcium; PTH, parathyroid hormone; d, days.
Discussion
PHPT and malignancy are the primary cause of hypercalcemia.10,11 The most common cause of PHPT is parathyroid gland adenomas (80%–85%), while carcinoma, parathyroid hyperplasia, parathyroid cyst, and multiple endocrine neoplasia types 1 and 2A are rare pathogeneses. 12 The symptoms of PHPT are initially mild or asymptomatic, followed by bone, neuromuscular, digestive, and kidney symptoms. Despite the various clinical manifestations of PHPT, hypercalcemia is the most common symptom in clinical cases.
Some studies provided an unclear definition of hypercalcemic crisis as a serum calcium concentration >3.5 mmol/L, accompanied by signs and symptoms.13,14 A hypercalcemic crisis was first described in 1939 by Hanes, and is considered as an endocrine emergency and fatal in the absence of optimal treatment. 15 Patients with hypercalcemia due to PHPT show changes in cardiac physiology and structure, including diastolic dysfunction, cardiac and vascular calcification, and left ventricular hypertrophy. 16
In a study of 67 patients with HIHC, only two patients suffered from cardiac arrhythmias. 8 However, severe cardiac arrhythmias are complications of hypercalcemic crisis. Three mechanisms are involved in the development of hypercalcemia-induced acute heart failure. One mechanism is intracellular hypercalcemia, which can impair myocardial repolarization coupling and reduce diastolic relaxation capacity, contributing to the development of heart failure. 17 Another mechanism is that accumulation of calcium can promote myocardial contraction band necrosis, which is characterized by excessive contraction of myofibrils and subsequent myocytolysis. 18 Additionally, catecholamines can markedly increase intracellular calcium concentrations, 18 consequently contributing to hemodynamic instability.
The acute effects of PHPT on renal function are not well understood. Moreover, non-oliguric acute kidney injury caused by refractory hypercalcemia requires emergent hemodialysis. Measuring concentrations of serum calcium and PTH is important for an early diagnosis, estimating disease severity, and treatment. When patients with acute cardiac damage and acute kidney injury have no obvious causes and elevated serum calcium concentrations are observed, PHPT-induced cardiac damage should be suspected. The treatment of hypercalcemia includes forced diuresis, bisphosphonates, oral phosphates, hydration with saline, calcitonin, glucocorticoids, and dialysis. Patients with sudden oliguria should be immediately treated with CRRT.
Imaging techniques help surgeons to locate adenomas and target the appropriate surgical area in PHPT. 9 Unfortunately, our patient who was treated with invasive respiratory support therapy was instantly transferred to the medical intensive care unit without Tc 99m-sestamibi scintigraphy. She had surgery performed after supportive treatment. After surgery, her serum calcium concentrations were greatly decreased, respiratory support was stopped, myocardial injury indicators gradually decreased, and her renal function gradually recovered. The patient was satisfied because the surgery and treatment saved her life. Our findings suggest that when patients with similar symptoms to those found in our patient are encountered in the clinical setting, the possibility of PHPT should be considered.
Footnotes
Ethics statement
The reporting of this study conforms to the CARE guidelines. 19 Detailed patient information has been de-identified. The study protocol was approved by the ethics review committee of Northern Jiangsu People’s Hospital. The patient provided consent for the treatment. Written informed consent was obtained from the patient for publication of this case report and the accompanying images.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.