
Abstract
Objective
To compare the clinical value of transcranial Doppler (TCD) ultrasound and computed tomography angiography (CTA) for diagnosing ischemic cerebrovascular disease.
Methods
A retrospective clinical study was conducted in 142 patients with ischemic cerebrovascular disease who were initially diagnosed by digital subtraction angiography. Under the single-blind condition, the patients were diagnosed by using TCD ultrasound and CTA independently. The accuracy of these two methods was compared.
Results
The accuracy of diagnosing bilateral middle cerebral artery, bilateral vertebral artery and bilateral internal carotid artery lesions with a TCD examination was significantly higher than that with a CTA examination. There were no significant differences in the accuracy of diagnosing bilateral anterior cerebral artery, bilateral posterior cerebral artery or basilar artery lesions between TCD ultrasound and CTA. The accuracy of diagnosing all cerebral arterial ischemic lesions was significantly higher with a TCD examination (87.39%) than with a CTA examination (69.75%). The accuracy of diagnosing all cerebral arteries that cause ischemic encephalopathy (cerebrovascular + cervical blood vessels) was significantly higher with a TCD examination (88.03%) than with a CTA examination (69.01%).
Conclusions
TCD ultrasound has several advantages over CTA. Therefore, TCD ultrasound is better for diagnosing ischemic encephalopathy than CTA.
Keywords
Introduction
The incidence of ischemic cerebrovascular disease is still increasing yearly. A recent report stated that a person dies of cerebrovascular disease every 12 s in the world and, in the event of stroke, the recurrence rate is 30% 5 years after stroke, which has caused a heavy burden to families and society.1,2 Direct economic losses can be as high as ≥$10 billion (including medical expenses) caused by this disease, which also leads to difficulties in the community, families and individuals.3–5
Ischemic cerebrovascular disease includes cerebral infarction (also known as ischemic stroke) and transient ischemic attack of which the highest rate of morbidity is from cerebral infarction.6,7 Many clinical reports have shown that extracranial carotid atherosclerosis stenosis or occlusion is closely related to the occurrence of ischemic cerebrovascular disease, development of cerebral infarction and recurrence of cerebral infarction. 8 Timely surgical treatment is required when carotid stenosis is >70%, and the incidence of cerebral infarction can be greatly reduced, which may greatly reduce the patients’ morbidity and mortality. 9 Therefore, the detection of neck arterial lesions is important and necessary. Digital subtraction angiography (DSA) is used as the gold standard for diagnosing vascular lesions in clinical practice. However, DSA is an invasive examination with a large amount of side effects, a high cost and is not easily accepted by patients. In addition, DSA cannot be used on blood vessel walls and surrounding tissue structure, which has hindered its use in the diagnosis of cervical vascular disease. In 1982, the transcranial Doppler (TCD) detection technique was applied to clinical practice because of its noninvasive examination, low cost of inspection, reliable results and high portability.10–13 Computed tomography angiography (CTA) technology and the rapid development of 64-slice spiral CTA have the advantage of displaying arterial disease with a high temporal and spatial resolution, and they have excellent image reprocessing techniques. An increase of spatial resolution has also greatly improved the image quality of head and neck CTA.14–16
This study aimed to further examine the best method to diagnose patients with ischemic cerebrovascular disease. We performed a retrospective clinical study on clinical data of patients with ischemic cerebrovascular disease who were diagnosed by DSA. Under the single-blind condition, two experienced senior practitioners were selected to diagnose the patients with TCD and CTA independently. We then compared the accuracy of TCD and CTA examinations in these patients for diagnostic purposes.
Material and methods
General information
A retrospective clinical study was conducted on the clinical data of patients who were admitted to our hospital with ischemic cerebrovascular disease and were diagnosed by DSA from July 2015 to July 2016. The patients initially had a brain computed tomography scan taken to exclude hemorrhagic lesions. Under the single-blind condition, two experienced senior practitioners were selected to diagnose the patients with TCD and CTA independently. We then compared the accuracy of TCD and CTA examinations of these patients for diagnostic purposes. We also recorded the patient’s age, blood pressure, blood sugar concentrations, blood lipid concentrations and other characteristics. We de-identified all patients’ details. The reporting of this study conforms to the STROBE guidelines. 17
Inclusion criteria
Patients who had ischemic cerebrovascular disease diagnosed by DSA were enrolled in the study. All patients had complete medical records and no contraindications. Patients were voluntarily involved in the study and the study was approved by the Medical Ethics Committee of the Second Affiliated Hospital of Dalian Medical University (approval number: LL202102). All of the patients provided written informed consent.
Diagnostic methods
Cerebrovascular CTA was performed using the Philips Brilliance 16-slice spiral CT machine (Royal Philips, Amsterdam, The Netherlands). The patient was placed in the supine position and head and neck scan position images were obtained. The contrast agent iodide (370 mgI/mL, 90–100 mL) was injected at a flow rate of 3.5 to 4.0 mL/s using a Nemoto high pressure syringe (Nemoto Kyorindo Co., Ltd., Tokyo, Japan) through the median cubital vein. The scan delay time was started according to the Bolus Tracking intelligent trigger with a trigger threshold of 110 Hu, and we performed a cross-section spiral volume scan. During the scanning process, the patient’s head and neck were absolutely mobilized, and the scanning range was from the aortic arch to 2 cm below the cranial roof. The scanning parameters were as follows: 120 kV; 200 mAs; collimation, 16 × 0.75; pitch, 1.188; tube rotation, 0.4 s; matrix, 512 × 512; thickness, 0. 8 mm; and distance, 0. 6 mm. After scanning, the original volume data were transferred over the local area network to the Philips Extended Brilliance™ Workspace or GE AW4.4 image post-processing station (GE Healthcare, Chicago, IL, USA). To obtain maximum intensity projection and volume rendering images. Curved planar reconstruction was performed by blood vessel analysis software for bilateral middle cerebral arteries, bilateral anterior cerebral arteries, bilateral posterior cerebral arteries, bilateral vertebral arteries, the basilar artery and bilateral internal carotid arteries.
The TCD examination method was performed using a transcranial Doppler ultrasound detector produced by Germany Kay Electronics Co. (Shenzhen City, China) and a 1.6-MHz probe. The patients were detected by two experienced clinicians independently. The patients were placed in the supine position for the temporal window and in the lateral position for the occipital window to detect bilateral middle cerebral arteries, bilateral anterior cerebral arteries, bilateral posterior cerebral arteries, bilateral vertebral arteries, the basilar artery and bilateral internal carotid arteries. We recorded the peak blood flow velocity in each artery, mean blood flow velocity and end-diastolic blood flow velocity. The changes in spectral morphology and the arterial pulse index were also recorded.
Statistical analysis
The data of each group were analyzed by PASW Statistics for Windows, Version 18.0 software (SPSS Inc., Chicago, IL, USA). One-way analysis of variance and the z-test were used to analyze the differences between the two groups. All data are expressed as mean ± standard deviation. For data with a normal distribution, single-factor analysis of variance was used. The least significant difference t test for pairs of two comparisons was used when the difference was statistically significant. P < 0.05 was considered statistically significant.
Results
We included 142 patients of whom 73 were men and 69 were women. Their age ranged from 32 to 71 years, with a median age of 51.9 ± 8.6 years.
First, we investigated the effect of CTA for diagnosing all ischemic cerebrovascular diseases of the cerebral arteries that cause ischemic encephalopathy. Figure 1 shows representative CTA images of ischemic cerebrovascular disease in bilateral middle cerebral arteries (Figure 1a, b), bilateral posterior cerebral arteries (Figure 1c), the basilar artery (Figure 1d), bilateral internal carotid arteries (Figure 1e) and bilateral vertebral arteries (Figure 1f). We then analyzed the application of TCD for diagnosing global cerebral artery ischemic cerebrovascular disease. Figure 2 shows representative TCD images of ischemic cerebrovascular disease in bilateral anterior cerebral arteries (Figure 2a), bilateral middle cerebral arteries (Figure 2b), bilateral posterior cerebral arteries (Figure 2c), the basilar artery (Figure 2d), bilateral internal carotid arteries (Figure 2e) and bilateral vertebral arteries (Figure 2f).
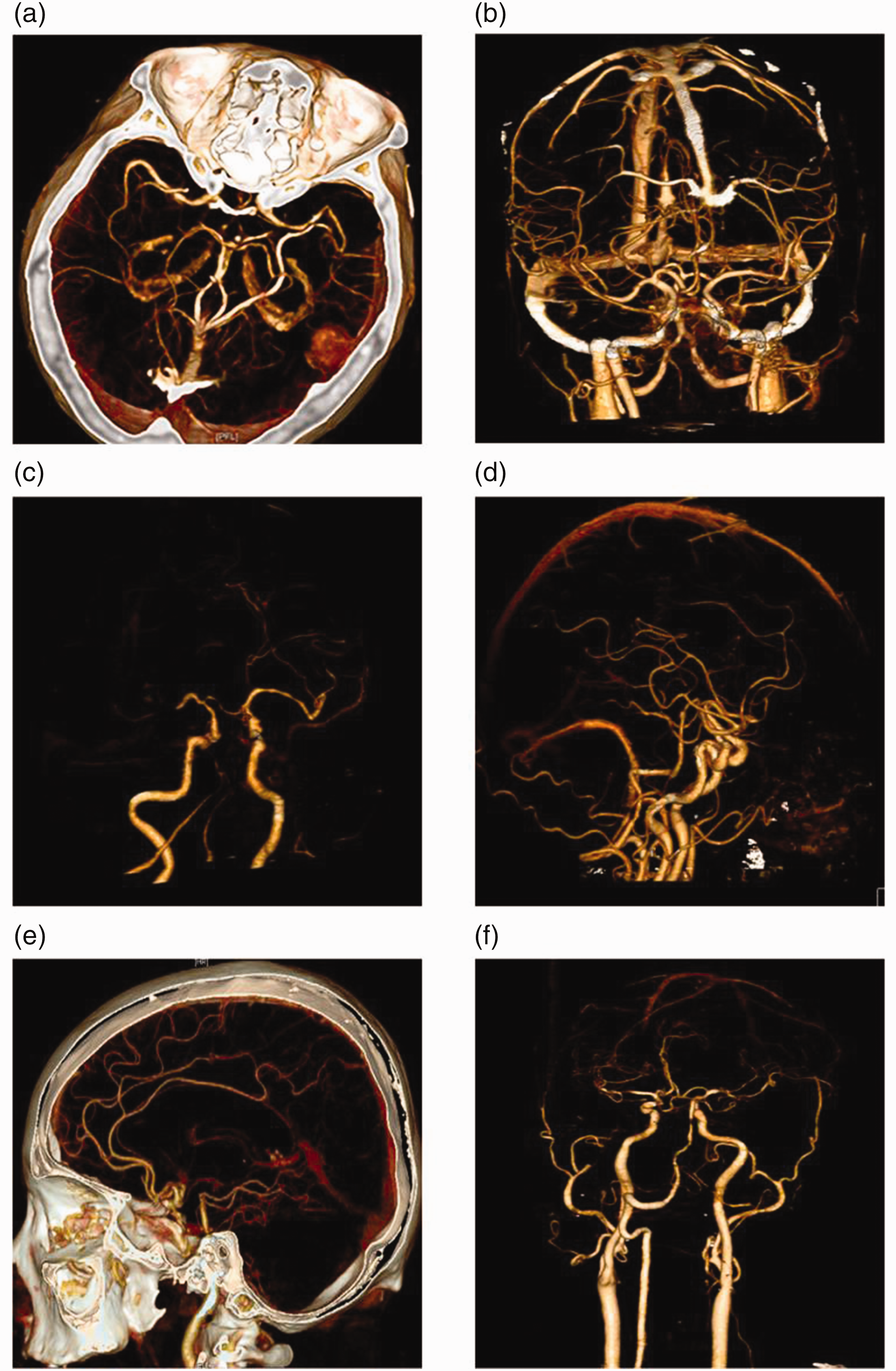
Computed tomography angiography scan of ischemic cerebrovascular disease in all cerebral arteries that cause ischemic encephalopathy. (a, b) Bilateral middle cerebral arteries, (c) bilateral posterior cerebral arteries, (d) the basilar artery, (e) bilateral internal carotid arteries and (f) bilateral vertebral arteries.

Transcranial Doppler ultrasound for detecting ischemic cerebrovascular disease in cerebral arteries. (a) Bilateral anterior cerebral arteries, (b) bilateral middle cerebral arteries, (c) bilateral posterior cerebral arteries, (d) the basilar artery, (e) bilateral internal carotid arteries and (f) bilateral vertebral arteries.
The accuracy of a TCD examination for diagnosing bilateral middle cerebral artery, bilateral vertebral artery and bilateral internal carotid artery lesions was significantly higher than that of a CTA examination (all P < 0.05) (Table 1). There were no significant differences in the accuracy of diagnosing bilateral anterior cerebral artery, bilateral posterior cerebral artery or basilar artery lesions between CTA and TCD examinations. The accuracy of a TCD examination for diagnosing all cerebral arterial ischemic lesions was significantly higher than that of a CTA examination (87.39% vs 69.75%, P < 0.05). The accuracy of a TCD examination for diagnosing all cerebral arteries that cause ischemic encephalopathy (cerebrovascular + cervical blood vessels) was significantly higher than that of a CTA examination (88.03% vs 69.01%, P < 0.05).
Comparison of DSA, TCD and CTA in the detection of all cerebral arteries that cause ischemic encephalopathy.

Values are n (%).
DSA, digital subtraction angiography; TCD, transcranial Doppler; CTA, computed tomography angiography; MAC, middle cerebral artery; ACA, anterior cerebral artery; PCA, posterior cerebral artery; VA, vertebral artery; BA, basilar artery; ICA, internal carotid artery; Cas, cerebral arteries.
Discussion
Cerebrovascular disease is one of the most common diseases of the nervous system and also a major public health problem that affects the population, especially older people. In the USA, stroke is the third most common cause of death and the primary cause of serious, long-term disability. 17 In November 2005, the World Health Organization reported that the global stroke death toll was 5.6 million, and people aged older than 60 years ranked second in global stroke deaths and the number of stroke deaths in China ranked second (180/10 million).
The occurrence and development of ischemic cerebrovascular disease is closely related to many factors and these risk factors can be divided into two categories of factors that cannot be affected and factors that can be affected. Risk factors that cannot have any intervention are age, sex, and genetic inheritance, and factors that can have intervention are hypertension, diabetes, heart disease, smoking, alcoholism, dyslipidemia, carotid stenosis, habitual salt intake, lack of exercise and high plasma fibrin concentrations. Continuous improvement of stroke risk factors has led to hyperhomocysteinemia being identified as an independent risk factor for stroke. Previous studies have shown that common risk factors for stroke are sex differences, and the average age of stroke in female patients is higher than that in male patients. 18 We also previously found that diabetes and atrial fibrillation were independent risk factors for the onset of stroke in women while smoking and alcohol abuse was an independent risk factor in male patients.19,20
In recent years, with the development of imaging technology, the diagnosis of ischemic cerebrovascular disease has been further improved. Conventional CT examinations, computed tomography perfusion, CTA, TCD and magnetic diffusion-weighted imaging have gradually been applied to clinical diagnosis, especially TCD and CTA because of their unique advantages. However, the ideal imaging strategy for ischemic cerebrovascular disease has not yet reached a consensus.21–24 Comparison of the clinical application of imaging can avoid unnecessary screening and a waste of imaging resources, and provide an early diagnosis, early treatment as soon as possible and greater benefits for patients.
Our study showed that the accuracy of diagnosing bilateral middle cerebral artery and bilateral vertebral artery lesions was significantly higher with a TCD examination than with a CTA examination. However, there was no significant difference in the accuracy of diagnosing ischemic cerebrovascular disease in bilateral anterior cerebral arteries between TCD and CTA examinations. There were also no significant differences in diagnosing ischemic cerebrovascular disease in bilateral posterior cerebral arteries or the basilar artery between TCD and CTA examinations. The accuracy of diagnosing ischemic cerebrovascular disease in bilateral internal carotid arteries was significantly higher with a TCD examination than with a CTA examination. This study showed that the accuracy of diagnosing all cerebral arterial ischemic lesions was significantly higher with a TCD examination than with a CTA examination. Furthermore, the accuracy of diagnosing all cerebral arteries that cause ischemic encephalopathy (cerebrovascular + cervical blood vessels) was significantly higher with a TCD examination than with a CTA examination.
In summary, the accuracy of a TCD examination for diagnosing cerebral arterial ischemic lesions was significantly higher than that of a CTA examination. The process of a TCD examination is relatively simple and patients can have repeated examinations. Therefore, this method should be used as the preferred method for diagnosing ischemic encephalopathy.
This study has some potential limitations. This was a retrospective clinical study and the sample size was small. In future studies, we will continue to increase the sample size to improve the accuracy and credibility of our findings.
Conclusion
TCD ultrasound has certain advantages for the diagnosis of ischemic cerebrovascular disease. This technique shows the location and extent of vascular lesions in real time, and improves the sensitivity and accuracy of diagnosing disease. TCD ultrasound can be applied to predict and evaluate the therapeutic effect of disease and to help patients achieve rehabilitation as soon as possible.
Footnotes
Author contributions
Jun Gao made substantial contributions to the conception and design of this study. Yu Wang performed the statistical analysis and interpretation of data, and was involved in drafting the manuscript. Qian Ding critically reviewed the manuscript and supervised the whole study process. All authors read and approved the final manuscript. All authors agreed to be accountable for all aspects of the work.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.