
Abstract
Objectives
Retrospective study to evaluate the diagnostic utility of rheumatoid factor (RF), anticyclic citrullinated peptide antibodies (ACPA) and antikeratin antibodies (AKA) in a broad age range of patients with rheumatoid arthritis (RA).
Methods
Clinical and serological data from patients with RA were collected and analysed. Patients were stratified according to age (<16 years [juvenile idiopathic arthritis; JIA], 16–40 years; 41–60 years and >60 years) and sex.
Results
The study included 3725 patients. There were no significant sex-related differences in rates of RF, ACPA or AKA positivity. RF, ACPA and AKA positivity were significantly less common in patients aged <16 years than those aged ≥16 years. There were no other significant differences between age groups.
Conclusions
RF, ACPA and AKA have better diagnostic value for RA in adult patients than in patients with JIA. A combination of RF, ACPA and AKA serological testing may be a useful diagnostic tool for RA in Chinese adults.
Keywords
Introduction
Rheumatoid arthritis (RA) is a systemic inflammatory disease involving hyperplasia of synovial tissues and chronic joint inflammation, affecting ∼1% of the population worldwide. 1 The disease course ranges from mild to aggressive, and early diagnosis and treatment can reduce joint destruction, preserve function and prevent disability. 2 Because of the highly variable and unpredictable course of RA, diagnostic tests with high specificity are desirable to enable early treatment.
Current clinically useful diagnostic markers for RA are acute phase reactants or autoantibodies. These include inflammatory markers (such as erythrocyte sedimentation rate [ESR] 3 and C reactive protein [CRP] level), 4 but disease damage may progress despite decreased inflammatory activity, and erosions can develop in patients without clinical sings of significant inflammation.5,6 ESR and CRP levels may reflect the disease activity of RA but the diagnostic value of both is poor. Diagnostic autoantibodies include rheumatoid factor (RF), anticyclic citrullinated peptide antibodies (ACPA) and antikeratin antibodies (AKA).7–9 Of these, RF has a low specificity for RA, 10 AKA has good specificity but poor sensitivity, 11 and ACPA is both sensitive and has high positive predictive value for RA diagnosis. 12 A combination of these autoantibodies provides a useful serological test for the diagnosis of RA.
Juvenile idiopathic arthritis (JIA) is the most common chronic rheumatological disease in children and adolescents, and is one of the most common chronic diseases of childhood. 13 Its aetiology and pathogenesis are not completely understood, and it differs from adult RA in terms of initial presentation. 13 Diagnosis of JIA is complicated as there is no specific single test; physicians use a combination of blood tests for inflammatory markers and autoantibodies, X-rays and clinical presentation.
It is unknown whether the diagnostic value of autoantibodies varies between children with JIA and adults with RA, and if so, which markers are more suitable for the diagnosis of patients in different age groups. The present retrospective study evaluated the diagnostic value of RF, ACPA and AKA in a broad age-range of Chinese patients with RA.
Patients and methods
Study population
This retrospective study included patients aged 5–80 years with confirmed RA who underwent treatment at the Department of Rheumatology and Immunology, the First Affiliated Hospital of Fujian Medical University, Fuzhou, China between July 2007 and August 2013. Exclusion criteria were: clinically significant infection; congestive heart failure; recent stroke (within 4 months); history of malignancy. RA was diagnosed according to the revised criteria of the American College of Rheumatology. 14 JIA was defined by patient age (<16 years) and duration of disease (>6 weeks). 14 Data regarding duration of disease, number of tender or swollen joints (of 28 joints tested), physical function score (Modified Standard Health Assessment Questionnaire 15 ), patient’s and physician’s assessment of pain and activity level (visual analogue scale from 0–10, with higher values indicating more severe impairment), Hospital for Special Surgery (HSS) knee score 16 (range 0–100, lower scores indicate greater disease activity), and serum CRP and ESR values were obtained from medical records, following routine analyses.
Study protocols were approved by the Institutional Medical Ethics Review Board of The First Affiliated Hospital of Fujian Medical University, Fuzhou, China. Patients provided written or verbal consent prior to inclusion in the study.
Laboratory analyses
Laboratory data were obtained from medical records; no analyses were performed on stored samples. Blood samples were originally taken using standard procedures and analysed in the course of routine treatment. Blood samples were centrifuged at 3500 r.p.m. (Sorvall™ ST 40; Thermo Scientific, Waltham, MA, USA) for 5 min at room temperature. Enzyme-linked immunosorbent assays (EUROIMMUN AG, Lübeck, Germany), performed according to the manufacturers’ protocols, were used to quantify serum ACPA (second-generation ACPA) and AKA. ACPA data were expressed as RU/ml and values >5 RU/ml were considered positive. An AKA titre >1 : 10 was considered positive. Serum RF was quantified by immunoturbidimetric assay (Dade Behring, Marburg, Germany), with values ≥10 IU/ml considered positive.
Statistical analyses
Data were presented as mean ± SD or n (%) and stratified according to sex or age (aged <16 [representing patients with JIA], 16 – 40, 41 – 60 and >60 years). Between-group comparisons were made using χ2-test, and odds ratios (OR) with 95% confidence intervals (95% CI) were calculated. Data analyses were performed using IBM SPSS® version 21.0 (IBM SPSS, Tokyo, Japan). P-values <0.05 were considered statistically significant.
Results
Clinical and demographic characteristics of a cohort of Chinese patients with rheumatoid arthritis (n = 3725) who participated in a retrospective study to evaluate the diagnostic utility of rheumatoid factor (RF), anticyclic citrullinated peptide antibodies and antikeratin antibodies.
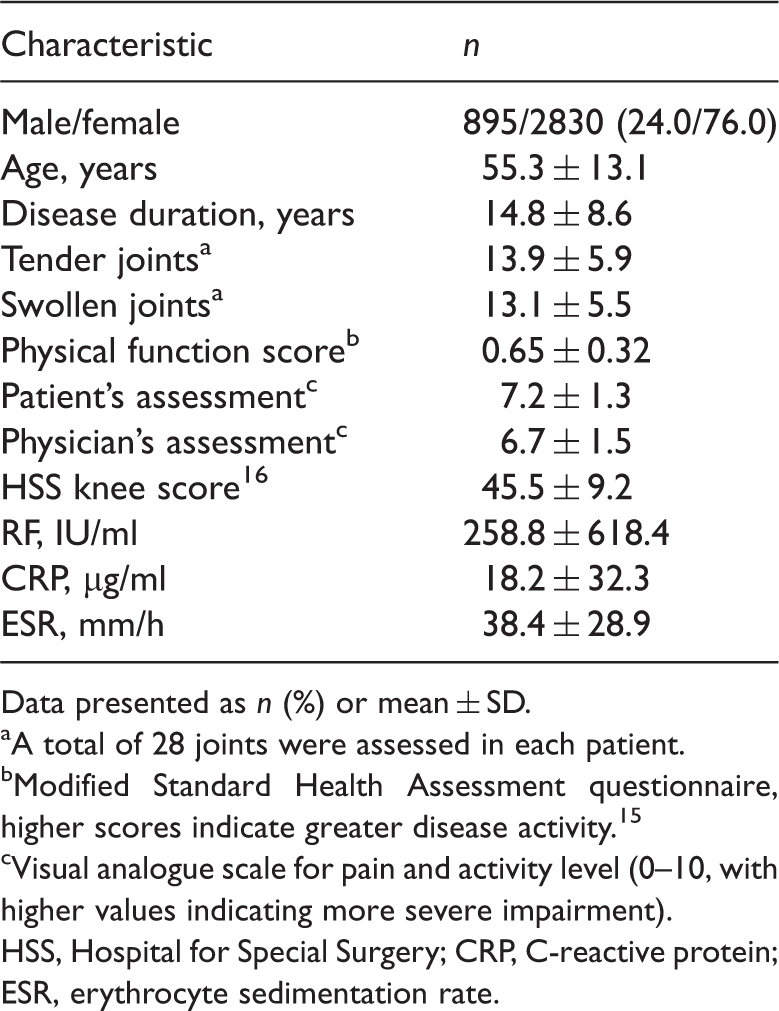
Data presented as n (%) or mean ± SD.
A total of 28 joints were assessed in each patient.
Modified Standard Health Assessment questionnaire, higher scores indicate greater disease activity. 15
Visual analogue scale for pain and activity level (0–10, with higher values indicating more severe impairment).
HSS, Hospital for Special Surgery; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
Concentrations of rheumatoid factor (RF), anticyclic citrullinated peptides (ACPA) and antikeratin antibodies (AKA) in serum samples from Chinese patients with rheumatoid arthritis, stratified according to sex.
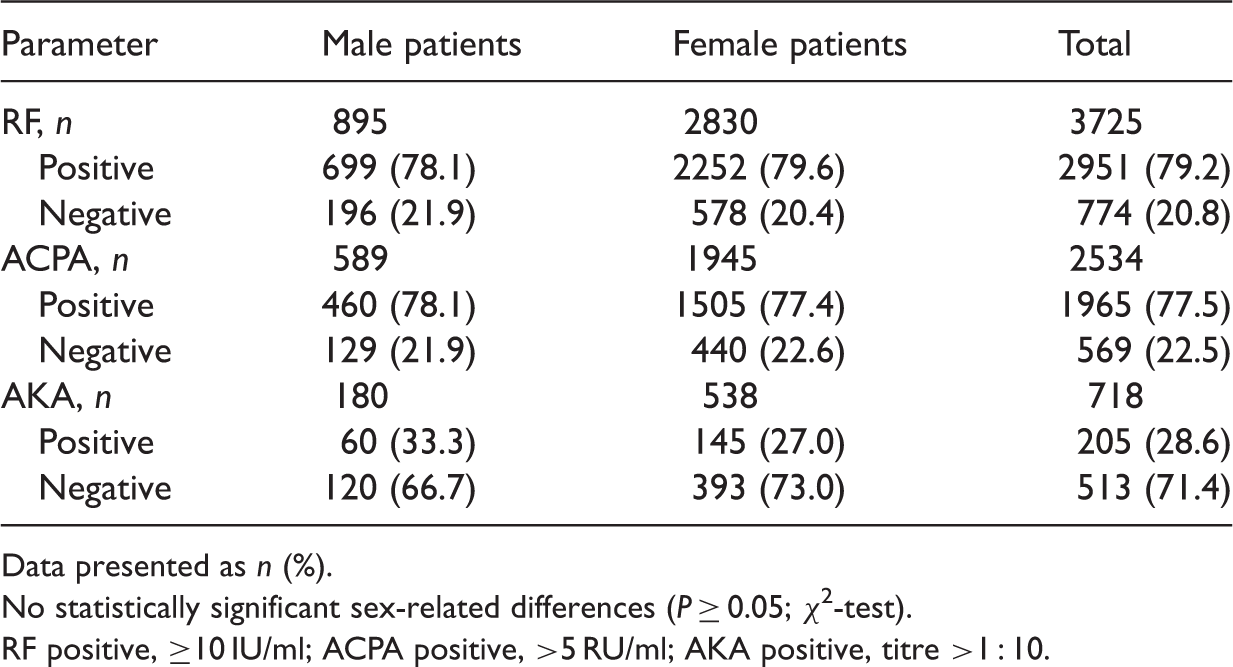
Data presented as n (%).
No statistically significant sex-related differences (P ≥ 0.05; χ2-test).
RF positive, ≥10 IU/ml; ACPA positive, >5 RU/ml; AKA positive, titre >1 : 10.
Concentrations of rheumatoid factor (RF), anticyclic citrullinated peptides (ACPA) and antikeratin antibodies (AKA) in serum samples from Chinese patients with rheumatoid arthritis, stratified according to age group.

Data presented as n or n (%).
OR: odds ratio; 95% CI: 95% confidence interval.
RF positive, ≥10 IU/ml; ACPA positive, >5 RU/ml; AKA positive, titre >1 : 10.
Discussion
A considerable portion of the disability in early stage and established RA is due to joint damage; 17 early diagnosis and prevention of such damage is therefore a major treatment goal. Identification of reliable disease predictors may enable modification of the disease course. Several serological biomarkers for RA (including ACPA, RF and AKA) have been evaluated, 18 and the findings of the present study indicate that these laboratory variables differ between JIA and adult RA.
Juvenile idiopathic arthritis is an umbrella term used to indicate a childhood-onset disease, characterized primarily by arthritis of unknown aetiology, which persists for ≥6 weeks. 19 The development of JIA is influenced by gene–gene interactions 20 and the Th1/Th2 pathway. 21 The present finding that RF-, ACPA- and AKA-positive status was significantly lower in patients aged <16 years (although higher than the findings of others 22 ) compared with those aged ≥16 years suggest that these laboratory variables may not be useful diagnostic markers for JIA. Studies have suggested an association between JIA and interleukin (IL) 6 polymorphism, 23 as well as the presence of anticitrullinated type II collagen and anticitrullinated fibrinogen antibodies. 24 It is likely that a combination of IL-6 genotyping and the detection of anticitrullinated type II collagen and anticitrullinated fibrinogen antibodies may be a useful diagnostic approach for JIA.
The present study found no RF, ACPA or AKA status differences between male and female patients, between patients aged 16–40 years and 41–60 years, or between those aged 41–60 years and >60 years. RF levels are elevated in 75% of patients with RA and this analysis is widely used for diagnosis. 25 ACPA positivity is frequently observed in patients with RA, especially in early disease,26,27 and has a specificity approaching 100% for RA diagnosis. 28 The sensitivities of RF, ACPA and AKA in patients aged >16 years in the present study were 80.1%, 78.2% and 29.1%, respectively, and there were no significant differences in the rates of RF-, ACPA- or AKA-positive status between different age categories (in patients ≥16 years).
In conclusion, RF, ACPA and AKA appear to have better diagnostic value for RA in adult patients than in patients with JIA. A combination of RF, ACPA and AKA serological testing may be an optimal diagnostic tool for RA in Chinese adults. Useful laboratory variables for the diagnosis of JIA require further investigation.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.