
Abstract
Objective
Esophagectomy is a high-risk surgical procedure with significant postoperative morbidity and mortality. This study aimed to investigate the risk factors of cervical anastomotic leakage and postoperative mortality.
Methods
In this retrospective, observational study, we recruited 1010 patients with esophageal cancer. Cox regression analysis was performed to identify factors affecting anastomotic leakage and postoperative mortality. After propensity score matching, the Kaplan–Meier curve was used to evaluate the effect of leakage on postoperative mortality.
Results
The number of patients with cervical anastomotic leakage, in-hospital mortality, 30-day postoperative mortality, and 60-day postoperative mortality was 194 (19.2%), 13 (1.3%), 12 (1.2%), and 16 (1.6%), respectively. The total length of hospital stay and hospital stay postoperatively were 29.7 ± 21.1 and 21.3 ± 20.3 days, respectively. Diabetes, stage IV, and an upper thoracic tumor were significant risk factors for leakage. Leakage and diabetes were significant risk factors for postoperative mortality. After propensity score matching, leakage also significantly affected postoperative mortality.
Conclusions
Patients with tumors in the upper thoracic segment of the esophagus may be more prone to developing anastomotic leakage compared with those with tumors in the middle or lower thoracic segment. Anastomotic leakage may prolong the length of hospital stay and increase postoperative mortality.
Keywords
Background
Esophageal cancer is the sixth most common cause of cancer-related mortality worldwide. 1 Surgical resection is the most important curative treatment option for esophageal cancer. Although the surgical technique of esophagectomy has been constantly updated and improved, it remains a complex surgery with a high mortality rate.2,3 Many of these patients suffer from life-threatening postoperative complications. Anastomotic leakage is a serious complication after resection of esophageal cancer, with a reported prevalence of 0.57% to 53%.4–6 Therefore, anastomotic leakage is an important cause of postoperative morbidity and mortality.
Intrathoracic anastomosis and cervical anastomosis are the two main methods for reconstructing the upper gastrointestinal tract. The incidence, severity, and prognosis of intrathoracic anastomotic leakage and cervical anastomotic leakage are markedly different.7,8 During the past two decades, cervical esophagogastric anastomosis (CEGA) has been increasingly used for reconstruction after esophagectomy because of its low morbidity and mortality rates compared with intrathoracic anastomoses.9,10 In a retrospective cohort study of 153 patients, the overall leakage rate, morbidity, and mortality of CEGA were 17%, 32.8%, and 6.4%, respectively. 11 In an Indian study of 77 patients, anastomotic leakage of CEGA was 19.4% and the 90-day mortality was 7.8%. 12 To overcome the relatively high leakage rate of CEGA, multiple research groups have developed varying techniques, such as stapled anastomosis, 10 partially stapled anastomosis, 11 and cervical end-to-side triangulating esophagogastric anastomosis. 13
Esophageal cancer resection is a high-risk surgical procedure. 14 To improve the clinical outcomes of this procedure, medical researchers need to investigate the risk factors for leakage and hospital mortality. Multiple clinical factors are associated with anastomotic leakage, including age, sex, preoperative weight loss, histology, tumor stage, and the location of tumors.4,15–17 However, little is known about the risk factors for postoperative mortality.
In Western countries, esophageal adenocarcinoma is the most common pathological subtype of esophageal malignancies. 18 However, in China, esophageal squamous cell carcinoma is the dominant pathological subtype. Such a pathological distinction might lead to different risk patterns for cervical anastomotic leakage and postoperative mortality in Chinese patients.
In this study, we collected clinical information of consecutive patients with esophageal cancer (histologically confirmed) who received esophagectomy with cervical anastomosis. We aimed to investigate the risk factors of cervical anastomotic leakage and in-hospital mortality after esophagectomy in Chinese patients with esophageal cancer at a high-volume cancer institute.
Methods
Patient cohort
This study included consecutive patients who had undergone esophagectomies with cervical anastomosis from January 2010 to December 2015 in the Thoracic Surgery Department of Sun Yat-sen University Cancer Center. In our institute, the majority of patients underwent the McKeown surgical procedure, and the remaining patients underwent left transthoracic procedures. All patients included in this study received cervical anastomosis. An end-to-side esophagogastric anastomosis was performed in the neck using either the single-layer hand-sewn or circular stapled anastomotic technique.
Care in the intensive care unit
All of the patients were sent to the intensive care unit after the operation. Anastomotic leakage was closely observed during the follow-up period. If any signs of leakage (e.g., fever or the presence of a purulent or salivary discharge from the cervical wound) appeared, further examinations, such as water-soluble contrast swallow study, endoscopy, or a computed tomography scan, were performed to confirm the presence of leakage. No routine diagnostic tests were performed. 19
Data collection
Relevant clinical and pathological data, including age, sex, location of the tumor, histological subtype, a history of comorbidities, such as hypertension and diabetes, pathological tumor-node-metastasis (TNM) stage, and preoperative treatment, were obtained retrospectively from electronic medical records at Sun Yat-Sen Cancer Center. The tumors were staged in accordance with the seventh edition of the Union for International Cancer Control TNM staging system. Postoperative information, such as the leakage of anastomosis, length of hospital stay, 30-day mortality rate, and in-hospital mortality rate, was also collected.
This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of the Sun Yat-sen University Cancer Center, Guangzhou, Guangdong Province, China (No. B2019-028-01). Written informed consent was obtained from the patients and all patients’ details were de-identified. The reporting of this study complies with the STROBE statement. 20 The authenticity of this article has been validated by uploading the key raw data to the Research Data Deposit public platform (www.researchdata.org.cn) (approval RDD number: RDDA2021002119).
Measurements
The main measurements in this study were cervical anastomotic leakage, the in-hospital mortality rate, and the 30-day mortality rate. Secondary measurements were the length of hospital stay after surgery and the total length of hospital stay. For survival analysis, we integrated in-hospital mortality and 30-day mortality as postoperative mortality (POM). More than 95% of patients stayed in hospital within 60 days after surgery, and all patients died within 60 days after surgery, except for one who died at 61 days after surgery. Therefore, we used 60-day postoperative mortality (POM60) as one of our primary measurements for survival analysis. All patients were followed up for 60 days. Based on the Surveillance, Epidemiology, and End Results program database, stage IV esophageal cancer had the poorest prognosis and the median overall survival (OS) was only 4 to 10 months, according to distant metastatic sites. 21 However, recent studies have suggested that aggressive local therapy with surgery after initial palliative chemotherapy can improve the median OS to 43 months in patients with stage IV esophageal cancer.22,23 Therefore, we considered that POM60 was the optimal measurement to evaluate post-surgical mortality.
Propensity score matching
To evaluate the prognostic value of leakage on CEGA, a 1:1 propensity score matching (PSM) analysis was performed to reduce the potential bias between the leakage and non-leakage groups. Propensity scores were calculated through logistic regression for each patient in the leakage and non-leakage groups. The covariates in the logistic regression were age, sex, comorbidity, histological type, tumor location, and TNM stage. Patients were matched based on the propensity score. Covariate balance was examined by the chi-square test. Survival comparisons were then performed for the matched patients using the same methods as those in the unmatched patients.
Statistical analyses
Continuous variables are shown as the mean (standard deviation) and the median (interquartile range). Frequencies and percentages are reported for categorical variables. The Student’s t test was performed to identify the different numerical variables across two subgroups. The chi-square test and Fisher’s exact test (n < 5) were used to compare categorical variables between subgroups. The Mentel–Haenszel chi-square test was used when categorical variables had more than two sub-levels. Cox regression analysis was used to evaluate the univariable and multivariable risks of candidate risk factors for progression. Kaplan–Meier curves were used to plot survival distribution against progression, and the log-rank test was used to assess differences in postoperative survival among subgroups. All tests of hypotheses were two-tailed and conducted at a significance level of 0.05. Statistical analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC, USA). All of the statistical analyses were appraised by a biostatistician.
Results
Clinicopathologic characteristics and treatment outcomes
A total of 1010 patients underwent esophagectomies with cervical anastomosis between January 2010 and December 2015 (Figure 1). Details of the clinicopathological characteristics of the patient cohort are shown in Table 1. A total of 775 (76.7%) patients were men and 144 (14.3%) had comorbidities (hypertension and/or diabetes). Squamous cell carcinoma was the dominant histological subtype. Only 1.1% of esophageal cancers were adenocarcinoma. Other histological types included small cell carcinoma, neuroendocrine carcinoma, and malignant melanoma. Most tumors were located in the middle thoracic esophagus. The majority of patients were in stage II or stage III. Twenty patients with stage IV received CEGA after esophagectomy. A total of 113 (11.2%) patients received preoperative treatment, which comprised neoadjuvant chemotherapy and neoadjuvant chemoradiotherapy. Cervical anastomotic leakage occurred in 194 (19.2%) patients. POM60 occurred in 16 (1.6%) patients. The total length of hospital stay was 29.7 ± 21.1 days.

Flow chart of the patients.
Clinical and pathological characteristics of the recruited cohort.

Values are mean ± standard deviation, median (range), or n (%).
TNM, tumor-node-metastasis.
Clinical and pathological risk factors for cervical anastomotic leakage
The occurrence of cervical anastomotic leakage was closely observed in the intensive care unit. To determine the potential risk factors for leakage, univariable and multivariable Cox regression analyses were performed. Univariable Cox regression analysis showed that diabetes and a stage IV tumor were significant risk factors for cervical anastomotic leakage (Table 2). The hazard of leakage in patients with diabetes with or without hypertension was 1.91 times higher than that in patients without any comorbidity (95% confidence interval [CI] = 1.00, 3.65; p = 0.05). The hazard of leakage in patients with a stage IV tumor was 2.95 times higher than that in patients with a stage I tumor (95% CI = 1.12, 7.77; p = 0.03). In contrast, a lower tumor location was an important protective factor against cervical anastomotic leakage. Patients with middle and lower thoracic esophageal cancer had a lower hazard of leakage with hazard ratios (HRs) of 0.08 (95% CI = 0.45, 1.05; p = 0.08) and 0.46 (95% CI = 0.26, 0.82; p = 0.009), respectively, compared with patients with upper thoracic esophageal cancer. Patients with radio-chemotherapy tended to show a lower hazard of cervical anastomotic leakage compared with patients without preoperative treatment (HR = 0.38, 95% CI = 0.14, 1.04; p = 0.06).
Clinical and pathological risk factors for cervical anastomotic leakage.
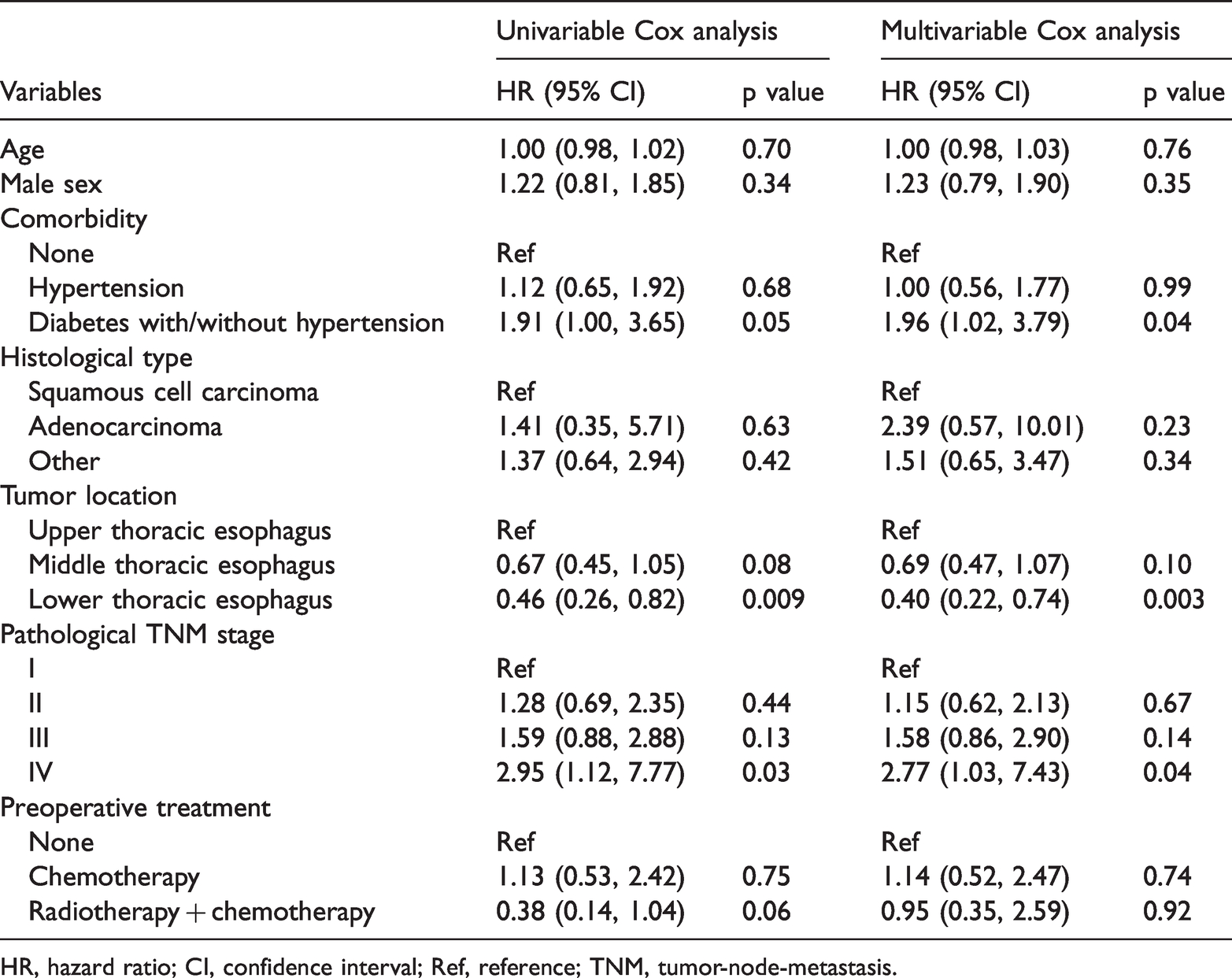
HR, hazard ratio; CI, confidence interval; Ref, reference; TNM, tumor-node-metastasis.
Multivariable Cox regression analysis also showed that diabetes with or without hypertension and a stage IV tumor were significant risk factors for cervical anastomotic leakage (HR = 1.96, 95% CI = 1.02, 3.79; p = 0.04 and HR = 2.77, 95% CI = 1.03, 7.43; p = 0.04, respectively). A lower thoracic tumor location had a protective effect against cervical anastomotic leakage (HR = 0.4, 95% CI = 0.22, 0.74; p = 0.003, Table 2). Other candidate factors, such as age and male sex, did not show a significant effect on leakage. While the hazard of leakage of adenocarcinoma was 2.39 times higher than that in squamous cell carcinoma, adenocarcinoma did not show a significant risk effect owing to the small samples size of only 11 patients with adenocarcinoma (Table 1).
Length of hospital stay and postoperative mortality
Leakage is a serious complication of cervical anastomosis after esophagectomy, leading to morbidity and a longer hospital stay. We found that the leakage group had a significantly higher in-hospital mortality rate (p = 0.001), 30-day post-operative mortality rate (p < 0.0001), and POM60 (p < 0.0001) than the non-leakage group (Table 3). Additionally, the leakage group had a significantly longer total length of hospital stay (p < 0.0001) and a longer length of hospital stay after surgery than the non-leakage group (both p < 0.001) (Table 3). These findings suggest that cervical anastomotic leakage leads to a longer postoperative hospital stay and a higher postoperative mortality rate.
Different treatment outcomes between the cervical anastomotic leakage group and the non-leakage group.
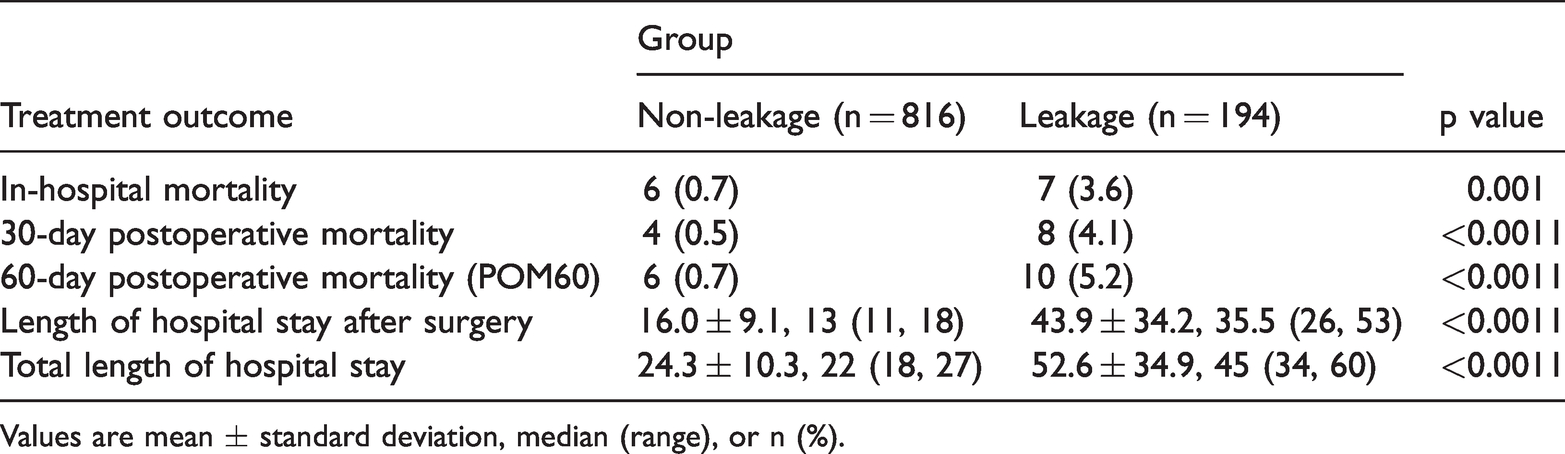
Values are mean ± standard deviation, median (range), or n (%).
Clinical and pathological risk factors for postoperative mortality
To determine the potential factors affecting postoperative mortality, univariable and multivariable Cox regression analyses were performed. We followed up all recruited patients as long as 60 days after esophagectomy. POM60 was the primary outcome measurement. Univariable and multivariable Cox regression analyses showed that leakage and diabetes with or without hypertension were significant risk factors for POM60 (Table 4). The HRs (95% CIs) of leakage for POM60 in univariable and multivariable analyses were 4.60 (1.54, 13.73; p = 0.006) and 6.05 (1.65, 22.23; p = 0.007), respectively. The HRs (95% CIs) of diabetes with or without hypertension for POM60 in univariable and multivariable analyses were 4.65 (1.25, 17.28; p = 0.02) and 5.89 (1.42, 24.48; p = 0.01), respectively. Other candidate variables, such as age, sex, histology, tumor location, and tumor stage, did not show a significant effect on POM60.
Clinical and pathological risk factors for 60-day postoperative mortality.

HR, hazard ratio; CI, confidence interval; Ref, reference; TNM, tumor-node-metastasis.
Effect of cervical anastomotic leakage on postoperative mortality
While Cox regression analyses showed that cervical anastomotic leakage was a significant risk factor for postoperative mortality, some clinicopathological features were not balanced between the groups. More patients in the non-leakage group had a lower thoracic tumor, and received both radiation and chemotherapy than those in the leakage group (Table 5). Such an imbalanced distribution might lead to potential bias in statistical evaluations. Therefore, to reduce this potential bias between the groups, PSM analysis was performed. After PSM, the patients were balanced between the subgroups (Table 5). The Kaplan–Meier curve with the log-rank test showed that leakage significantly affected postoperative survival within 60 days in the raw dataset and in the PSM dataset (both p < 0.05, Figure 2).
Clinical and pathological characteristics of the recruited cohort stratified by cervical anastomotic leakage and the PS-matched cohort.

Values are mean ± standard deviation, median (range), or n (%).
PS, propensity score; TNM, tumor-node-metastasis.

Kaplan–Meier curves for postoperative mortality in the raw dataset (a) and the propensity score-matched dataset (b).
Discussion
In our study, the incidence of anastomotic leakage was 19.2%, which is higher than that reported in some other studies.21–23 However, the hospital mortality rate for patients with cervical anastomotic leakage was 3.6%, and the 30-day mortality rate was 4.1%, which is lower than those in previous studies. 3 In our institution, we have good follow-up and diagnosis of anastomotic leakage. Even though we detected more cervical anastomotic leakage than reported previously, the majority of cases did not cause postoperative mortality.
Anastomotic leakage is one of the most common and serious complications after esophagectomy. Therefore, the choice of the anastomotic site has an important effect on the treatment and prognosis of esophageal cancer surgery. Commonly used anastomotic positions include cervical anastomoses and intrathoracic anastomoses. The risk of anastomotic leakage in cervical anastomoses is higher than that in intrathoracic anastomoses. However, because anastomotic leakage of the neck is outside the chest cavity and on the body’s surface, it is more convenient to deal with, drainage is more sufficient, and it is easier to control than with intrathoracic leakage. This study also suggested that after active treatment, mortality caused by cervical anastomotic leakage was not high.
In this study, the majority of the patients had stage II or stage III esophageal cancer, but only 11.2% of them received neoadjuvant treatment. In our clinical practice several years previously, the proportion of neoadjuvant treatment used for esophageal cancer was relatively low. Most previous studies on neoadjuvant therapy for esophageal cancer were based on esophageal adenocarcinoma,24,25 and relatively few of them focused on squamous cell carcinoma. In recent years, there have been advances in esophageal surgical techniques and perioperative management concepts, as well as improvement in chemotherapy regimens and chemotherapeutic support. Therefore, there is still a lack of high-level, evidence-based, clinical studies on comparison of neoadjuvant chemoradiotherapy and neoadjuvant chemotherapy. All of these factors were partly responsible for the low adoption rate of neoadjuvant chemotherapy in patients with esophageal squamous cell carcinoma. Additionally, because a major proportion of patients with esophageal cancer were from relatively poor families, this restriction of economic conditions might also be a reason why neoadjuvant therapy has not been further promoted.
At present, the effect of neoadjuvant therapy on anastomotic leakage of esophageal cancer is controversial. Some studies have suggested that neoadjuvant therapy causes anastomotic leakage,26,27 while some other studies have suggested that there is no relationship between them. 28 Even a few studies have suggested that preoperative chemoradiotherapy reduces the incidence of leakage. 29
This study showed that the incidence of anastomotic leakage appeared to be lower in patients after neoadjuvant therapy. We hypothesize that this finding may be due to a reduction in the scope of surgical resection in patients with neoadjuvant therapy, which may reduce injury and the risk of anastomotic leakage. This finding requires further study for validation.
We also found that the location of the tumor, stage IV, and diabetes had an effect on the occurrence of anastomotic leakage. Age and sex had no significant effect on anastomotic leakage. These results suggest that cervical anastomotic leakage is associated with the local characteristics of the tumor, an advanced tumor stage, and comorbidity of diabetes.
Our study showed that anastomotic leakage led to serious adverse consequences, including a prolonged hospital stay and a high in-hospital mortality rate. PSM showed that anastomotic leakage was a significant risk factor of postoperative mortality. Diabetes was not only related to leakage, but also related to postoperative mortality. These findings suggest that special care should be taken in the treatment of such patients.
Conclusions
This study suggests that patients with tumors in the upper thoracic segment of the esophagus may be more prone to developing anastomotic leakage than those with tumors in the middle or lower segment. Anastomotic leakage may significantly prolong the hospital stay and increase the postoperative mortality rate. Patients with the preoperative comorbidity of diabetes may also have increased leakage and postoperative mortality. This study had a large sample size of patients compared with many other studies. Further studies with a prospective and multicenter design will better clarify the predictive factors for cervical anastomotic leakage and short-term postoperative outcomes after esophagectomy.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211045540 - Supplemental material for Anastomotic leakage and postoperative mortality in patients after esophageal cancer resection
Supplemental material, sj-pdf-1-imr-10.1177_03000605211045540 for Anastomotic leakage and postoperative mortality in patients after esophageal cancer resection by Quanguan Su, Chenxi Yin, Wei Liao, Haoxian Yang, Liying Ouyang, Rong Yang and Gang Ma in Journal of International Medical Research
Footnotes
Acknowledgement
We thank Dr. Haoyu Zhou (College of Information and Intelligence, Hunan Agricultural University, Changsha, China) for his assistance with biostatistical analyses.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding by the National Science Foundation of China (No. 61972147_) was used to support Dr. Zhou’s analyses.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.