
Abstract
Background
Thoracogastric airway fistula (TGAF) is a serious complication of esophagectomy for esophageal cancer. We conducted a systematic review of the appropriate therapeutic options for acquired TGAF.
Methods
We performed a literature search to identify relevant studies from PubMed, EMBASE, and Web of Science using the search terms “gastric airway fistula”, “gastrotracheal fistula”, “gastrobronchial fistula”, “tracheogastric fistula”, “bronchogastric fistula”, “esophageal cancer”, and “esophagectomy”.
Result
Twenty-four studies (89 patients) were selected for analysis. Cough was the main clinical presentation of TGAF. The main bronchus was the most common place for fistulas (53/89), and 29 fistulas occurred in the trachea. Almost 73% (65/89) of patients underwent non-surgical treatment of whom 87.7% (57/65) received initial fistula closure. Twenty-three patients underwent surgery, including 19 (82.6%) with initial closure. The 1-, 2-, 3-, 6-, and 9-month survival rates in patients who underwent surgical repair were 95.65%, 95.65%, 82.61%, 72.73%, and 38.10%, respectively, and the equivalent survival rates in patients with tracheal stent placement were 91.67%, 86.67%, 71.67%, 36.96%, and 13.33%, respectively.
Conclusion
TGAF should be suspected in patients with persistent cough, especially in a recumbent position or associated with food intake. Individualized treatment should be emphasized based on the general condition of each patient.
Keywords
Introduction
Thoracogastric airway fistula (TGAF) is a rare and potentially fatal complication after esophagectomy for esophageal cancer, with an estimated incidence of 0.3% to 1.5%.1–3 This condition involves an abnormal connection between the airway and thoracostomach, which has been pulled up to the thorax and reconstructed to replace the esophagus. Gastric juices and contents then flow into the tracheobronchial tree through the fistula, resulting in various symptoms. The clinical presentation of TGAF varies from mild to fatal, and includes fever, cough, choking, expectoration, burning sensation, chest pain, pneumonia, dyspnea, and life-threatening hemoptysis. However, an early diagnosis and suitable treatment can effectively prevent the progress of TGAF and improve the patient’s quality of life. The main treatment choices include surgical repair and stent implantation, and although other non-surgical treatments have gradually emerged, these have only been represented in case reports. There is currently no widely accepted strategy for TGAF. We therefore searched the relevant literature and analyzed the available data to outline the appropriate diagnostic methods and therapeutic options for TGAF.
Materials and methods
This systematic review was carried out according to the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement guidelines. The PRISMA flow chart is shown in Figure 1.

Patient selection flow chart. Twenty-four studies were included in this review.
Data-searching strategy
A computerized literature search was performed to identify relevant studies in the PubMed, EMBASE, and Web of Science databases, from the inception of each database to January 2019. The search terms were “gastric airway fistula”, “gastrotracheal fistula”, “gastrobronchial fistula”, “tracheogastric fistula”, “bronchogastric fistula”, “esophageal cancer”, and “esophagectomy”. Two reviewers searched the literature independently to identify articles appropriate for inclusion in the study, and the bibliographies of the accepted articles were also searched manually.
Study criteria
Case series and case reports associated with TGAF published in English were included. Cases that did not provide a follow-up duration, as well as reviews, editorials, letters to editors, and duplicate studies were excluded.
Data abstraction
The following variables were extracted from the full texts of each study: age, sex, location of fistula, treatment strategy, and survival time. One-, 2-, 3-, 6-, and 9-month survival were also recorded. The authors were not contacted to request additional information.
Statistical analysis
All statistical analyses were performed using SPSS Statistics for Windows, Version 21.0 (SPSS Inc., Chicago, IL, USA). Survival times are analyzed with the Kaplan–Meier method. For all analyses, a P value < 0.05 (two-tailed) was considered statistically significant.
Results
General data
We identified 151 potential records, of which 27 were excluded after removing duplicates and 88 were excluded after reviewing the titles and abstracts. After checking the full-text publications, 24 studies, including 19 case reports and 5 case series, were selected for analysis, comprising 89 patients (Figure 1). A summary of these studies is shown in Table 1. Seventy-five (84.3%) patients were men. The median age was 59.6 (range 38–78) years. Among the 24 studies, 23 patients from 11 studies (1 case series and 11 case reports) underwent surgical repair, and 60 patients from eight studies (4 case series and 4 case reports) received stent placement. The treatment strategies in the other five studies included use of a septal occluder, Amplatzer vascular plug II, over-the-scope clip, and endobronchial Watanabe spigot, and conservative treatment.
Basic data collected from included studies.
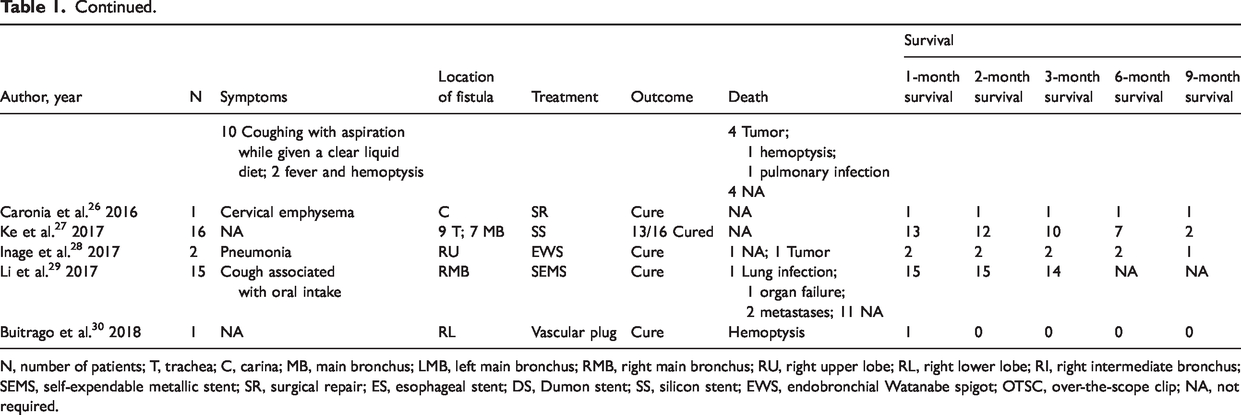
N, number of patients; T, trachea; C, carina; MB, main bronchus; LMB, left main bronchus; RMB, right main bronchus; RU, right upper lobe; RL, right lower lobe; RI, right intermediate bronchus; SEMS, self-expendable metallic stent; SR, surgical repair; ES, esophageal stent; DS, Dumon stent; SS, silicon stent; EWS, endobronchial Watanabe spigot; OTSC, over-the-scope clip; NA, not required.
Symptoms
Cough was the main clinical presentation of TGAF. Among the 24 studies included in this review, three case series did not mention the symptoms, while the other 19 case reports and two case series, comprising 57 patients, all recorded the clinical presentation. Thirty-three patients presented with cough, of whom four had a persistent cough, 13 had cough associated with oral intake, and 16 had cough in a recumbent position. Pneumonia, dyspnea, hemoptysis, and fever were the second most common clinical presentations. Other symptoms, including chest pain, sepsis, and crepitations, were also presentations of TGAF, but were rare.
Imaging
The findings on chest X-rays in patients with TGAF patients were opacities or localized consolidation, primarily at the base of the lungs and associated with the location of the fistula. If the fistula develops on the trachea and carina, the bilateral pulmonary region will be affected, while if the fistula only occurs on one of the main or intermediate bronchi, the unilateral pulmonary region will be affected. Although X-ray findings cannot show the fistula directly, these presentations support the diagnosis in patients with suspected TGAF. Gastrografin contrast swallow could effectively show the process of contrast flow, with contrast flow into the tracheobronchial tree indicating the existence of TGAF. Regarding the choice of contrast agent, water-soluble contrast materials should be the first choice because they can be absorbed rapidly. 4 Barium sulfate was the most common radiographic contrast material for upper gastrointestinal investigations; however, leakage of barium sulfate into the mediastinum may cause mediastinitis, and the deposition of barium in the alveoli may result in refractory pulmonary infection.
Computed tomography (CT) and 3D-reconstruction techniques can provide good anatomical delineation. 5 A window width of 400 HU and a window level of −50 to −100 HU were recommended for diagnosing TGAF on CT. Patients with TGAF are usually malnourished, and a conventional mediastinal window may thus display false positive signs due to a partial volume effect. The diameter of the tracheobronchial tree, as an essential parameter for stent choice and design, could also be measured from the CT image.
Endoscopy can provide visualization of the fistula, regardless of bronchoscopy or gastroscopy. However, bronchoscopy is more accurate than gastroscopy for a diagnosis of TGAF. Fischer et al. 6 reported that initial gastroscopy did not reveal a fistula, while bronchoscopy clearly showed the existence of a fistula. The main reason for this difference is that the fistula may originate in the hemiplication formed by the gastric fundus, while the surface of the bronchus is smooth, allowing the fistula to be observed clearly.
Pulmonary scintigraphy is an effective technique for exploring minimal fistulas between the tracheobronchial tree and the digestive tract. Graziani and colleagues 7 observed significant amounts of radiolabelled air in the gastric cavity in pulmonary scintigraphy, strongly supporting the existence of a passage between the airway and the stomach. 99mTc-Technegas particles are approximately 30 to 60 nm, and can thus easily diffuse through a minimal fistula.
Fistula location
The process of pulling up of the stomach into the thoracic cavity during esophagectomy for esophageal cancer means that all areas of connection between the tracheobronchial tree and stomach are at risk of forming TGAF. The main bronchus was the most common place for fistula formation (53/89), 29 fistulas occurred in the trachea, the carina showed fistula formation in three cases, two cases occurred in the intermediate bronchus, and two cases occurred in the right upper lobe and right lower lobe.
Therapeutic options
Non-surgical procedures tended to be the most popular treatment option for TGAF. Almost 73% (65/89) of patients underwent non-surgical treatment, of whom 87.7% (57/65) received initial closure of the fistula. The types of devices included a tracheobronchial self-expandable metallic stent, a Dumon stent, a silicon stent, a septal occluder, an Amplatzer vascular plug II, an over-the-scope clip, and an endobronchial Watanabe spigot. Stent placement in the tracheobronchial tree accounted for a large percentage (60/65) of the non-surgical procedures.
Surgical procedures are invasive and are typically used for benign TGAF, especially for early-stage TGAF secondary to esophagectomy. However, surgical procedures were used as a last option in some patients who failed non-surgical procedures. Shi et al. 8 and Bakho et al. 9 reported on patients in whom stent placement failed, who underwent subsequent surgical repair with good results. The types of surgical procedures included autologous fascia lata repair, pericardial flap repair, vascularized intercostal myoplasty, and Roux-en-Y gastrojejunostomy. In this review, 23 patients underwent surgery of whom 19 (82.6%) received initial closure.
Follow-up
In this review, the longest follow-up time was 48 months. 10 The 1-month survival rate for all enrolled patients was 93%, and the 2-, 3-, 6-, and 9-month survival rates were 88.6%, 75.0%, 50%, and 22.9%, respectively. The 1-, 2-, 3-, 6-, and 9-month survival rates in patients who received surgical repair were 95.65%, 95.65%, 82.61%, 72.73%, and 38.10%, respectively, while the equivalent rates in patients with tracheal stent placement were 91.67%, 86.67%, 71.67%, 36.96%, and 13.33%, respectively. Survival analysis showed that the median survival duration was significantly shorter in patients with tracheal stent placement (6 months) compared with patients with surgical repair (35.8 months) (χ2 = 8.852; P = 0.0001, log-rank test) (Figure 2). However, there was no significant difference in the median survival duration between patients with bronchial fistula (6.1 months) and patients with tracheal fistula (8 months) (χ2 = 0.017; P = 0.895, log-rank test) (Figure 3).

Survival curves of patients who received tracheal stent placement and surgery.
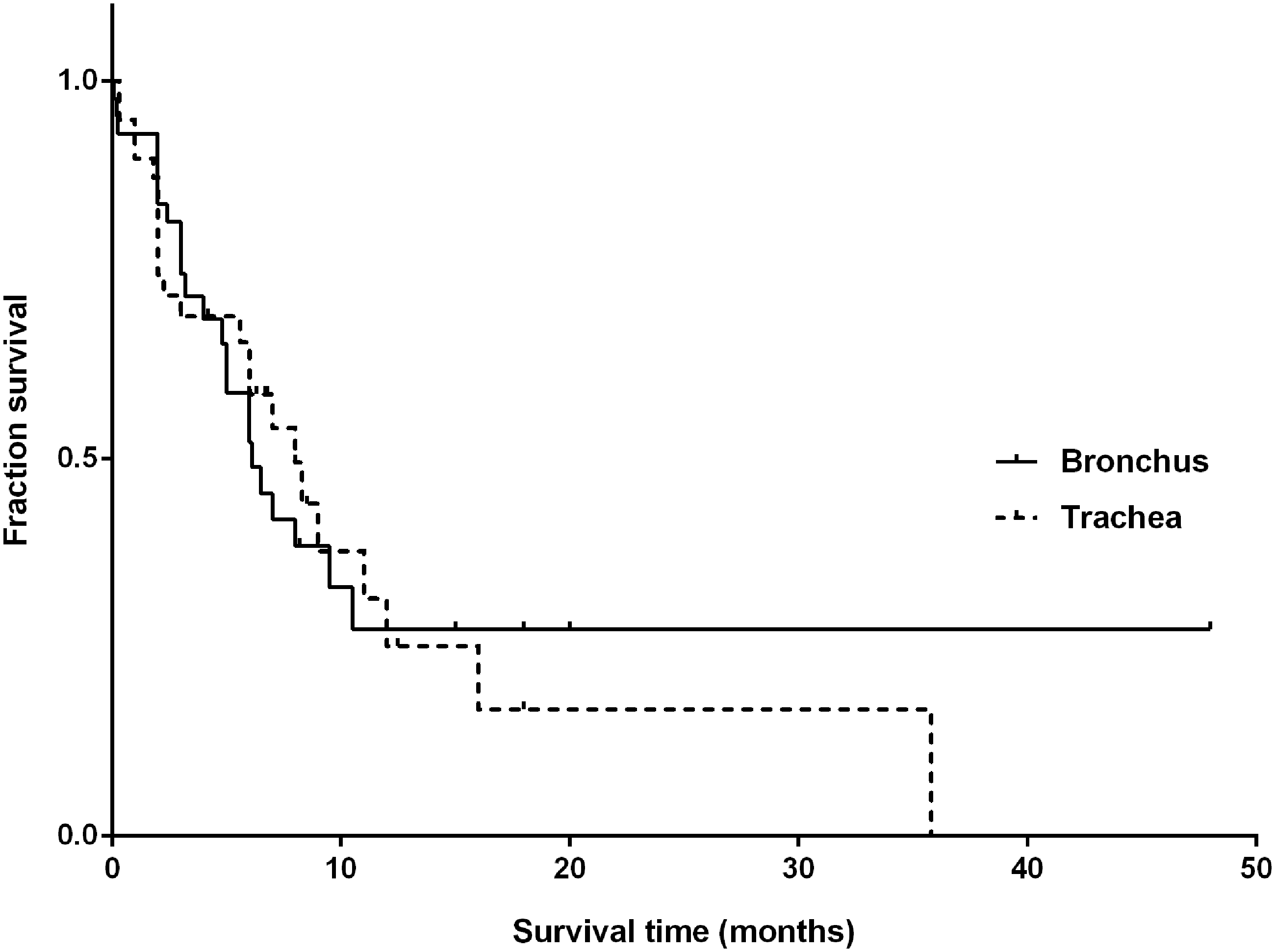
Survival curves of patients with fistulas located in the bronchus and trachea.
Discussion
In this systemic review, cough was the main clinical presentation of TGAF. Bronchoscopy and multi-slice CT (MSCT) played important roles in confirming a diagnosis in patients with suspected TGAF. The management strategies mainly depended on the general condition of the individual patients.
TGAF may occur early or late, and its causes vary. Early TGAFs arise from extensive dissection, vessel manipulation, or ischemia. Early TGAFs mainly involving esophageal anastomosis leakage, including mechanical fistulas, are usually discovered within the first 2 days after surgery, while classic ischemia anastomosis leakages commonly appear 5 to 6 days postoperation. 11 They usually form between the adjacent stomach wall due to ischemic necrosis caused by stomach staples. The excessive separation and destruction of the mediastinal blood supply of the trachea and main bronchi also contribute to the formation of fistulas. 12 Late TGAFs mostly occur as a result of non-healing ulcers of the gastric conduit, anastomotic leaks, inflammation, infection, iatrogenic trauma, radiotherapy, or tumor recurrence after esophagectomy.11,12 The process of late fistula formation may involve perforation of the stomach wall by the ulcer of the gastric conduit, and subsequent damage to the tracheal wall by the gastric fluid. Alternatively, the stomach tissue may not be able to tolerate the dosage of radiation for esophageal cancer, resulting in fistula formation as a result of radiation injury. Finally, the tumor may erode the stomach wall or tracheal wall, promoting inflammation, infection, and abscess, and eventually causing a fistula.13,14
Clinical diagnosis is usually made based on the presentation of classical symptoms, including cough in a recumbent position or in association with oral food intake, while imaging evidence may be needed to help make a diagnosis in patients with atypical symptoms. TGAF should be suspected in patients with cough, fever, dyspnea, hemoptysis, or pneumonia following esophagectomy. Medical imaging evidence from bronchoscopy, gastroscopy, MSCT, or Gastrografin is needed to confirm the accuracy of the diagnosis, with TGAF being diagnosed when an abnormal connection between the thoracic stomach and airway is observed. Bronchoscopy can clearly show a small fistula and its location, while MSCT can reveal the diameter of the tracheobronchus and the conditions surrounding the fistula in the mediastinum. Both imaging methods are useful for treatment, including surgical and non-surgical treatments. However, gastroscopy is not necessary. In one case, the patient was inappropriately diagnosed with pneumonia because the operator failed to observe a small fistula hidden by hemiplication of the gastric fundus during esophagogastroscopy, 6 and the fistula was eventually detected by bronchoscopy.
Preservation of lung function and fistula occlusion are fundamental to the treatment of TGAFs. Oral food intake is forbidden to prevent the gastric contents from flowing into the airway and worsening the function of the lungs. Antibiotics and parenteral nutrition are also needed. Conservative treatment is also a possible option. Hugin et al. 15 reported on the successful cure of a gastrobronchial fistula between the right intermediary bronchus and the esophagogastric anastomosis using ventilation maintained at low airway pressures, combined with a partially covered wall flex stent placed in the esophageal and gastric remnant. Non-surgical treatment could effectively occlude the fistula and act as a bridge treatment, and the application of a tracheal stent could improve the patient’s general condition before the trachea is suitable for surgical repair. Tracheal stent placement, and other non-surgical methods, also provide good palliative treatment and possible long-term solutions for patients with no indication for surgery but who are eager to alleviate the related symptoms.12,16 However, surgical repair is a definitive treatment with a better survival rate than tracheal stent placemen. Surgery also has fewer complications because of the lack of devices left in the body, while device placement can lead to massive bleeding, hemoptysis, asphyxia, and death.16–18 Notably, surgery can be performed if non-surgical treatment fails, if the patient’s general condition is suitable.8,9 The median survival duration was significantly higher among patients who underwent surgical repair compared with those who received tracheal stents. However, patients who received tracheal stents in some studies were not candidates for surgical repair, which may explain this difference. All three treatment strategies have specific advantages and supplement each other (Figure 4), and the choice of treatment needs to take account of the individual patient’s condition.

Relationships among conservative treatment, non-surgical treatment, and surgical repair. TGAF, thoracogastric airway fistula.
The main limitation of the current study was the small sample size. Most studies did not report the fistula size, which plays an important role in the patient’s prognosis. Early diagnosis and treatment can alleviate patient suffering and improve their quality of life. However, whether an early diagnosis can improve the patient’s lifespan and prognosis remains to be determined.
In conclusion, TGAF should be strongly suspected in patients with persistent cough, especially when in a recumbent position or in association with oral food intake. Bronchoscopy and MSCT are recommended to confirm the suspected diagnosis. In terms of the treatment strategy, non-surgical treatment can provide a better initial fistula closure rate, but surgical repair is associated with a better survival rate. Individualized treatment should be adopted based on the general condition of the patient.