
Abstract
Objective
To compare the sternal fixation effect of a polyetheretherketone (PEEK) cable product and stainless steel wire after median sternotomy.
Methods
A multicentre retrospective clinical trial was conducted in patients that underwent median sternotomy for a range of surgical reasons. The sternum was fixed using PEEK sternal cables in the experimental group and stainless steel wires in the control group. The general patient state, product manoeuvrability, bone and wound healing state and blood test results were evaluated at seven visits during the preoperative, surgical and follow-up periods.
Results
A total of 108 patients (54 in each group) were included in the analysis at the final 180-day follow-up. The sternum was successfully closed using PEEK cables or steel wires in all patients and all healed well. No pathological changes were found on the X-ray imaging. Computed tomography imaging confirmed ideal fracture healing. No significant difference was found between the experimental group and the control group in outcomes.
Conclusion
PEEK cables are easy to implant and show desirable effectiveness in sternal fixation without any observed side-effects.
Introduction
Despite the evolution of minimally invasive surgeries and interventional techniques, median sternotomy is currently the most common approach in cardiac surgery. The conventional procedure of sternum fixation uses stainless steel wires. However, the latest studies have revealed that this approach may increase the risk of sternal dehiscence, pulmonary dysfunction, chest wall discomfort and mediastinal infection. 1 Multifragmentary fractures of the sternum can result from high-energy trauma, which is a life-threatening injury and often results in local trauma to soft tissues. 2 Preoperative risk factors, including obesity, chronic obstructive pulmonary disease, New York Heart Association functional class III/IV, osteoporosis, immunosuppression and previous sternotomy, all increase the risk of sternal dehiscence.3,4
Different methods for sternal fixation, including different suture patterns, different steel wire quantities and novel titanium devices, have been tested to reduce mortality, morbidity, hospital stay, overall costs and psychological distress.4–8 However, metallic implants may increase the inconvenience for some patients in the scenario of magnetic resonance imaging scans, security checks and personal privacy. Polyetheretherketone (PEEK) is a polyaromatic thermoplastic polymer with satisfactory biocompatibility and mechanical properties that has already been widely used in various surgical fields, including spine surgery, orthopaedic surgery and maxillo-facial surgery. 9 A novel sternal fixation product consisting of a PEEK cable and a stainless needle was designed to provide an alternative sternal fixation method. This multicentre clinical trial was retrospectively conducted to evaluate the safety and effectiveness of this PEEK sternal fixation system.
Patients and methods
Study design and population
This multicentre, single-blinded, retrospective clinical trial enrolled patients suitable for median sternotomy in the Department of Cardiovascular Surgery, First Affiliated Hospital of Xi‘an Jiaotong University, Xi’an, Shaanxi Province, China and the Department of Cardiovascular Surgery, Shaanxi Provincial People’s Hospital, Xi’an, Shaanxi Province, China between May 2015 and September 2017. Two parallel groups were divided at a ratio of 1:1. The inclusion criteria were as follows: (i) patients suitable for median sternotomy; (ii) patients without skin irritation; (iii) patients aged 18–65 years; (iv) full legal competence; (v) written informed consent provided. The exclusion criteria were as follows: (i) presence of severe systemic infection or severe systemic disorders; (ii) history of allergies; (iii) severe osteoporosis; (iv) pregnancy, preparing for pregnancy or currently breastfeeding; (v) severe mental health disorders; (vi) misuse of drugs, cigarettes or alcohol; (vii) participation in other interventional trials within previous 3 months; (viii) expected non-compliance with the requirements of the trial. The reporting of this study conforms to the STROBE statement. 10
This study protocol was approved by the Medical Ethics Committee of Shaanxi Provincial People’s Hospital (no. 2015-X006) and the Ethical Committee of the First Affiliated Hospital Xi’an Jiaotong University (no. ywllsl-2015-029-01). The study was conducted in accordance with the Declaration of Helsinki. All study participants provided written informed consent before inclusion in the study.
Perioperative protocol
General anaesthesia was administered to all patients prior to surgery and routine perioperative antibiotic prophylaxis was administered. Further antibiotic therapy was given based on serum infection markers and antimicrobial susceptibility tests. All patients were draped in a standard manner and the skin was incised with a scalpel. The subcutaneous tissue was dissected by electrocautery. The median sternotomy was performed in the standard manner using an electrosternum saw and bone wax was applied along the sternal fracture surface.
After the heart surgery, the sternum was closed using PEEK sternal cables (Kontour Medical Technology, Xi'an, China) in the experimental group and stainless steel wires (M649; Ethicon, Raritan, NJ, USA) in the control group (Figure 1). Monofilament surgical stainless steel sutures were applied (size 6, 0.8 mm diameter) with a V-40 (tapercut 1/2 circle) needle. This type of stainless steel suture is regularly used in sternal fixation. 11 In the experimental group, after placing it around the sternum, the needle of the PEEK sternal cable was removed, and the tail of the cable was inserted into the lock at the head of the cable. Then, the cable was tightened with a specially designed device until a suitable tension was reached and the redundant part of the cable was discarded. Any operational inconvenience was documented, including appearance defects, cable ruptures, operational difficulties and failure. Mediastinal drilling tubes were inserted in all patients. The subcutaneous tissue was closed with running absorbable sutures and the skin was closed with running intradermal sutures. The research group designed a 3-point scale for doctors to evaluate the manoeuvrability of this closure system: 2 = easy manoeuvrability; 1 = regular manoeuvrability; 0 = poor manoeuvrability.

Representative three-dimensional imaging of sternal dehiscence with steel wire fixation.
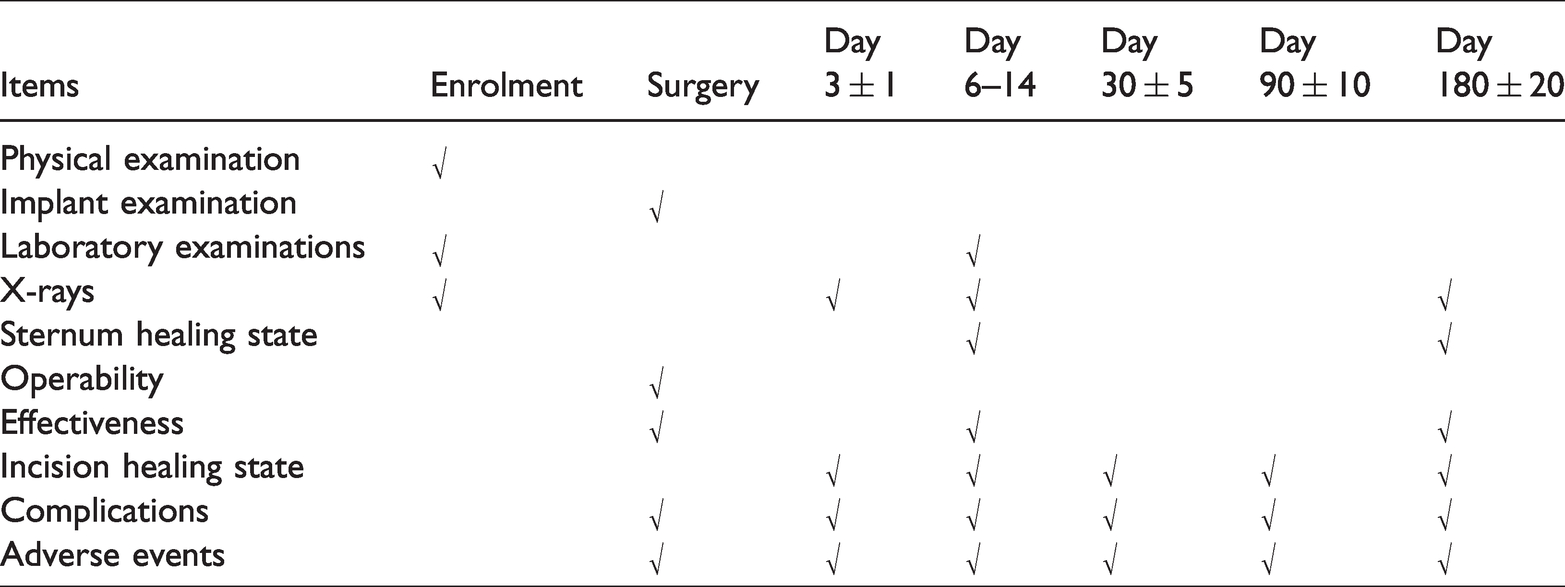
The follow-up period was 180 days. In addition to a preoperative assessment and the surgical procedure, five post-surgical follow-up visits were planned to assess the outcomes at 3 ± 1 days, 6–14 days, 30 ± 5 days, 90 ± 10 days and 180 ± 20 days after the surgery (Table 1). Physical examinations, laboratory examinations (routine blood tests, liver and kidney function tests) and X-rays were performed at each follow-up visit. Computed tomography (CT) imaging was used as required to assess the sternum healing state.
Standard follow-up protocol items used in this multicentre clinical trial that retrospectively evaluated the safety and effectiveness of a polyetheretherketone sternal fixation system compared with steel wire fixation.
The sternum healing state was evaluated using the following 4-point scoring system: 4 = no tenderness, no abnormal sternal displacement, no PEEK cable rupture or deformation, continuous bone callus or no osteotomy gap in the X-ray images; 3 = slight tenderness without abnormal sternal displacement, slight PEEK cable rupture or deformation without functional compromise, discontinuous bone callus or a fuzzy osteotomy gap in the X-ray images; 2 = tenderness without abnormal sternal displacement, slight PEEK cable rupture or deformation without functional compromise after medical therapy, discontinuous bone callus or a fuzzy osteotomy gap in the X-ray images; 1 = tenderness with abnormal sternal displacement, severe PEEK cable rupture or deformation, observed osteotomy edges and a widened gap. 12
Based on the revised Vancouver Scar Scale, the wound healing state was scored as follows: 1 = well healed without redness, swelling, exudation, effusion or infection around the incision; 0 = local redness, swelling, exudation, effusion or infection around the incision. 13 Severe complications, including sternal dehiscence, subcutaneous hydrops, marrow cavity haemorrhage and infection, were classified as invalidating the use of this product.
Statistical analyses
The sample size was based upon the product efficiency data reported from a pilot study. Assuming an alpha of 0.05 and a power of 0.9, the necessary sample size per group was 46. To account for the anticipated 15% attrition, the final sample size needed was 54 per group. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA). The distribution of the data was evaluated. Normally distributed continuous variables are presented as the mean ± SD. Categorical variables are presented as frequencies and percentages. Wilcoxon signed-rank test was used to test sternal healing at postoperative days 6–14 and the intraoperative manoeuvrability of the PEEK cable between the two groups. Student’s t-test was used to compare the wound healing state and the clinical laboratory results between the two groups. A P-value <0.05 was considered statistically significant.
Results
This multicentre, single-blinded, clinical trial retrospectively collected 108 participants in two medical centres without any exclusion, attrition or death. The demographic and clinical characteristics of the two groups are listed in Table 2. Other than age (P = 0.03 compared with the control group), there were no significant differences between the experimental and control groups. The participants underwent surgeries including coronary artery bypass grafting, valvular replacement or repair, congenital heart disease repair and other cardiovascular surgeries. All PEEK cables and steel wires were successfully implanted in all patients without defects, cable rupture, operational difficulties or failure (Figure 2). Manoeuvrability scored 2 in 53 of 54 patients (98.1%) in the experimental group and 49 of 54 patients (90.7%) in the control group. None of the doctors gave a manoeuvrability score of 0 for any of the patients. No abnormal incidents occurred during any of the surgical procedures.
Baseline demographic and clinical characteristics of patients (n = 108) enrolled in this multicentre clinical trial that retrospectively evaluated the safety and effectiveness of a polyetheretherketone sternal fixation system compared with steel wire fixation.

Data presented as mean ± SD or n of patients.
*P = 0.03 compared with the control group; no other significant between-group differences (P ≥ 0.05); Student’s t-test.

Representative sternal fixation using polyetheretherketone cables. The colour version of this figure is available at: http://imr.sagepub.com.
During the follow-up period, all participants recovered well, except for one patient in the control group that experienced subcutaneous lipoliquefaction at day 7 postoperatively and was discharged after effective therapies. No abnormalities and no significant differences were found in the physical examinations, blood cell tests or biochemical profiles at the last visit. No pathological changes were found on the X-ray imaging and the PEEK cables could not be detected on the X-ray images. Some patients in the experimental group received an additional CT scan at the last visit; and three-dimensional CT imaging at day 180 postoperatively showed that the cables were placed around the sternum without rupture or displacement and that the bone presented a satisfactory healing state, without malunion, fracture or dehiscence (Figure 3).

Representative three-dimensional imaging of the sternum and the polyetheretherketone cable at postoperative day 180. The colour version of this figure is available at: http://imr.sagepub.com.
Discussion
With a reported incidence of 0.2% to 5%, sternal dehiscence may result in sternal malunion, mediastinitis and poor wound healing.4,14–17 Based on our clinical experience, achieving a suitable tension of conventional steel wires is difficult, and an inappropriate tension may cause wire breakage and lead to sternal instability, sternal fracture, and even sternal dehiscence, especially for certain patients, such as those with severe osteoporosis or obesity, or children. 18 The size 6 stainless steel suture is 0.8 mm in diameter and is able to provide enough support for the sternum. However, the stainless steel may break due to inappropriate tension because the fixation process requires experience for the surgeon to find a suitable tension. 11 In the experimental group, the fastening device was designed to prevent surgeons from pulling the PEEK cable too tight, which made it easier to apply the fixation cable with ideal tension. Additionally, metal artefacts in imaging scans may increase the diagnostic difficulties in the future. The ideal material for sternal closure should be simple, inexpensive, stable and biocompatible. PEEK is a highly biocompatible material that has been widely used in medical implant products. 9
Coughing is a common symptom after receiving heart surgery and helps expectorate the patient’s airways. Previous research has demonstrated that the internal distending pressure may reach 40 kPa on all sides during maximal coughing. 19 Roughly calculated based on the formula ‘F = P · S’, this means that the force acting on the sternum may reach 384 N as the length and width of the sternum may reach 160 mm and 60 mm, respectively. 20
Based on these details and the biomechanical properties of the PEEK cables, three to five cables would be suitable to provide enough mechanical support for the sternum. In this current trial, the surgeons found that the specially designed cable and fastening device were easy to operate and achieved a suitable tension. The cable can only be pulled in one direction, and when reaching a suitable tension, the specially designed fastening device can restrain the operator from pulling it tighter. In addition, the PEEK cable is much wider than the steel wire, increasing its osseous contact area. The wider design aims to avoid concentrated local forces on the bone, improve sternal stability, relieve pain as the tension increases and reduce the possibility of sternal dehiscence. During the follow-up, all patients achieved satisfactory sternal stability and no postoperative complications were reported in the experimental group. This work showed that the PEEK cable was a favourable option for sternal closure in typical patients.
This current study had several limitations. First, PEEK is a non-absorbable biocompatible material that permanently implants fixation cables in the body. It provides long-term support, especially for those with a high risk of sternal dehiscence, but its presence may cause uncomfortable feelings after full sternum healing in some patients. Secondly, because the PEEK cable is wider than the stainless steel wire, patients with thin subcutaneous tissues may be able to palpate the cable through the skin. For those patients that are upset about the presence of implants, removal surgery after full healing may be an option. Thirdly, although the 180-day follow-up period revealed a satisfactory result, a longer follow-up is necessary for a more comprehensive assessment.
In conclusion, the PEEK sternal fixation system was easily manipulated and could provide satisfactory mechanical support for sternal healing.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Key Research and Development Program of Shaanxi province (no. 2020ZDLSF04-11).