
Abstract
We performed a retrospective analysis of the clinical manifestations, laboratory and imaging examinations, treatment, and prognosis of a male infant who was diagnosed with mediastinal and subglottic hemangioma in our hospital. The clinical features of this patient were coughing, wheezing, and dyspnea. Enhanced computed tomography of the neck and chest showed a diffuse abnormality in the right-upper mediastinum. He was diagnosed with a hemangioma after a physical examination combined with bronchoscopy. The clinical symptoms were relieved by oral propranolol. We also investigated the clinical characteristics, treatment, and prognosis of mediastinal and subglottic hemangioma in infants in the previous literature, and searched for case reports of this disease in China and in other countries. We only identified three previous cases of mediastinal and subglottic hemangioma in infants, indicating that this condition is rare. In the proliferative stage, surrounding organs and tissues are compressed, which can be life-threatening. Most of these children develop wheezing, shortness of breath, dyspnea, cyanosis, and other symptoms within 2 months. Enhanced computed tomography and magnetic resonance imaging combined with soft bronchoscopy can confirm the diagnosis of this disease, and oral propranolol achieves a favorable effect.
Keywords
Introduction
Infantile hemangiomas (IHs) are the most common tumors in infants, accounting for 4% to 10% of tumors. 1 According to the location, this disease is primarily divided into superficial, deep, and mixed IHs, with incidence rates of 65%, 15%, and 20%, respectively. Case reports of mediastinal and subglottic hemangiomas in infants in China or in other countries are rare. Although these cases can be clearly evaluated and diagnosed by non-invasive methods, they are easily misdiagnosed or missed because the clinical manifestations of this disease are non-specific. Most patients with mediastinal and subglottic hemangiomas have a good prognosis when they are diagnosed early and receive timely treatment with oral drugs. However, the mortality rate in these patients is high when the diagnosis and treatment are delayed. 2
We report the clinical manifestations, laboratory and imaging examinations, treatment, and prognosis of a male infant who was diagnosed with mediastinal and subglottic hemangioma in our hospital. Additionally, to improve the awareness and understanding of mediastinal and subglottic hemangioma, we (i) summarized and analyzed the characteristics of the progress of this disease, as well as diagnosis and treatment, in four cases in infants; and (ii) summarized its etiology and pathogenesis.
Methods
Case presentation
A full-term male neonate was born by cesarean section owing to an incorrect fetal position on 6 December 2019, with a birth weight of 3.35 kg. He was admitted to a local hospital because of wheezing on 20 January 2020 (1 month and 20 days after birth) and underwent assisted mechanical ventilation due to his worsening condition. Seven days later, he was transferred to the Children’s Intensive Care Unit of Hainan Women and Children’s Medical Center owing to his inability to be weaned off the ventilator. After treatment with anti-infective medications and methylprednisolone as an anti-inflammatory agent, the infant was successfully withdrawn from the ventilator and discharged when his symptoms began to improve. However, the infant began wheezing again 1 week after being discharged. He then showed shortness of breath and inspiratory dyspnea, and he was admitted to our hospital again on 6 March. A physical examination showed a temperature of 36.6°C, respiratory rate of 50 breaths/minute, pulse rate of 136 beats/minute, and weight of 7.2 kg. He was conscious and active, and his reactions were normal. He manifested superficial lymph nodes that were not palpable or enlarged, a pharynx that was slightly congested, an inspiratory tri-concave sign (+), and marked breath sounds in both lungs. Wheezing sounds were also heard. His heart, abdomen, and nervous system were normal.
After admission, an enhanced computed tomography (CT) scan of the neck and chest showed the following: (i) diffuse abnormal enhancement in the right-upper mediastinum, (ii) enlarged vessels and an enlarged paratracheal region of the neck with an undetermined cause, and (iii) an obviously compressed and narrowed subglottic area and trachea (Figure 1). Magnetic resonance imaging (MRI) showed a space-occupying lesion with a rich blood supply in the right-upper mediastinum surrounding the large vessels. This lesion protruded locally to the trachea to form a mound-like protrusion, and a narrowed and compressed trachea, which suggested a hemangioma. Neck B-ultrasound showed a hypoechoic mass in the lower part of the neck that suggested a hemangioma (4.4 × 2.3 × 3.3 cm3). An electrocardiogram showed an incomplete right bundle branch block. Electronic bronchoscopy showed that the subglottic airway was compressed and deformed, with the main airway obviously narrowed. At the 6 o’clock position of the subglottic area, there was a raised tissue area that was red and rich in blood vessels. We considered that this abnormality was bronchial stenosis (or subglottic hemangioma) (Figure 2).
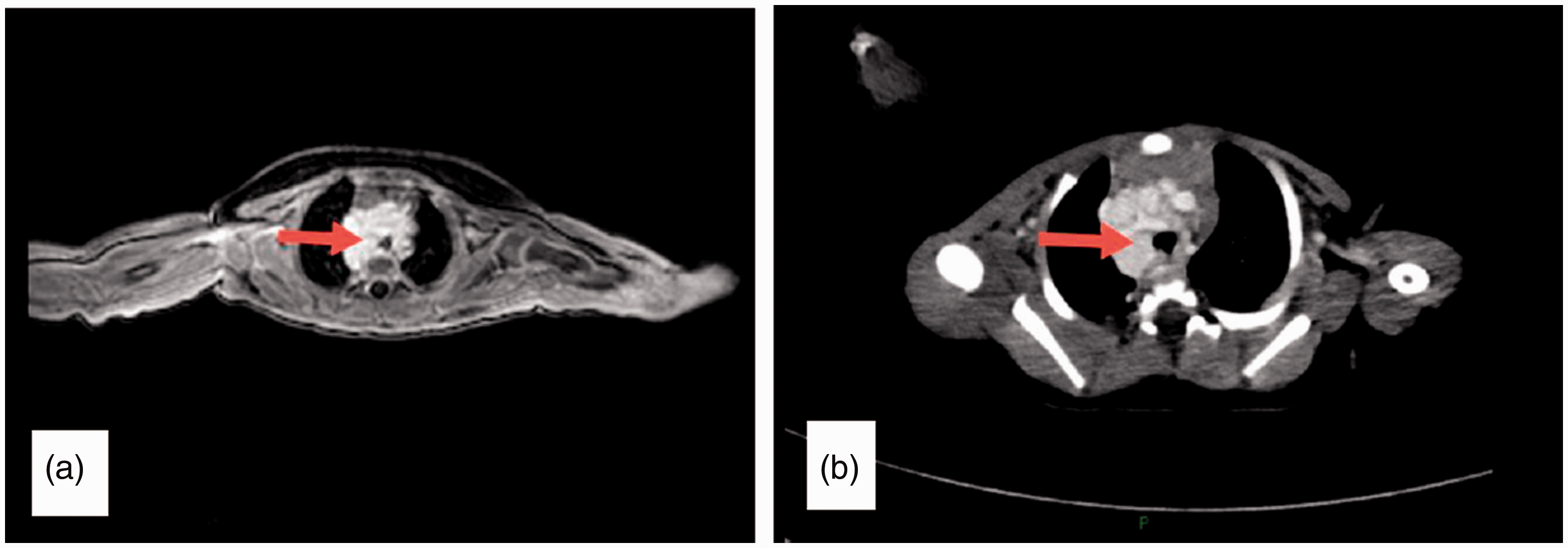
(a) Enhanced magnetic resonance image of the neck showing a hemangioma, with the enhanced signal demonstrating compression of the trachea (red arrow). (b) Enhanced computed tomographic image of the neck showing a hemangioma, with the enhanced signal showing the hemangioma surrounding the trachea and protruding toward the distal airways (red arrow).

(a) Soft bronchoscopy under local anesthesia shows that the trachea is compressed and deformed. (b) Soft bronchoscopy under local anesthesia shows that the trachea is occupied by a mass of blood vessels.
An examination of blood indices showed no abnormalities in routine blood, liver, or kidney function tests, myocardial enzymes, or coagulation. Four analyses of Mycoplasma pneumoniae and Chlamydia showed the following. The M. pneumoniae immunoglobulin G level was 46.10 AU (arbitrary units)/mL and the M. pneumoniae immunoglobulin M level was 1.38 COI (cutoff index). All Chlamydia examinations were negative. Azithromycin was administered orally as an anti-infective agent, and oral propranolol, budesonide, and acetylcysteine in a nebulized form for inhalation were administered. The child’s wheezing was relieved after 3 days of medication. After 1 week, his symptoms were significantly relieved, and wheezing could only be heard by auscultation after he moved, but not when in a quiet state. Re-examination of liver function indicated that the alanine aminotransferase level was elevated (45 U/L), and blood glucose levels, blood pressure, and heart rate were within the normal range. Propranolol was administered at 2 mg/kg. The final diagnoses after discharge were (i) mediastinal and subglottic hemangioma, (ii) bronchial stenosis, (iii) lung infection, and (iv) complete right bundle branch block. A re-examination of the neck by B-ultrasound 1 month after discharge showed that the hemangioma had shrunken to 15 × 12 × 28 mm3. Additionally, liver and kidney function indices, blood glucose levels, and blood pressure remained in the normal range. A portable pulse oximeter (Philips DB12; Suzhou Erda Medical Equipment Co., Ltd., Suzhou, China) used at home for monitoring showed that heart rate and blood oxygen were in the normal range. The boy was followed up for 8 months, and the dose of propranolol was reduced to 1 mg/kg. During this period, blood glucose levels and liver and kidney function were tested every 2 to 3 months and they were normal. A re-examination of color Doppler ultrasonography on 10 December 2020 showed that the size of the hemangioma was 5.3 × 7.0 × 12.8 mm3 and that the clinical symptoms had disappeared completely. The reporting of this study conforms to the CARE guidelines. 3
Literature review
We searched the English medical literature using PubMed, Springer Link, and Elsevier databases. We used the following search queries for PubMed. When we searched for “subglottic hemangioma and infant,” we retrieved 34 relevant reports, for “mediastinal hemangioma and infant” we retrieved 5 reports, and for “subglottic and mediastinal hemangioma and infant or child” we retrieved 3 reports. Relevant Chinese reports were found in the WanFang and CNKI databases. Using the search query “subglottic or mediastinal hemangioma and infants or child” we retrieved 147 relevant reports in these databases. However, we found no articles when searching for “subglottic and mediastinal hemangioma and infant or child.” After carefully reading all of these articles, we found three previous cases. 1 , 4 , 5 When we combined the data from the current case and the previous cases, we found that the age at diagnosis was ≤6 months in all patients, one patient was a boy, and three were girls. One case was a premature infant at 34 weeks of gestation. All four infants had symptoms, such as inspiratory dyspnea, wheezing, or cyanosis during crying. One infant showed difficulty in feeding, one showed gastroesophageal reflux, and one manifested accompanying symptoms of superficial hemangioma. The latest diagnosis was made a few months after the symptoms first appeared. Regarding treatment, two infants underwent surgery (one underwent laser ablation and subglottic hemangioma resection and one underwent glottoplasty) and all four infants improved with oral propranolol. This information is summarized in Table 1.
Clinical manifestations, signs, treatment, and prognosis of subglottic and mediastinal hemangioma in four infants.
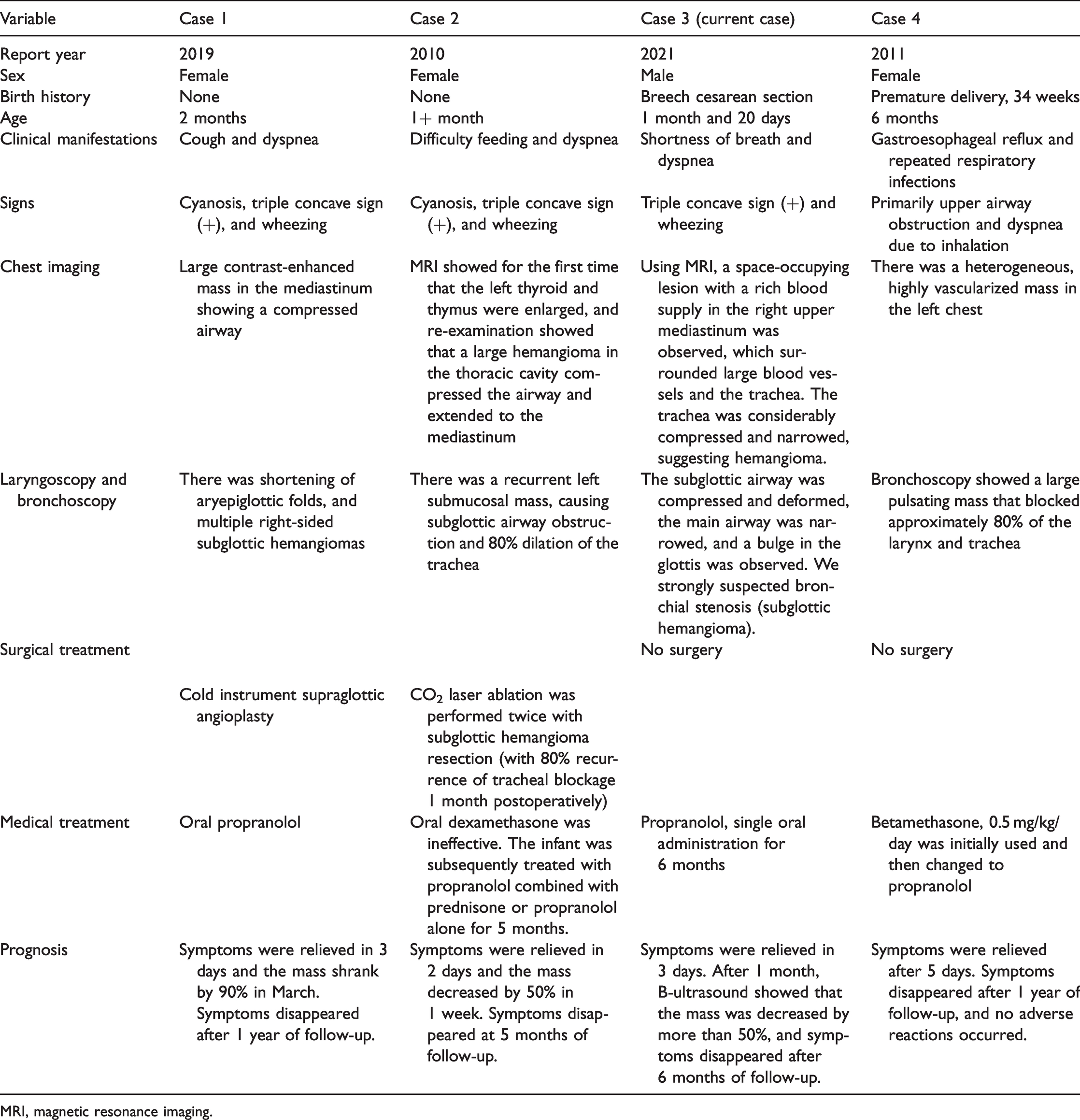
MRI, magnetic resonance imaging.
Discussion
Hemangioma is a commonly observed benign vascular neoplasm. 6 IHs are among the most common soft tissue tumors that occur in infancy. 7 IHs are congenital benign tumors derived from vascular endothelial cells, with different clinical manifestations because of the variety of growth sites. IHs are usually classified as superficial, deep, or mixed, depending on the location. The growth characteristics of IHs follow the growth patterns of skin hemangiomas, which rapidly proliferate at 1 to 3 months, and degenerate at approximately 1 year old. 8 , 9 There are two primary mechanisms that cause the degradation and neovascularization of hemangiomas. (i) Mechanisms underlying angiogenesis comprise the de novo formation of vessels from pre‐existing vessels. This vessel formation is accomplished by degradation of the basement membrane, migration of endothelial cells, tubulogenesis, and recruitment of perivascular cells. (ii) Mechanisms of vasculogenesis entail the growth of new blood vessels from stem cells or progenitor cells. Hemangioma progenitor/stem cells, endothelial cells, and pericytes are the main cells involved in the pathogenesis. The molecular basis of IH involves genetics, vascular endothelial growth factor and its receptors, angiopoietins and Tie2, the Notch pathway, the mammalian target of rapamycin pathway, and other pathways. 10
Subglottic hemangioma is a benign infantile tumor, and the growth of subglottic hemangiomas only accounts for 1.5% of congenital abnormalities. Subglottic hemangioma is relatively rare, but life-threatening, when unrecognized or untreated, and the rapid growth of airway IHs may lead to complete obstruction of the airway. The incidence of mediastinal hemangioma is lower than 0.5%. Mediastinal hemangioma is usually asymptomatic and discovered accidentally via imaging, but it may manifest as non-specific symptoms, such as chest pain, shortness of breath, dyspnea, and dysphagia. 11 Few children with subglottic hemangioma have combined mediastinal hemangioma. In these rare cases, the airway is first narrowed owing to the endogenous space-occupying property of the subglottic hemangioma, and it is further narrowed because of growth of the mediastinal hemangioma and external pressure. This condition becomes life-threatening if it is not discovered in a timely fashion. Therefore, subglottic combined with mediastinal hemangioma presents a monumental challenge for clinicians in the evaluation of children with respiratory distress.
The age at symptom onset of hemangiomas in the mediastinum and subglottis is typically ≤2 months, and its incidence is related to premature birth, multiple births, female sex, and low birth weight. 12 Our literature review included three cases in which the three infants were girls. 1 , 4 , 5 These three infants developed symptoms of hemangiomas within 2 months. The child treated at our hospital was delivered by cesarean section owing to an incorrect fetal position, and there were no high-risk factors present.
Our literature review of mediastinal and subglottic hemangioma showed that clinical manifestations were non-specific and primarily included coughing, wheezing, shortness of breath, dyspnea, feeding difficulties, gastroesophageal reflux, and repeated respiratory infections. Additionally, the longest time from symptom onset to diagnosis was several months, indicating that this disease is easily misdiagnosed or missed. The present case was a child who was admitted to our hospital owing to symptoms, including phlegm, breathlessness, and shortness of breath, but he had no vomiting or feeding difficulties. He had symptoms on 20 January, which were temporarily relieved by treatment with methylprednisolone because of difficulty in weaning him off the ventilator. This treatment may have temporarily inhibited the growth of the hemangioma, and he was discharged after relief of his symptoms. However, more severe wheezing reappeared 1 week after discharge, and the diagnosis was confirmed by spiral CT, soft bronchoscopy under local anesthesia (Figure 1), MRI, and B-ultrasound.
Subglottic hemangioma is relatively common, and ultrasonography combined with local anesthesia under soft bronchoscopy can confirm its diagnosis. However, mediastinal hemangioma is rare, and a combination of spiral CT, MRI, and other related examinations are recommended to further clarify the situation and avoid a missed diagnosis. MRI shows the different components and vasculature of IHs because of its high contrast resolution, tissue characterization capabilities, good spatial resolution, and wide field-of-view. Disadvantages of MRI include the requirement for user expertise, a long scanning time, and contraindications, such as metallic devices. CT has wide applicability, a short turnaround time, high isotropic spatial resolution, a wide field-of view, and multiplanar reconstruction capabilities. Chest CT shows high sensitivity in detecting calcification and phleboliths, which are a feature of IHs. Therefore, using a combination of these modalities is recommended. 13
Propranolol is rapidly becoming the standard of care for treating subglottic hemangiomas. 14 Despite widespread adoption of this treatment, the rarity of this condition has limited previous studies to only case reports and small series. There are no evidence-based guidelines for proper dosing of propranolol or the duration of treatment. Despite the inherent limitation of a relatively small sample size in our literature review, it suggests that concurrent steroid use with propranolol does not decrease the rate of treatment failure. Based on current evidence, we recommend a dosage of 1 to 3 mg/kg/day, starting with 1 mg/kg/day, and increasing the dosage incrementally. Treatment can be continued through at least 12 months of age, and possibly up to 18 months, depending on the proliferation characteristics of individual patients. 2 Propranolol has few side effects, which may include bradycardia, hypotension, and hypoglycemia. Other potential side effects of propranolol include bronchospasm, fatigue, nightmares, heart failure, and peripheral vasoconstriction. 15 We also emphasize the importance of follow-up of patients with mediastinal and subglottic hemangioma.
In our case, oral propranolol was administered immediately after the diagnosis was confirmed, with an initial dose of 1 mg/kg, and within 1 week we slowly increased the dose to 2 mg/kg. Symptoms were relieved after 3 days of propranolol treatment, and wheezing was reduced. After 1 week, when the patient was in a quiet state, no dyspnea or wheezing was observed. The child has now been followed up for 8 months, and the propranolol dosage has been reduced to 1 mg/kg/day. During this period, blood glucose levels, and liver and kidney function were reviewed every 2 to 3 months, and no obvious abnormalities were found. A recent CT scan showed that the hemangioma had almost disappeared, and the clinical symptoms had disappeared completely. In the other three cases in our literature review, the symptoms were relieved after several days of taking propranolol and there were no severe complications.
Before propanol became widely used, oral glucocorticoids were the first-line treatment for IH. Glucocorticoids can cause serious adverse reactions (e.g., personality changes [irritability], cushingoid facies, growth retardation, and increased risk of infection.). Therefore, oral use of glucocorticoids is currently limited to severe and refractory IH (e.g., IH with thrombocytopenia) or cases of failure of beta-blocker treatment in IH. The optimal dosage of an oral glucocorticoid is 2 to 3 mg/kg/day and the typical treatment schedule is 4 to 12 weeks of full-dose treatment, with a gradual reduction in dose. 16 In our literature review, two of the four cases did not improve after treatment with oral dexamethasone, but improved after the use of propranolol only or propranolol combined with glucocorticoids. The indications for surgical treatment are as follows: (i) a large hemangioma remaining on the face, which may affect the appearance; (ii) propranolol contraindications, intolerance, or insensitivity; (iii) no reduction in the tumor after conservative treatment and the possibility to perform surgery during the regression period; 17 and (iv) hemangioma growth in a special position (e.g., subglottic and mediastinal hemangioma) exerting life-threatening pressure on important organs, in which case immediate surgery is required to relieve the compression.
Among the three cases from our literature review and our case, two cases showed large hemangiomas. One of these cases was treated by cold instrument supraglottic angioplasty and one had CO2 laser ablation and subglottic hemangioma resection. However, because the recurrence rate of tracheal blockage 1 month after surgery is 80%, we emphasize the importance of combining surgery with propranolol and steroids. Clinicians should take note of children with risk factors (e.g., premature birth, multiple births, female sex, and low birth weight) when signs/symptoms of coughing, wheezing, shortness of breath, difficulty in breathing, and difficulty in feeding occur. In such cases, there should be suspicion that airway hemangiomas may be present, and the clinician should complete an airway assessment. Additionally, we recommended not using methylprednisolone without a clear diagnosis to avoid concealing the symptoms and thereby delaying the diagnosis.
Footnotes
Acknowledgment
Author contributions
W.X. and J.C. designed the study and wrote the manuscript. Q.Y.L. and Y.H. collected data and drafted the manuscript. S.C, N.F., Z.M, Y.W., Q.L., X.H., and L.F. contributed to data acquisition and participated in discussions.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved by the Medical Ethics Committee of the Hainan Women and Children’s Medical Center (ethical approval no. 2020-16). A guardian of the child signed informed consent for publication of this case report.
Funding
This study was supported by Hainan Major Science and Technology Projects (No. ZDKJ2019010), and the Key Research and Development Project of Hainan Province (No. ZDYF2020216).