
Abstract
Objectives
To compare the yield of early combined use of chest X-ray (CXR) and chest computed tomography (CT) in patients diagnosed with community-acquired pneumonia (CAP) presenting to the emergency department (ED) and assess the impact of chest CT on the initial diagnosis.
Methods
The medical records of 900 patients who presented to the ED and were diagnosed with CAP over a 1-year period were reviewed, and 130 patients who underwent CXR and chest CT within 48 hours were selected. CXR findings were classified as positive, negative, or inconclusive for CAP. Chest CT findings were defined as positive, negative, inconclusive, or positive with add-on to the CXR findings. CT was classified as having no benefit, large benefit, or moderate benefit based on the chest CT and CXR findings.
Results
Chest CT results were positive in 90.7% of patients, with 41.5% being newly diagnosed after negative or inconclusive CXR and 21.5% being diagnosed with add-on to the CXR findings. CT had large, moderate, and no benefit over CXR in diagnosing or excluding CAP in 45.3%, 21.5%, and 33.1% of patients, respectively.
Conclusion
Early chest CT may be used to compliment CXR in the early diagnosis of CAP among patients in the ED.
Keywords
Introduction
Community-acquired pneumonia (CAP) is associated with a significant disease burden. Early and rapid diagnosis of CAP is crucial for good outcomes in elderly and immunocompromised individuals. The diagnosis of CAP depends on the clinical presentation and radiologic findings. The clinical symptoms include cough (86%), dyspnea (72%), and sputum production (64%) accompanied by one or more of the following: fever, fatigue, myalgia, abdominal pain, diaphoresis, and headache. Chest X-ray (CXR) findings suggestive of CAP include the presence of a new interstitial infiltrate, lobar consolidation, or cavitation. 1
The criteria for diagnosing CAP differ among various guidelines. The American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) guidelines and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines state that the diagnosis of CAP is based on clinical symptoms and CXR features. 2 The British Thoracic Society (BTS) guidelines recommend CXR in all hospitalized patients, when the diagnosis is in doubt, when an unsatisfactory response to treatment has been obtained, or if the patient is considered to be at high risk for an underlying lung pathology such as lung cancer. 3 The Lebanese Society for Infectious Diseases and Clinical Microbiology (LSIDCM) adapts the recommendations of the ATS/IDSA and ESCMID in terms of performing CXR to diagnose or rule out pneumonia when suspected. 4 Furthermore, according to the BTS, chest computed tomography (CT) helps to improve the accuracy of a CAP diagnosis (especially when the diagnosis is in doubt) compared with CXR alone. The ATS/IDSA states that the role of chest CT remains unclear because in cases of unclear or possible CXR findings, observation and empiric antibiotics followed by repeat CXR should be adequate for establishing the diagnosis. 5
Although chest CT is believed to be superior to plain CXR because it provides a rapid and accurate diagnosis,6,7 its role in the diagnosis of CAP is unclear because of its higher radiation dose, elevated cost, and limited bedside availability. 7 However, many new techniques and protocols are being implemented to decrease the radiation dose of CT scans.8,9 Prendki et al. 9 reported that low-dose chest CT helped to exclude the diagnosis of pneumonia in a geriatric population and hence decreased the risk of unnecessary antibiotic administration.
The use of CT for common chest conditions in the emergency department (ED) has markedly increased in the last decade. Chest CT may be of benefit in diagnosing certain individuals with suspected CAP, such as patients with febrile neutropenia, 11 patients with HIV and suspected Pneumocystis jirovecii pneumonia, 12 and elderly bedridden patients. 13 In a recent large prospective study, Claessens et al. 14 evaluated the use of CT in patients with suspected CAP presenting to the ED. They found that CT changed the initial management regarding admission, antibiotic administration, or discharge in 50% of cases. 14 Therefore, we conducted the present retrospective chart review to compare the yield of early CXR and chest CT in patients suspected to have CAP presenting to the ED of a tertiary care center in Lebanon. The objective of our study was to determine the impact of adding chest CT to CXR on the initial diagnosis of CAP.
Methods
This was a retrospective review of the medical charts of all patients who presented to the ED and were diagnosed with CAP from 1 January 2014 to 1 January 2015. We included adult patients aged >18 years who underwent chest CT and CXR for the diagnosis of pneumonia with a maximum of 48 hours between these two modalities. We excluded patients diagnosed with nosocomial pneumonia 48 hours after admission, 15 patients who underwent only one radiological test (either chest CT or CXR), and patients diagnosed with a condition other than CAP that could explain their febrile illness (Figure 1). The CXR findings were identified as positive, negative, or inconclusive for pneumonia. The chest CT findings were defined as positive, negative, inconclusive, or positive with add-on to the CXR findings. The imaging modality (CXR or chest CT) was considered positive for pneumonia when the radiological findings were suggestive of pneumonia, negative for pneumonia when no radiological findings were suggestive of pneumonia, and inconclusive for pneumonia when the radiological findings could not rule out pneumonia. We used the term “add on” for chest CT when the radiological findings were suggestive of pneumonia with additional findings not identified on CXR.

Flow chart of the study.
Chest CT examinations were performed without or with contrast (Omnipaque 350) on Siemens (Munich, Germany) or Philips (Amsterdam, Netherlands) machines. The following parameters were used: thickness, 3 mm; increment, 2 mm; kVp, 120; mAs/slice, 250; evolving standard resolution; collimation, 64 × 0.625; pitch, 1.078; rotation time, 0.75 seconds; field of view, 350 mm; window/level, 360/60; matrix, 512; ACS used; and delay after injection, 30 s. Sagittal and coronal reformats were obtained.
Based on the chest CT and CXR findings, the benefit of CT was divided into three categories: no benefit, significant benefit, and moderate benefit. In the no benefit group, the CT results were similar to the CXR results. In the moderate benefit group, CT provided information in addition to that of positive CXR. In the significant benefit group, CT was positive while CXR was negative or inconclusive, or CT was negative (ruling out CAP) when CXR was inconclusive or positive.
The obtained data were analyzed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including means, standard deviations, counts, and frequencies, were used for the baseline demographic characteristics and other study variables. Group comparisons were performed using analysis of variance for continuous variables as applicable and the chi-square test for categorical variables as applicable. Multivariate analysis was performed using logistic and linear regression.
The Institutional Review Board at the American University of Beirut approved this study before its initiation on 28 September 2017 (approval no. IM.AR-B.15). The reporting of this study conforms to the STROBE statement. 16 Because this was a retrospective chart review, patient consent was not required.
Results
We reviewed the charts of 900 patients who presented to the ED during the 1-year study period and were diagnosed with CAP. A total of 130 patients underwent both CXR and chest CT within 48 hours of admission to the ED. The patients’ mean age was 67 years. The average duration of the hospital stay was 6 days. Among all patients, 90% had comorbidities; these were mainly hypertension (38.1%), diabetes (38.1%), and cancer (35.6%). The overall mortality rate at the end of the hospital stay was 3.1% (Table 1).
Baseline demographic characteristics.
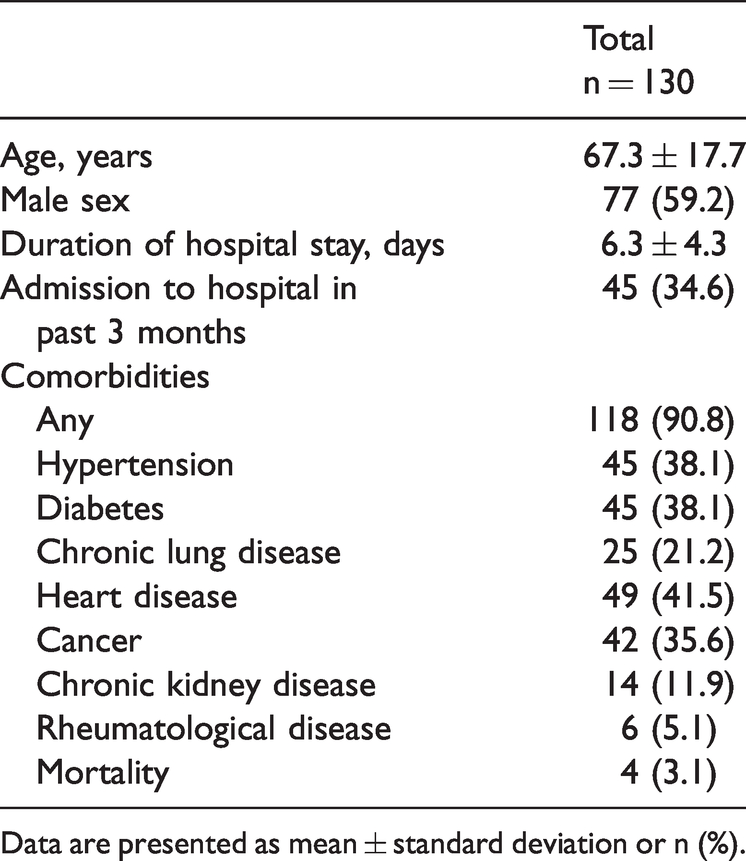
Data are presented as mean ± standard deviation or n (%).
Forty-seven sputum cultures were sent for microbiological investigation; of these, 18 were positive for microorganisms and 29 were negative. Only nine patients had a significant positive microbiology that was thought to be linked to the diagnosis of pneumonia. Relevant positive cultures were as follows: Staphylococcus aureus (n = 3), Haemophilus influenzae (n = 3), Enterobacter cloacae (n = 1), Moraxella catarrhalis (n = 1), and Escherichia coli (n = 1). Chest CT had a significantly higher rate of positive results (90.7%) for CAP diagnosis than CXR (51.5%) (P < 0.0001) (Table 2).
CAP diagnosis using CXR and chest CT.

CAP, community-acquired pneumonia; CXR, chest X-ray; CT, computed tomography.
In total, 45.3% of patients were in the significant benefit group, in which CT diagnosed or ruled out CAP; 21.5% of patients were in the moderate benefit group; and 33.1% of patients were in the no benefit group. The details of these radiological groups are shown in Table 3.
Radiological findings of CXR and chest CT.

CXR, chest X-ray; CT, computed tomography.
Multivariate analysis was performed to identify the demographic factors associated with an increased benefit of chest CT over CXR. We ran a multivariate analysis to assess the relationship between the demographic factors (sex, duration of hospital stay, admission to the hospital in the past 3 months, and comorbidities) and the benefit groups. The results showed that patients with comorbidities had higher odds of being in the significant benefit group than in the no benefit group (odds ratio, 1.98), but without statistical significance (Table 4).
Multivariate analysis of demographic factors associated with increased benefit of chest CT over CXR.

CXR, chest X-ray; CT, computed tomography; OR, odds ratio; CI, confidence interval.
We also compared the patient characteristics among the three groups (large, moderate, and no benefit), but no significant differences were found (Table 5).
Differences among three groups: large, moderate, and no benefit.

Data are presented as mean ± standard deviation or n (%).
Discussion
In this retrospective study, we assessed the value of early chest CT in the diagnosis of CAP in patients presenting to our ED. Few studies have been performed to assess the role of early chest CT (during the first 48 hours of admission) in diagnosing CAP, and to our knowledge, none of these few studies have been conducted in the Middle East.
Our study showed that early chest CT resulted in a diagnosis of CAP in more than 90% of cases, whereas CXR failed to diagnose more than half of cases. Around 41.5% of CAP cases were diagnosed by CT after negative or inconclusive CXR. Thus, chest CT can provide an early diagnosis and facilitate timely antibiotic administration in the ED setting, where crowding may sometimes delay diagnostic or therapeutic interventions.17,18 Antibiotics should be administered directly after CAP diagnosis, although the time frame or cutoff is still controversial.19,20 Maughan et al. 21 found that the subset of patients who had false-negative CXR findings and were later diagnosed with pneumonia by CT were significantly younger than patients complaining of chest pain in the ED.
In 21.5% of cases of the present study, early chest CT contributed further to the appreciation of the severity of CAP by revealing additional radiological findings (e.g., parapneumonic effusion, additional infiltrates) compared with CXR. These results are in concordance with a study by Claessens et al., 14 in which chest CT modified the classification of CAP in 58.7% of patients presenting to the ED, as well as with a study by Karhu et al., 22 in which chest CT provided additional findings in comparison with CXR in around 60% of patients with CAP requiring admission to the intensive care unit.
Low-dose chest CT has been proven to show high accuracy in diagnosing pulmonary diseases while markedly decreasing the radiation dose; some papers have suggested that it may be nearly equivalent to the radiation dose of a conventional radiograph. 8 This would favor early incorporation of chest CT in the diagnosis of CAP, especially to help predict the prognosis in patients with CAP. 23
Finally, discussing the cost of care for patients with CAP is of utmost importance in guiding strategy implementation. The cost of care of CAP depends whether the patient is admitted or treated as an outpatient. In a retrospective analysis of patients admitted for low-risk CAP within a 1-year period, the cost of inpatient care was about eight times higher than outpatient management. 24 The cost difference between chest CT and CXR depends on the country, hospital, and service requesting the imaging. The cost of chest CT ordered in ED settings may be up to six times higher than the cost of regular CXR.
Limitations
Our study has several limitations, including its retrospective nature; it was difficult to determine why chest CT was ordered, and chest CT could have been ordered after inconclusive CXR. We included all patients who underwent CXR followed by chest CT within 48 hours. The time lapse between the two modalities might have been long enough for more radiological findings to manifest. Another limitation is that our findings reflect the experience of a single tertiary care center and not the general trends throughout the country. Additionally, patient selection bias might be present because the patients were limited to the ED only. A prospective study in which both modalities are performed simultaneously is needed to allow for better evaluation. Such a study should include larger numbers of patients and determine the value of inflammatory markers such as C-reactive protein and procalcitonin in the multivariate analysis.
Conclusion
Our study showed that a reasonable number of patients who underwent chest CT and CXR within 48 hours from ED admission had findings on chest CT that were not identified on CXR and led to early recognition of pneumonia. Considering the radiation risk and cost of chest CT, ED physicians should use chest CT as an add-on imaging modality when CXR is negative or inconclusive in patients clinically suspected to have CAP, especially high-risk patients. Further large prospective studies are needed to determine the population that may benefit the most from early chest CT and the overall outcome of patients who undergo early chest CT in terms of the hospitalization duration, morbidity, and mortality.
Prior presentations
29th European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Amsterdam, the Netherlands, 13–16 April 2019. 17th annual conference of Lebanese Society of Family Medicine – “Defeating obesity: prevention and treatment,” Hilton Beirut Metropolitan Palace, Lebanon 6–7 October 2018.
Footnotes
Author contributions
DI and ZH are responsible for the study design, data collection, data analysis and interpretation, and drafting and finalization of the manuscript. AB is responsible for the oversight of the project, research idea, study design, data analysis, and writing and finalization of the manuscript. MA is responsible for the research idea and study design. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.