
Abstract
Introduction:
Evaluation of potential outcomes of COVID-19-affected pneumonia patients using computed tomography scans may not be conceivable in low-resource settings. Thus, we aimed to evaluate the performance of chest X-ray scoring in predicting the disease severity and outcomes of adults hospitalised with COVID-19.
Methods:
This was a retrospective chart analysis consuming data from COVID-19-positive adults who had chest X-ray availability and were admitted to a temporary COVID unit, in Bangladesh from 23rd April 2020 to 15th November 2021. At least one clinical intensivist and one radiologist combinedly reviewed each admission chest X-ray for the different lung findings. Chest X-ray scoring varied from 0 to 8, depending on the area of lung involvement with 0 indicating no involvement and 8 indicating ⩾75% involvement of both lungs. The receiver operating characteristic curve was used to determine the optimum chest X-ray cut-off score for predicting the fatal outcomes.
Result:
A total of 218 (82.9%) out of 263 COVID-19-affected adults were included in the study. The receiver operating characteristic curve demonstrated the optimum cut-off as ⩾3 and ⩾5 for disease severity and death, respectively. In multivariate logistic regression analysis, a chest X-ray score of ⩾3 was found to be independently associated with disease severity (aOR: 8.70; 95% CI: 3.82, 19.58, p < 0.001) and a score of ⩾5 with death (aOR: 16.53; 95% CI: 4.74, 57.60, p < 0.001) after adjusting age, sex, antibiotic usage before admission, history of fever, cough, diabetes mellitus, hypertension, total leukocytes count and C-reactive protein.
Conclusion:
Using chest X-ray scoring derived cut-off at admission might help to identify the COVID-19-affected adults who are at risk of severe disease and mortality. This may help to initiate early and aggressive management of such patients, thereby reducing their fatal outcomes.
Introduction
Since the declaration of COVID-19 as a pandemic on 11 March 2020, 1 researchers from around the globe have come forward to curb the spread of the disease. More virulent viral strains have significantly threatened the established COVID-19 diagnostic and management strategies. 2 The clinical spectrum of COVID-19 disease also ranges from asymptomatic infection to severe or critical stages of the disease where hypoxemia is an important indicator of lung involvement. However, a diagnostic dilemma is often created when hypoxemia is absent (silent hypoxemia) until the critical stages of the disease.3,4 These may cause irreversible progression of the disease. Thus, a rapid and appropriate diagnosis is the key to controlling the potential transmission and reducing secondary infections among close contacts and healthcare professionals. 5 During this pandemic, one Chinese radiology specialist gave strong recommendations on high-resolution computed tomography (CT) imaging 6 for the screening and diagnosis of COVID-19, whereas laboratory detections are time-consuming and require laborious laboratory provisions. 1 Although chest CT scans have higher sensitivity (90%) and specificity (91%) for diagnosing COVID-19 infection, they are only sometimes convenient for resource-constrained backgrounds due to the higher expense and special settings. 7 Moreover, the continuous use of chest CT scans (from diagnosis to discharge) became difficult to sustain over time due to the gradual and massive increasing number of hospitalised COVID-19 patients as well as their consequent increase in radiological examinations. 8 Besides, using radiography equipment requires high disinfection after each use, which can make massive tests painstaking and time-consuming.
In practice, for hygienic reasons, chest X-rays (CXRs) are often directly taken with patients on a stretcher or bed, lying down or, at best, sitting considered the first and most important imaging modality, 8 especially during the pandemic when the hospital systems are overwhelmed. 9 The Radiological Society of North America, the American College of Radiology and the Spanish Society of Medical Radiology recommended using a CXR to monitor and assess the COVID-19 disease progression. 9 Thus, the use of CT chests randomly is not encouraged, 8 which reduces the CT scan machine load and limits the radiation exposure and cross-infection to the patient.4,8 Till now, several severity scoring systems in CXR have been used for quantitative and objective estimation of lung involvement and progression 10 and some evaluated the area of lung involved, while others focused on infiltrative patterns.10,11 Paraskevas et al. 12 suggested two scores, BRIXIA and radiographic assessment of lung edema score (RALES), which are reliable and can be used to assess the prognosis of patients with COVID-19 requiring hospitalisation.
In our centre, we decided to use CXR either in our radiology setting unit or portable as a mainstay because it is logistically easier and faster equipment than any other radiation device. In addition, these portable technique facilities were better suited for serial monitoring of patients in poor clinical conditions. In our setting, we followed a scoring system13,14 that facilitated diagnosing deteriorating patients by evaluating CXR reports of hospitalised patients with COVID-19. To our knowledge, limited studies determined a specific cut-off derived from the CXR scoring system for predicting the outcome of COVID-19 infection.
Thus, in this study, we aimed to find an optimum cut-off from the CXR scoring system that would predict the severity of the disease and fatal outcomes of COVID-19 infection.
Ethical consideration
We received the approval of the waiver for informed patient consent from the Institutional Review Board of icddr,b for this retrospective study.
Methods and materials
Study design and data collection
This was a retrospective chart analysis consuming data from all COVID-19-positive adults who had CXR availability and were admitted to a temporary COVID-19 treatment facility at the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) from 23rd April 2020 to 15th November 2021. Dhaka Hospital recorded all the relevant COVID-19 patients’ data in their repository. We have excluded the data either due to lack of clinical information or admission CXR. The researcher used these data for scientific analysis and publication with prior approval from the authority. After receiving approval from the IRB, icddr,b on 15th February 2023, we accessed data and analysed the data between 16th February and 15th March 2023.
We treated 263 COVID-19-positive adults having different severity of pneumonia admitted into our temporary COVID unit. Among them, 218 patients were evaluable, the rest were excluded as either clinical information was incomplete or CXRs were not available. We reviewed their baseline CXRs, clinical data and laboratory reports. The admission data of these patients were collected using standard case record forms.
Patient and public involvement
We did not involve patients and members of the public in research, such as in the design, conduct, reporting or dissemination plans of the research. We collected clinical data from the health record as they were admitted for COVID-19 illness.
Clinical evaluation
Icddr,b developed a temporary COVID-19 treatment facility with 10-bed ICU dedicated to the management of COVID-19 during the pandemic and established a clinical protocol based on national and international guidelines that were revised over time to accommodate the new evidence-based recommendations. A devoted management team was formed by physicians, a radiologist, nurses and health assistants trained in critical medicine, supervised by an intensivist physician and scientist, and led by the division’s senior director. Antibiotics and other drugs were prescribed depending on clinical conditions and supportive laboratory or CXR findings. A detailed description of the unit was provided elsewhere. 15
Laboratory result and CXR analysis
Necessary laboratory investigations and digital portable CXRs (A/P view) were performed to evaluate the critically sick COVID-19-affected adults and minimise in-hospital transmission through the radiology department. We have two qualified radiographers who followed the standard recommendation of mA (milliampere). The mA is adjusted according to body weight, body thickness, age and sex. 16 At least one clinical intensivist and one radiologist combinedly reviewed each admission CXRs for the presence of consolidation, ground-glass opacities (GGO), reticular opacities and pleural effusion. The team did not have any major disagreement about the CXR findings between the radiologist and clinician. X-ray distribution was classified into ‘peripheral’ (the outer one-third of the lung), ‘central’ (the inner two-thirds of the lung) or ‘both’ and ‘unilateral’ or ‘bilateral’. The scoring was done from 0 to 4 (0 = no involvement; 1 < 25%; 2 = 25%–50%; 3 = 50%–75%; and 4 > 75% of involvement), and the scores of both lungs were summed with a maximum value of 8. 13 Figure S-1(a) and (b) expressed the examples of the CXR scoring procedure.
Operational definition
GGO: is a radiological term indicating an area of hazy increased lung opacity through which vessels and bronchial structures may still be seen. It is less opaque than consolidation, in which such structures are obscured. 17 There are many potential causes of GGO, including infections, inflammation and tumour. A 2020 review by Trusted Source also found that GGO was the most common lung abnormality among patients with COVID-19 pneumonia.
Baseline CXR: A baseline CXR is a diagnostic imaging procedure used to assess the initial condition of a patient who has been diagnosed with COVID-19 or is suspected of having the virus. It helps in identifying and visualising common pulmonary abnormalities associated with COVID-19, such as GGO, consolidations and other lung changes. These findings aid in confirming the presence of the virus and assessing the severity of lung involvement.
Disease severity: It included mild to moderate cases, where patients having an influenza-like illness with mild symptoms for instance, fever, cough, malaise, headache, sore throat, muscle pain without dyspnoea or abnormal imaging as well as an adult with fever, cough, dyspnoea, respiratory rate (RR) <30 breaths and saturation >93% without any oxygen support. And severe to critical cases, where they presented with respiratory distress and RR ⩾30 breaths/min or oxygen saturation ⩽90% at rest. For the study purpose, cases with acute myocardial infarction, COVID-19-associated coagulopathy, unremitting fever and sepsis were also included in severe cases, and also patients requiring mechanical ventilation, or high flow nasal cannula for respiratory failure or having shock or organ failure. 18
Statistical analysis
The statistical analysis for the study was performed using Stata-15 software (StataCorp LP, Texas, USA). The demographic characteristics of the study patients were summarised and compared using frequency with percentages for qualitative variables and median interquartile range (IQR) or mean standard deviation (SD) for quantitative variables. The associations between the demographic characteristics and the outcome variables were analysed using the chi-square test for qualitative variables and Mann–Whitney U test, and the t-test for quantitative variables. Odds ratios (OR) with 95% confidence intervals (CI) were calculated to represent the strength of the association between the variables. A two-sided probability of less than 0.05 was considered statistically significant. The receiver operating characteristic (ROC) curve analysis with the area under the ROC curve (AUROC) was used to explore the cut-off values in CXR scoring to predict disease severity and death. These optimal cut-off values were determined based on the highest sensitivity and specificity and were used as a predictor for disease severity and death. Simple and multivariable logistic regression analysis was performed to identify the independent variables (age, sex, antibiotic usage before admission, fever, cough, diabetes mellitus, hypertension, total leukocyte count and C-reactive protein (CRP)) that were significantly associated with the outcomes.
Results
We reviewed baseline CXR, clinical data and blood test results of 218 COVID-19-positive adults (Figure 1) and their baseline demographic and clinical characteristics are shown in Table S1.

Conceptual framework depicting the pathway from the inclusion of participants to developing the CXR scoring system for predicting disease severity and death.
Performing ROC curve analysis, we explored the cut-off for CXR score and also evaluated their sensitivity and specificity to fix an optimum cut-off that may predict disease severity and death for COVID-19-affected adults (Tables S2 and S3).
Table S4 shows the diagnostic performance of CXR in predicting disease severity and death. The AUROC is a measure of the diagnostic accuracy of a test, with a value of 1 indicating perfect accuracy and a value of 0.5 indicating no diagnostic accuracy (Figure 2(a) and (b)).

The area under the ROC curve is 0.84 (a) and the area under the ROC curve is 0.86 (b).
For predicting disease severity, the AUROC was 0.84, indicating a good level of diagnostic accuracy. Around 68.5% of patients with severe disease were correctly identified by the CXR score of ⩾3 and 89.52% of patients without severe disease were correctly identified by the CXR score of <3. For predicting death, the AUROC was 0.86, indicating a good of diagnostic accuracy level. Around 81.5% of patients who died were correctly identified by the CXR score of ⩾5. The specificity of 82.78% indicates that 82.78% of patients who survived were correctly identified by the CXR score of <5.
In Table 1, the results indicated the factors associated with severe to critical and mild to moderate outcomes in patients. Age, CXR score, hypertension, total leukocyte count and CRP were found to be significantly associated with the severe to critical outcomes; however, other factors like male sex, antibiotics usage before admission, fever, cough and diabetes mellitus were not found to be significant.
Association of outcome (disease severity) and predictors/independent variables.

n/N: number of patients; IQR: interquartile range; SD: standard deviation; OR: odds ratio; CI: confidence interval.
The mean age of COVID-19-affected adults with severe to critical illness was 58.7 ± 14.2 years, which was higher compared to the mean age of patients with mild to moderate illness (46.9 ± 15.8 years). For each 1-year increase in age, the odds of having a severe to critical illness increased by 5% (odds ratio of 1.05, 95% CI: 1.03, 1.07, p < 0.001). The proportion of patients with hypertension was higher among those with severe to critical illness (54.1%) compared to those with mild to moderate illness (35.4%), and the odds ratio of 2.14 (95% CI: 1.24, 3.72, p < 0.006) indicates that having hypertension increases the odds of having a severe to critical illness by 2.14 times. The proportion of patients with a CXR score ⩾3 was higher among those with severe to critical illness (46.7%) compared to those with mild to moderate illness (2.1%), and the odds ratio of 12.94 (95% CI: 6.53, 25.66, p < 0.001) indicates that having a CXR score ⩾3 greatly increases the odds of having a severe to critical illness (Table 1).
Table 2 represents the relationship between different variables and the fatal outcomes of COVID-19-affected adults where we observed 28 deaths (12.8%) among 218 participants. The variables included age, sex, use of antibiotics before admission, presence of fever and cough, CXR score, diabetes mellitus, hypertension, total leukocyte count and CRP.
Association of outcome (death) and predictors/independent variables.
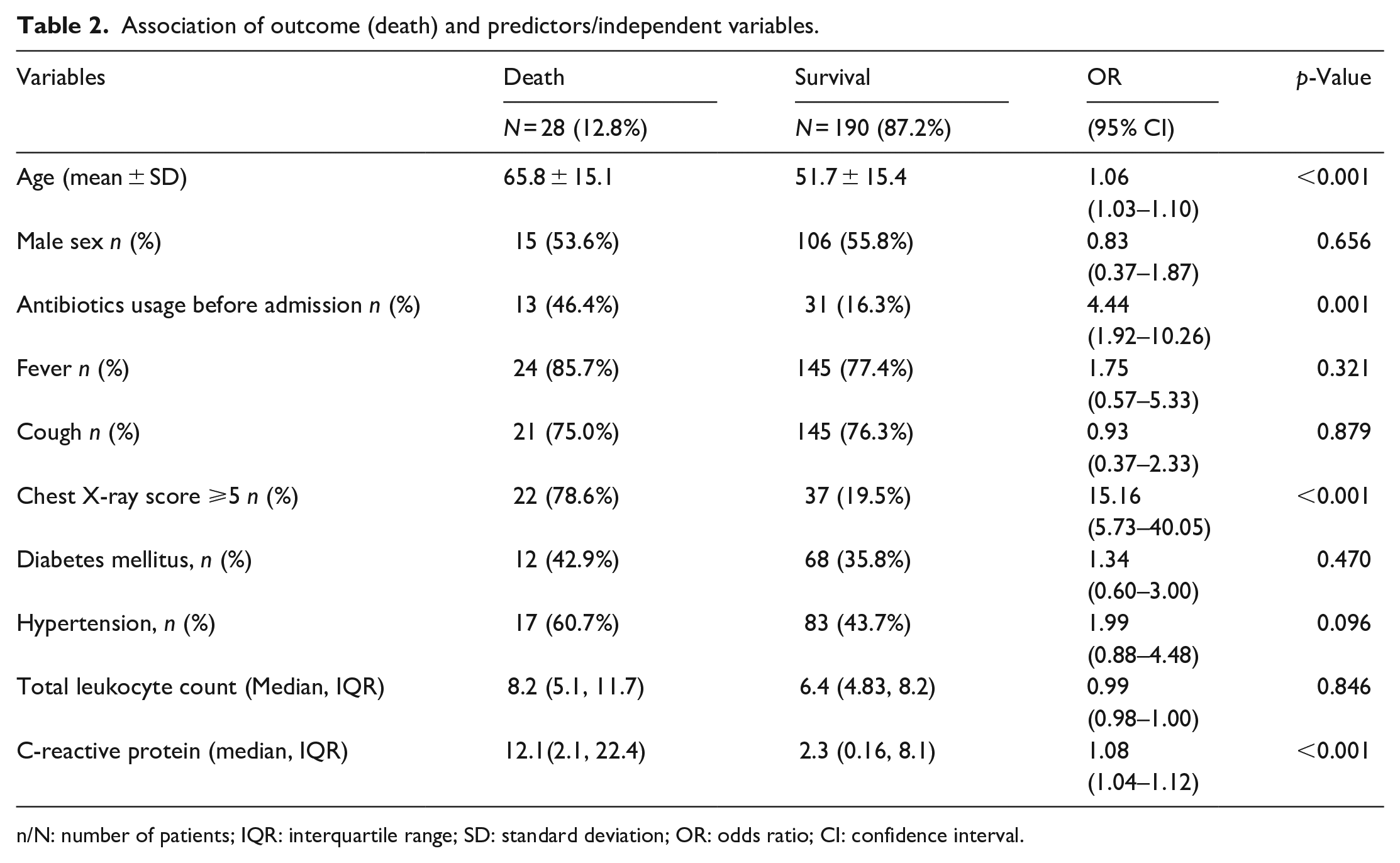
n/N: number of patients; IQR: interquartile range; SD: standard deviation; OR: odds ratio; CI: confidence interval.
These results showed that the mean age of patients who died was 65.8 years, which was significantly higher than the mean age of survivors (51.7 years). The odds ratio of 1.06 (95% CI: 1.03, 1.10) indicates that the odds of death increased by 6% with each year increase in age. The results showed that the mean age of patients who died was 65.8 years, which was significantly higher than the mean age of survivors (51.7 years). The results also showed that the use of antibiotics before admission was significantly associated with survival (OR: 4.44, 95% CI: 1.92, 10.26, p = 0.001), while CXR scores (OR: 15.16, 95% CI: 5.73, 40.05, p < 0.001) and high CRP (OR: 1.08, 95% CI: 1.04, 1.12, p < 0.001) were significantly associated with death (Table 2).
The results did not show significant associations between sex, the presence of fever or cough, diabetes mellitus or hypertension and total leukocyte count with death or survival. The results of this study suggested that age, use of antibiotics before admission, CXR scores and CRP were important factors in predicting death or survival in COVID-19-affected adults (Table 2).
Logistic regression analysis shown in Table 3 was performed to detect the independent association of outcome variables (disease severity and death) with the specific cut-off values in CXR scoring.
Logistic regression analysis is to detect the independent association of outcome variables with chest X-ray scores.
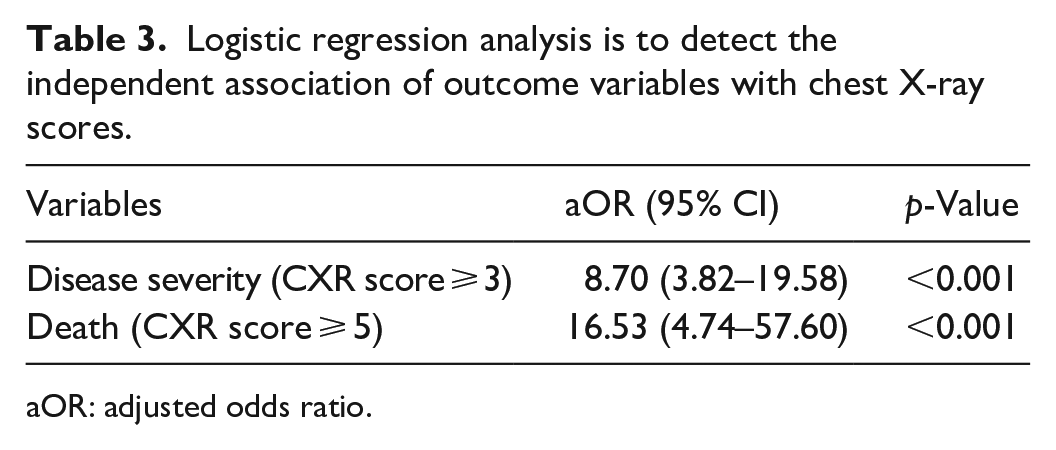
aOR: adjusted odds ratio.
Each model was adjusted for age, sex, antibiotic usage before admission, history of fever and cough, diabetes mellitus, hypertension, total leukocyte count and CRP. In CXR scoring, COVID-19 diseases, 8.70 times turned into severe to critical stages of diseases, if the cut-off value was 3 or more than their counterpart (p < 0.001) and cut-off value ⩾5 had 16.53 times more predictability of death than the survivor (p < 0.001).
Discussion
In our temporary COVID unit, we followed Orsi et al.’s eight CXR scoring system to diagnose COVID-19 pneumonia. 13 The feasibility and repeatability of a CXR severity score and the correlation between the CXR scoring and clinical and laboratory parameters were all described by the same study. 19 During the emergency crisis setting, several scoring systems of CXR in different studies were considered an essential tool, especially for patients in intensive care units. 1 It is useful for monitoring the rapid progression and the assessment of lung abnormalities among COVID-19-infected patients. CXR scoring is frequently requested to assess lung involvement due to the high positivity rate in CXR, even in silent hypoxemia. It has also been considered in both routine and emergency settings for its wide accessibility and instant execution at the patient’s bed with portable CXR machines, thus limiting cross-infection.19,20 As per recommendation from the U.S. Centres for Disease Control and Prevention, healthcare professionals must take standard precautions to control cross-infection and rapidly spreading COVID-19 diseases via respiratory droplets. 21
However, during the emergency crisis in the pandemic, the radiology department played a significant role in defining the severity or grading of COVID-19 pneumonia for the critical management of the patients through the CXR scoring system.22,23. BRIXΙA and RALES scores in CXR show good to excellent reliability as well as variability in the inter-rater agreement. The prognostic accuracy of the two scores for in-hospital mortality for all raters demonstrated good to excellent prognostic value having a consistent upward trend with significant differences between severity groups in both radiological scores. 12 At the same time, the number of chest CT requests in this pandemic has been reduced due to hassle in the subsequent necessity for intense infection control measures in CT suites as well as difficulties in mobilizing hypoxic patients, and the involvement of high radiation.24,25 Depending on the extent of involvement by consolidation or GGOs in CXR, we considered a maximum score of 8 in our setting. 19 In our study, we have categorised the CXR scoring to predict disease severity and death.
Cut-off value ⩾3 in CXR scoring predicting disease severity, and following this predicting value, patients may turn into severe to the critical stage of disease and it is advocated by 84% AUROC. Like other comorbidities, COVID-19-positive patients with hypertension are more vulnerable to disease severity and may turn into severe to critical stages of the disease. High CRP levels and total leukocyte count were also found to have an association with the severe to critical stage of the disease. Setiawati et al. have described COVID-19 pneumonia severity and assessed with the modified CXR scoring systems that correlated significantly with clinical severity and outcome.26,27 These scoring systems can help to determine the severity of the disease with its progression (severe pneumonia, acute respiratory distress syndrome, sepsis and septic shock) in COVID-19 patients, particularly in areas where facilities and specialists are scarce. In this study, three scoring systems like Brixia score (p < 0.01, correlation coefficient 0.232), RALE score (p < 0.01), correlation coefficient 0.209), and Dr. Soetomo General Hospital score (p < 0.01, correlation coefficient 0.194) were observed and found to have significantly correlated with the clinical severity of the disease. Due to a lack of clinical data, the comparison between the scoring systems and patient’s comorbidities was not evaluated in this study. 27 Several studies revealed that CXR severity based on scoring correlated with inflammatory markers including high CRP levels have been observed in patients with severe COVID-19 infection and required supplemental oxygen during admission.22,28 Like our study, Toussie et al. 29 formulated a simple CXR scoring system among patients aged 21–50 years who were admitted and had an initial CXR. In this study, CXR divided the lungs into six zones and found hospital admission was associated with a higher score (>2 out of 6) and a score of >3 at admission was associated with a higher risk of severity of the diseases and required ventilatory support.
Other findings in our study, cut-off value ⩾5 in CXR scoring, were found to have a high chance to predict mortality and supported by AUROC findings. A study was conducted in Italy among 302 hospitalised Caucasian patients with COVID-19 for whom the outcomes were available where X-ray scoring named BRIXIA scoring which had been found to predict in-hospital mortality for COVID-19 having high score values.29,30 Another study conducted among 343 following hospitalisation with COVID-19 found that a CXR score of cut-off ⩾3 independently predicted mortality. 31 Our analysis also revealed that in COVID-19 patients, 13 (46.43%) who had used antibiotics before admission are 4.4 times more vulnerable to death compared to those who did not receive antibiotics before admission. On the contrary, Cao et al. 32 exploded in their study that the administration of antimicrobial treatments was not related to mortality. 32 Rawson et al. 33 reported in their study that bacterial and fungal coinfection rates were lower in patients presenting with coronavirus infections. In their article, among nine studies, bacterial coinfection was 8% in COVID-19 cases, and broad-spectrum antimicrobial therapy was used for 72% of COVID-19 cases. However, the generation of prospective evidence is required to support the antimicrobial policy as well as specific interventions for the COVID-19 pandemic. 33 Furthermore, in our study, patients with comorbidities like diabetes mellitus and hypertension had higher percentages of risk of mortality compared with those who survived. Concerning laboratory findings, high CRP level was significantly associated with the risk of mortality.
Strengths and limitations of this study
Our study’s objective was to emphasize the performance of CXR scoring for the prediction of disease severity and mortality. The validated cut-off values in the CXR scoring system in our study could play in primary- or secondary-level hospitals where patients rush and overwhelm a healthcare system, especially in lower-and middle-income countries. Thus, it can be used to assess which patients could need special attention for hospital admission as well as tertiary care in countries, where there is an outburst of cases and scarcity in the healthcare system.
Being a retrospective and single-centered study was one of the limitations. We collected all data from 23rd April 2020 to 15th November 2021, so we did not calculate the sample size and power of the study. The lack of a gold standard especially the absence of CT scan findings in validating the CXR scoring for the prediction of disease severity and mortality was a major limitation of this study. However, to our knowledge, this was the first study from Bangladesh and the information generated from this study will be valuable for other clinicians and policymakers in limited resources settings such as Bangladesh.
Conclusions
Our data suggest that cut-off values in the CXR scoring system are promising for predicting disease severity and deaths. Thus, validated cut-off values and these simple predicting factors may help to initiate early intervention with aggressive treatment among COVID-19-affected adults with different severity of pneumonia to reduce their fatal outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231222325 – Supplemental material for Performance of chest X-ray scoring in predicting disease severity and outcomes of patients hospitalised with COVID-19 in Bangladesh
Supplemental material, sj-docx-1-smo-10.1177_20503121231222325 for Performance of chest X-ray scoring in predicting disease severity and outcomes of patients hospitalised with COVID-19 in Bangladesh by Shamsun Nahar Shaima, Md Ahshanul Haque, Monira Sarmin, Sharika Nuzhat, Yasmin Jahan, Fariha Bushra Matin, Lubaba Shahrin, Farzana Afroze, Haimanti Saha, Rehnuma Tabassum Timu, Mehnaz Kamal, Abu Sadat Mohammad Sayeem Bin Shahid, Nadia Sultana, Gazi Md. Salahuddin Mamun, Mohammod Jobayer Chisti and Tahmeed Ahmed in SAGE Open Medicine
Footnotes
Acknowledgements
We gratefully acknowledge core donors of the International Centre for Diarrhoeal Disease Research, Bangladesh for their support and commitment to research efforts. icddr,b, receives unrestricted support from the Government of the People’s Republic of Bangladesh, Canada, Sweden and the UK. We would like to express our sincere thanks to all clinical fellows, nurses, members of the feeding team and cleaners of the hospital for their invaluable support and contribution to patient care.
Author contribution
TA, MJC, MS and SNS conceived and designed the study. TA, MJC, MS, SN, YJ, LS and FA supervised the project administration, MAH, MJC and SNS did data analysis. SNS, MS, SN, YJ and MJC drafted the manuscript. LS, FA, SN, YJ, MS, ASMSBS and MJC critically revised and edited the paper. SNS, MAH, ASMSBS, GSM and MJC had full access to all study data. MK, NS, RTT, FBM and HS collected and verified the data. All authors agree to be responsible for the accuracy and integrity of the data and accept accountability for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our Institutional Review Board is comprised of Research Review Committee and Ethical Review Committee. Ethical approval for this study was waived as it was a retrospective study and also not taking the consent. Through vigorous review process, IRB approved this manuscript developed from retrospective data set. An approval letter from Ethical Review Committee of icddr,b is attached here.
Informed consent
Informed consent was not sought for this study, as data were collected retrospectively and an approval letter from Ethical Review Committee of icddr,b has been taken for this context.
Trial registration
Not applicable.
Data sharing statement
The data set contained the personal information of the study participants. Our institutional review board will not have the provision to disclose any kind of information. Thus, our policy is not to make the data set available in the manuscript, the supplemental files or a public repository. However, data related to this manuscript are available upon request. Researchers who meet the criteria for access to confidential data may contact Ms. Armana Ahmed (aahmed@icddrb.org) to the research administration of icddr,b (![]() ).
).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.