
Abstract
Neurological complications after spinal anesthesia have been rarely reported. Persistent neurological dysfunction due to spinal cord or nerve root injury is a serious complication of lumbar anesthesia and manifests as leg pain, numbness, and weakness after initial recovery from anesthesia. We herein report a case of foot drop on the opposite side after spinal anesthesia for ankle fracture surgery. The patient’s symptoms completely disappeared after 3 months, and we consider that her neurological complications were likely caused by the neurotoxicity of local anesthetics.
Introduction
Neurological complications after spinal anesthesia have been rarely reported. 1 Persistent neurological dysfunction due to spinal cord or nerve root injury is a serious complication of lumbar anesthesia and manifests as leg pain, numbness, and weakness after initial recovery from anesthesia.2,3 Fortunately, such neurological complications are often temporary and reversible. Nevertheless, these infrequent complications often lead to pain and incomprehension. Therefore, it is necessary for doctors to increase their experience with managing such neurological complications and share solutions with one another. To the authors’ knowledge, few cases of such complications after caesarean section have been reported in the English-language literature. We herein report a case of foot drop on the opposite side after spinal anesthesia for ankle fracture surgery.
Case report
A 30-year-old woman underwent surgery for a fracture of her right ankle. Spinal anesthesia was administered using a 25-gauge spinal Quincke needle with the patient in the left lateral position. The needle was inserted into the L3–L4 space. After withdrawal of cerebrospinal fluid, 2 mL of 0.75% piperocaine was injected with no resistance. Following needle removal, the patient’s position was immediately changed to the supine position. The effect of anesthesia was rapid, and the patient’s vital signs were stable. About 10 minutes later, the nerve block was at the T10 level, which fully meet the surgical needs. The patient was changed to the left lateral position again for performance of the right ankle surgery. The operative duration was 2 hours, and the patient reported no discomfort during the operation. Two hours postoperatively, the patient recovered voluntary movement of both lower limbs, her muscle strength was grade 3, and she reported skin numbness. At 4 hours postoperatively, her thigh muscle strength was completely recovered. The patient reported that the incision on the affected side was slightly painful and that the skin felt normal; on the healthy side (left lower limb), however, she felt numbness and weakness from the calf to the foot. The day after the operation, the numbness of her leg and foot on the healthy side was not significantly relieved, the feeling of weakness was more severe, and foot drop was obvious. We considered the possibility of temporary neurological symptoms after lumbar anesthesia and thus administered glucocorticoids and dehydrating drugs to the patient. On the second day after the operation, the numbness of the left lower limb was alleviated and its severity was decreased; however, the patient still had a feeling of weakness. The above-mentioned drug treatment was continued and the patient’s condition was closely observed. On the third day after the operation, foot drop and numbness were still present in the dorsum and plantar aspects of the foot, and the symptoms were no longer substantially relieved thereafter.
Lumbar magnetic resonance imaging revealed subcutaneous fasciitis of the lower back (Figure 1). Doppler ultrasound of the nerves showed no obvious peroneal nerve compression (Figure 2). The patient received Chinese acupuncture after discharge. During the next 2 months, she experienced spontaneous motor recovery to grade 4/5 in her left ankle. Three months after surgery, the patient’s left foot symptoms were completely recovered and she was able to walk on the ground with a cane as the fracture of the right ankle progressed toward bone union.

Magnetic resonance imaging showed subcutaneous fasciitis of the lower back.
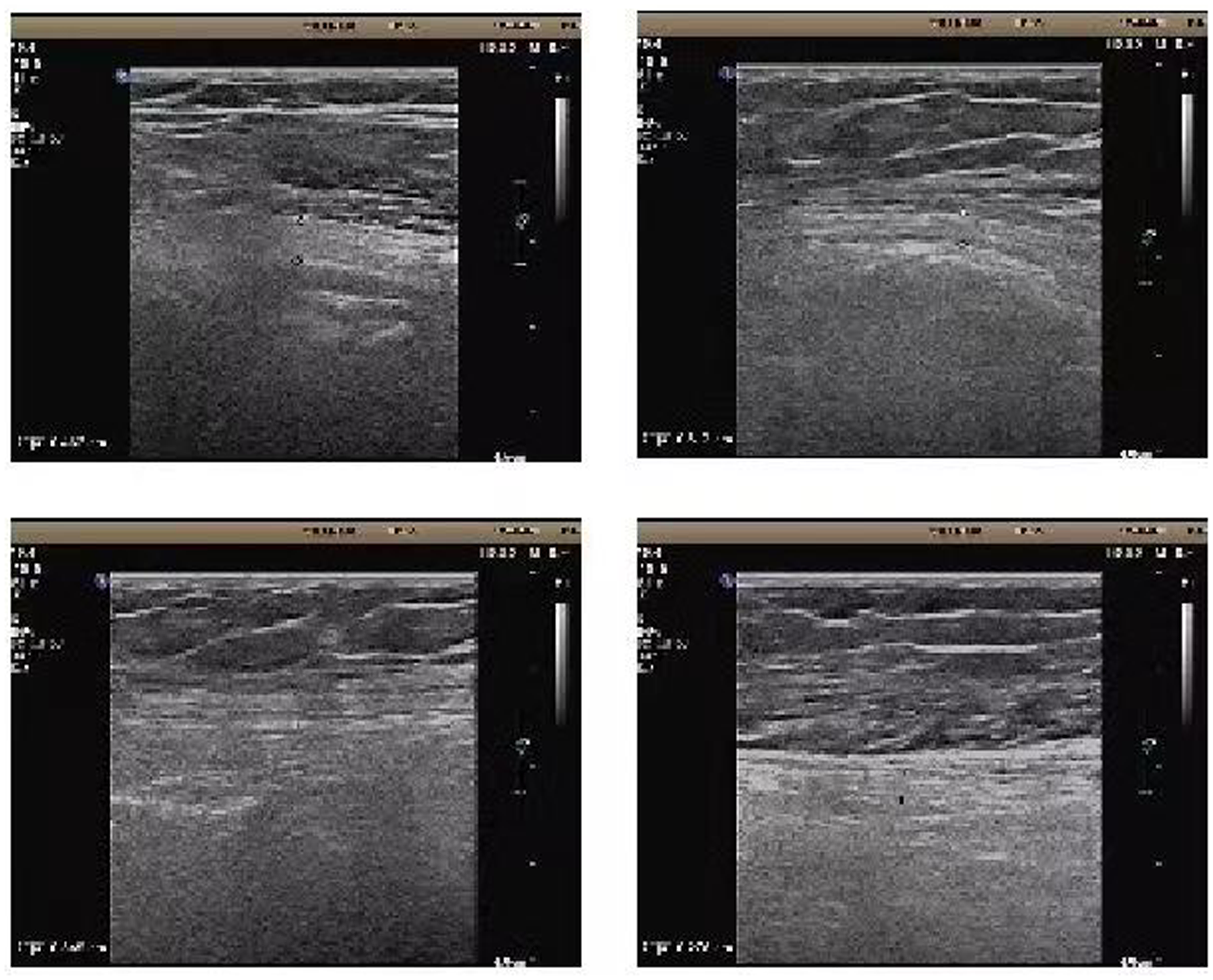
Doppler ultrasound of the nerves showed no peroneal nerve compression.
Discussion
Lumbar anesthesia has been widely used in various operations, such as cesarean section and lower limb surgery, because of its advantages of accurate anesthesia, rapid onset, and less drug use. Persistent neurological dysfunction due to spinal cord or nerve root injury is a serious complication of lumbar anesthesia, but it is not common. In one study, the incidence of complications after epidural anesthesia was 0.35/10,000, and that after spinal anesthesia was 0.42/10,000. 1 A few case reports to date have described foot drop after spinal anesthesia for cesarean section.2,3 We have herein reported a case of foot drop on the opposite side after spinal anesthesia for ankle fracture surgery.
The most common causes of neurological complications after lumbar anesthesia include direct needle trauma and neurotoxicity from local anesthetics.4,5 Direct needle trauma is mainly caused by puncture location errors and repeated attempts. In the present case, the anesthesiologist did not make repeated attempts, and there was no resistance to injection; therefore, the nerve injury was less likely to have been caused by incorrect puncture. Local anesthetics have been found to have toxic effects on the spinal cord or nerve roots, and these effects are often strongly correlated with concentration and dose. Three possible mechanisms are as follows. First, local anesthetics directly act on central or peripheral neurons, disrupt the oxidative phosphorylation process of neurons, affect the transmembrane action potential of mitochondria, and cause programmed neuronal apoptosis. Second, local anesthetics inhibit endothelial-dependent vasodilation or interfere with prostaglandin synthesis, resulting in decreased neuronal blood flow and hypoxia injury. Third, intracellular ion overload destroys the cell structure and directly causes nerve injury.
In addition, a spinal epidural or subdural hematoma, an epidural abscess, bacterial or aseptic meningitis, and anterior spinal artery syndrome can all cause neurological complications. In the present case, magnetic resonance imaging showed only lumbar fasciitis and skin folds after puncture; no changes in spinal cord signaling were observed. We considered that common peroneal nerve injury due to postural compression was also possible because the patient was in the lateral decubitus position during the surgery. 6 However, considering the scope of the patient’s sensory impairment and results of her Doppler ultrasound examination, we excluded this factor.
Glucocorticoids and dehydrating drugs were considered effective and safe in the early stage. The patient showed a significant decrease in the level of sensory impairment during the first 3 days, but complete recovery appears to be a lengthy process. Fortunately, the current literature indicates that such neurological complications are often temporary and reversible. Traditional Chinese medicine and acupuncture may have unique effects in treating nerve injury. Therefore, a positive attitude is desirable because it may be more conducive to the patient’s recovery.
Footnotes
Declaration of conflicting interests
The authors declare no conflict of interest in preparing this article.
Consent statement
Verbal consent was obtained from the patient by telephone.
Ethics
The requirement for ethics approval was waived because the author’s institution does not require ethics approval for retrospective reports of individual cases that do not involve human studies.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.