
Abstract
Dextrocardia is a rare cardiac malposition that was first described in 1606. Mirror-image dextrocardia is characterized by a mirror-image change of the normal position of the heart. Most cases are accompanied by situs inversus viscerum, whereas only 3% to 10% of cases are associated with intracardiac anomalies. Valve surgery for acquired valvular lesions in patients with mirror-image dextrocardia with situs inversus is rare. Diagnosing situs anomalies in adults is important to prevent errors during surgical operations, emergency procedures, or interventional operations. In this report, we present two cases of mitral regurgitation in patients with mirror-image dextrocardia. One patient had mirror-image dextrocardia with subacute infective endocarditis and mitral regurgitation, and the other patient had mirror-image dextrocardia with mitral Carpentier type I regurgitation. In both patients, mitral valve repair was successfully performed using a transseptal approach.
Teaching points
Dysplasia of the inferior vena cava is important because patients with dextrocardia may have an interruption of the inferior vena cava in the liver, and such patients require venous cannulation through the inferior vena cava during cardiac surgery. Computed tomography is an effective means of examining the superior and inferior vena cava for abnormalities in all patients with dextrocardia. In such cases, the keys to the whole operation are the position of the surgeon, the surgical incision, and the site of venous and arterial catheterization. These decisions should be based on the results of preoperative imaging studies. In a typical case of dextrocardia with situs inversus, standing on the patient’s left side provides a good view of the mitral valve surgical field and is reportedly the preferred method for mitral valve surgery in this patient population. The mitral valve has a symmetrical appearance; therefore, it is not difficult to operate on the mitral valve in patients with dextrocardia. Because the tricuspid valve has an asymmetrical three-dimensional configuration, however, special attention should be paid to tricuspid annuloplasty in such patients. A rigid three-dimensional annuloplasty ring turned over will not fit the cardiac anatomy of patients with dextrocardia; therefore, a flexible ring is recommended for tricuspid annuloplasty.
Introduction
Dextrocardia is an anatomical peculiarity in which the heart is located in the middle of the mediastinum with its basal-to-apical axis pointing to the right and caudally. Situs inversus totalis associated with dextrocardia is rare, affecting 1 in 10,000 adults. 1 The occurrence of dextrocardia is closely related to the left–right axis specification of the embryo. Asymmetric expression of Nodal, Pitx2, Cited2, and other related signaling molecules as well as the regulation of signaling pathways are important factors affecting the specification of the left and right axes.2–5 Deletion or abnormal expression of signaling molecules related to the left and right body axes can lead to the formation of dextrocardia. 6 Many animal experiments have been carried out to explore the underlying molecular mechanisms of this condition,7,8 and great progress has been made. However, the specific mechanisms remain unclear. Furthermore, dextrocardia is not directly related to race, ethnicity, or sex.
Cardiac surgery in patients with dextrocardia poses difficult problems because of the unusual anatomy of the heart. Various surgical techniques have been used to deal with the unusual anatomical disposition of the heart and obtain good valve exposure. However, few reports have focused on mitral valve surgery in patients with dextrocardia. Fishman et al. 9 described a family with major cardiac anomalies (including dextrocardia) and ocular anomalies in three members. However, the dextrocardia in this family was of the situs inversus type. Three siblings had dextrocardia, and all of them had situs solitus. Kikon et al. 10 also reported a case of dextrocardia with situs solitus in which the surgeon approached the operation from the left side of the patient. The left-sided approach makes it easier to visualize the valve as it will appear from the right side and has been found to be comfortably implemented by other research groups. Khan et al. 11 reported a case of dextrocardia with situs solitus in a patient with moderate pulmonary hypertension. The aorta was difficult to visualize; consequently, cannulation was not easy to perform. However, two-stage venous cannulation was used for venous drainage, and inferior vena cava cannulation was not performed. Inferior vena cava cannulation could have been extremely risky because the left ventricle would have been lifted, potentially causing it to rupture against the valve prosthesis. The incision was made in the left atrium with the surgeon on the left side of the patient. This approach was noted to provide good exposure with less retraction. A starfish retractor has also reportedly been used to lift the heart to the left side and establish cardiopulmonary bypass. 11 We herein report the surgical management of two cases of dextrocardia with mitral regurgitation. The reporting of this study conforms to the CARE guidelines. 12
Case Reports
Case 1
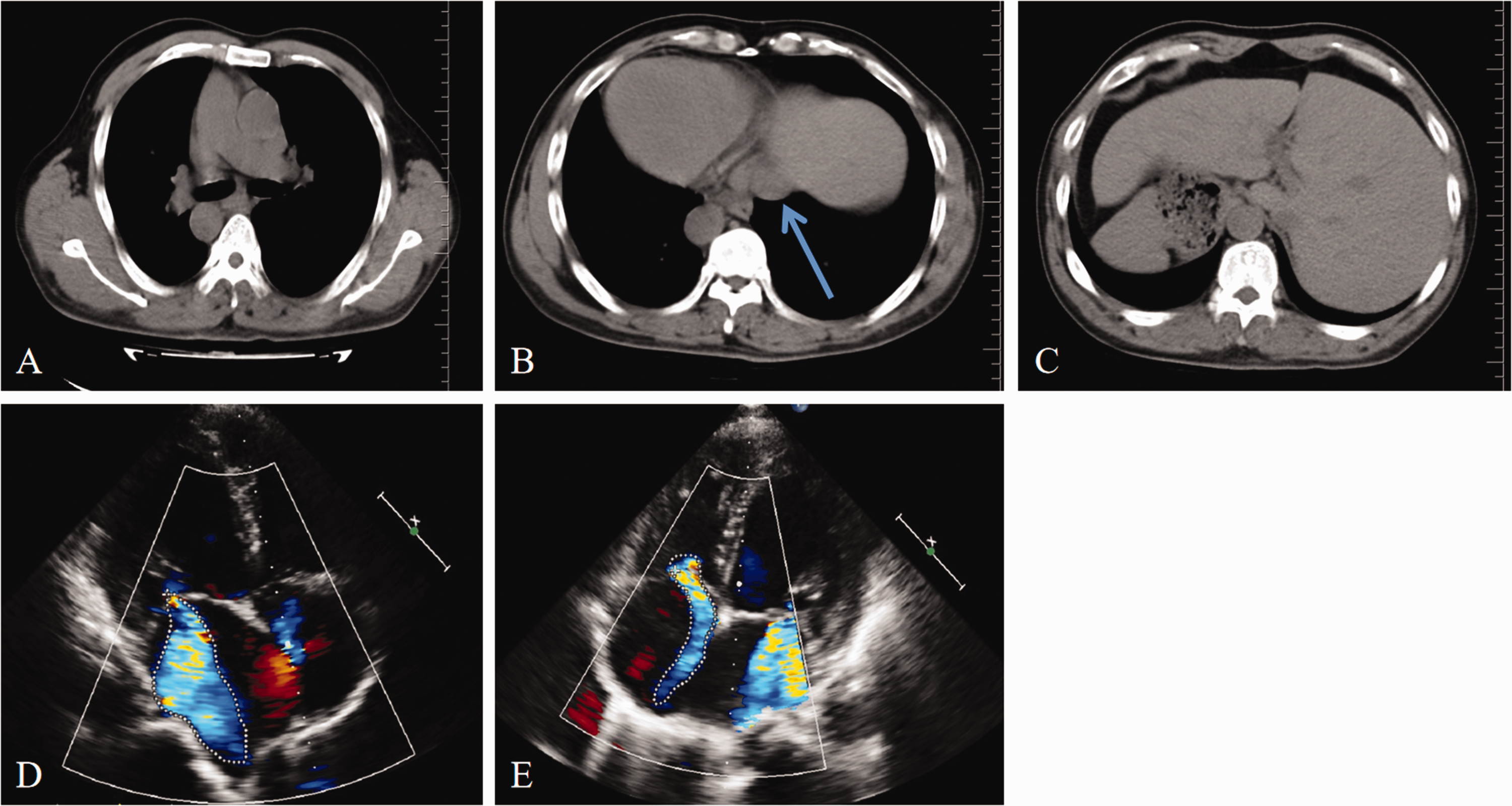
A 50-year-old man with intermittent dyspnea, low-grade fever, and dizziness was transferred to our department from a county hospital. He denied any family history of dextrocardia with situs inversus. He had a history of diabetes and cerebral infarction that had been diagnosed at other county hospitals. Preoperative computed tomography (CT) revealed dextrocardia with an enlarged silhouette, situs inversus totalis, and normal continuity of the inferior vena cava (Supplementary Video 1). The anatomical diagnosis was mirror-image dextrocardia, looped ventricles, and normal related great arteries without associated congenital cardiac abnormalities (Figure 1(a)–(c)). Transthoracic echocardiography further revealed severe mitral valve regurgitation with a significantly thickened tip of the posterior leaflet of the mitral valve. When closed, the posterior leaflet was detached from the left atrium. Echocardiography also showed extensive systolic eccentric regurgitation of the left atrium with an area of about 16.3 cm2 (Figure 1(d), (e)). The left ventricular end-diastolic diameter was 65 mm, left atrial anteroposterior diameter was 60 mm, and ejection fraction was 55% as measured by echocardiography. Preoperative blood culture suggested the presence of grass-green streptococci, so named because the α-hemolytic zone appears as a grass-green zone around the colonies.

Preoperative imaging and ultrasound findings of the first patient. (a) X-ray examination indicated dextrocardia and cardiac enlargement. (b) Confirmation of an L-loop ventricular orientation and concordant atrioventricular connections. (c) Computed tomography revealed transposition of the abdominal organs and normal continuity of the inferior vena cava (blue arrow). Transthoracic echocardiography showed (d) severe mitral regurgitation and (e) mitral valve vegetation.
Case 2
A 57-year-old man with progressive exertional dyspnea was transferred to our department from a county hospital. He denied any family history of dextrocardia with situs inversus or other cardiac health comorbidities. Preoperative CT revealed dextrocardia with situs inversus totalis (the liver was on the left side of the abdomen, the spleen was on the right side of the abdomen, and the inferior vena cava was on the left side of the aorta) and normal continuity of the inferior vena cava (Figure 2(a)–(c), Supplementary Video 2). Transthoracic echocardiography further revealed severe mitral valve regurgitation with a widely distributed mitral regurgitation signal in the left atrial systolic phase (the regurgitation area was approximately 13.4 cm2) and a widely distributed tricuspid regurgitation signal in right atrial systolic phase (the regurgitation area was approximately 6 cm2) (Figure 2(d), (e)). The left ventricular end-diastolic diameter was 62 mm, left atrial anteroposterior diameter was 46 mm, and ejection fraction was 29% (two-plane Simpson method) as measured by echocardiography. The coronary arteries were found to be normal by coronary angiography performed before surgery.
Preoperative imaging and ultrasound findings of the second patient. (a) Confirmation of an L-loop ventricular orientation and concordant atrioventricular connections. (b) Computed tomography revealed normal continuity of the inferior vena cava (blue arrow). (c) Computed tomography revealed transposition of the abdominal organs. Transthoracic echocardiography showed (d) severe mitral regurgitation (dotted line) and (e) moderate tricuspid valve regurgitation (dotted line).
Surgical technique
Both patients underwent cardiac surgery as planned with sternotomy and cardiopulmonary bypass. After complete inspection of the mediastinum and its contents, the surgeon remained on the right side of the patient, and cannulation was performed by inserting the arterial cannula into the ascending aorta and the venous cannula into the superior vena cava and inferior vena cava. Moderate hypothermia was applied. Cardioplegic arrest was achieved using antegrade crystalloid cardioplegia and blood cardioplegia. Carbon dioxide was insufflated into the surgical field. After the beginning of cardiopulmonary bypass, the surgeon switched his position from the right side to the left side of the patient. Because of the deep position of the left atrium (due to the malposition), we decided to perform a right atriotomy via a transseptal approach instead of a left atriotomy because of the possibility that a left atriotomy would not provide sufficient exposure to reach the mitral valve.
In the first patient, we first explored the left atrium without thrombosis and then explored the mitral valve. Vegetations were present in the P3 area of the valve leaflet and measured approximately 12 mm. We cut off these vegetations (Supplementary Video 3) and performed repeated water injection tests. This confirmed that the prolapse of the edge of the valve in the P3 area was causing severe mitral insufficiency. We decided to suture and fold the area with polypropylene 5-0 sutures. After the second water injection test, the mitral regurgitation was significantly improved; however, a small amount of central regurgitation was still present. Finally, we implanted a 30-mm Carpentier-Edwards Physio II forming ring (Edwards Lifesciences, Irvine, CA, USA), and the intraoperative water injection test result was satisfactory. We completed the process of tricuspid valve formation using a flexible annuloplasty ring. We followed up the patient early after surgery and 2 months after discharge, and his postoperative chest X-ray findings were normal (Figure 3(a)). The patient was classified as having New York Heart Association class I heart failure with satisfactory mitral valve function on echocardiography (Figure 3(b)).

Postoperative imaging and ultrasound findings of the first patient. (a) Chest X-ray re-examination 2 months postoperatively and (b) Transthoracic echocardiography showed minimal mitral regurgitation 2 months postoperatively.
In the second patient, after exploring the left atrium and finding no thrombus, we evaluated the enlarged mitral annulus. Repeated water injection tests showed Carpentier type I regurgitation, with particularly obvious regurgitation at the posterior–interior junction of the anterior and posterior lobes. In our center, the probability of mitral valve repair in such cases is high; therefore, we used a 5-0 Proline suture line to close the posterior–interior junction of the anterior and posterior lobes of the mitral valve. After measuring the annulus with a specific instrument, a 30-mm mitral annuloplasty ring was implanted, and repeated water injection tests yielded satisfactory results. We completed tricuspid valvuloplasty and implanted a tricuspid annuloplasty ring. The patient’s postoperative chest X-ray findings were normal (Figure 4(a)). Postoperative transthoracic echocardiography revealed mild mitral valve regurgitation and normal left and right ventricular function (Figure 4(b)).

Postoperative imaging and ultrasound findings of the second patient. (a) Postoperative chest X-ray re-examination and (b) Early postoperative transthoracic echocardiography showed mild mitral regurgitation.
Discussion
Cardiovascular imaging techniques are widely used and indispensable for the diagnosis and treatment of valvular heart disease. 13 Thus, dextrocardia is not difficult to diagnose clinically, and it is easy to identify such patients with CT and X-ray examinations. CT plays an important role in preoperative planning 13 because dextrocardia may be associated with an additional risk of cardiovascular abnormalities. Up to 25% of patients with dextrocardia have cardiac abnormalities such as azygos continuation of the inferior vena cava and partial anomalous pulmonary venous return. 14 Dysplasia of the inferior vena cava is important because these patients may have an interruption of the inferior vena cava in the liver, necessitating venous cannulation through the inferior vena cava during cardiac surgery. 1 CT is an effective means of examining the superior and inferior vena cava for abnormalities in all patients with dextrocardia. 13 The left atrial approach and a single dual-stage venous cannula may be used when the right ventricle blocks access to the inferior vena cava. 10 In most cases, central cannulation is used. However, in cases of posterior rotation and deep left atrial location, peripheral cannulation of the femoral vein is preferred because of the poor location and inaccessibility of the inferior vena cava.
Few literature reviews have focused on reports of mitral valve surgery in patients with dextrocardia. 10 Often, the most important aspect of surgery is exposure of the surgical field because the intervention itself does not differ from that in patients with levocardia. The keys to the whole operation are the position of the surgeon, the surgical incision, and the sites of venous and arterial catheterization. These decisions should be based on the results of preoperative imaging studies. In a typical case of dextrocardia with situs inversus, standing on the patient’s left side provides a good view of the mitral valve surgical field and is reportedly the preferred method for mitral valve surgery in this patient population. 10 For patients who have previously undergone cardiac surgery, repeat median sternotomy is associated with well-known risks, and right-sided thoracotomy has been widely used for repeat mitral valve surgery with outcomes similar to those of sternotomy. 15
The mitral valve has a symmetrical appearance; therefore, it is not difficult to operate on the mitral valve in patients with dextrocardia. Kishimoto et al. 16 reported that implantation of a semirigid three-dimensional saddle-shaped ring in patients with dextrocardia in the same manner as that in patients with a normally positioned heart can achieve satisfactory results. The left circumflex coronary artery usually runs near the mitral valve annulus at the lateral scallop of the posterior leaflet. Therefore, coronary artery injury must be avoided when inserting annuloplasty stitches around this region. Because the tricuspid valve has an asymmetrical three-dimensional configuration, special attention is needed when performing tricuspid annuloplasty in such patients. A rigid three-dimensional ring turned over will not fit; therefore, a flexible ring is recommended for tricuspid annuloplasty in these patients. 16 Park et al. 17 reported that continuous over-and-over suturing can achieve even plication of the tricuspid annulus, which prevents shrinkage of the flexible ring that might otherwise occur during ligation of the mattress suture. In addition, to avoid atrioventricular block in the mirror-image structure, sutures should not be placed around the conduction pathway on the septal leaflet. With a thorough understanding of the anatomical features of the mirror-image heart, mitral and tricuspid repair in patients with dextrocardia is not particularly difficult. Although our patients only underwent surgical repair of the mitral valve, there are sporadic reports of successful transcatheter aortic valve repair and transcatheter mitral valve repair procedures using a Carillon device (Cardiac Dimensions, Kirkland, WA, USA) in patients with valvular disease.18,19 More options for the treatment of such patients in future are anticipated.
In our patients, preoperative CT showed no abnormalities of the inferior and superior cava positions at the level of the right atrium, and the dimensions of the right ventricle were almost normal. This facilitated easy dissection and placement of snares on the inferior vena cava and optimal cannulation of the inferior vena cava. Although a previous report described access to the mitral valve through the left atrium (75%), 20 we consider the double-caval cannulation strategy for transseptal mitral valve repair to be a reliable and reproducible technique that can also be used in patients with associated tricuspid valve disease. The key to successful mitral valve repair relies on familiarity with the mitral valve anatomy and lesion classification rather than being significantly impacted by differences in dextrocardia.21–23 Thorough preoperative examination and knowledge of the anatomy of patients with dextrocardia associated with positional inversion is essential to prevent potential complications. The present study emphasizes the significance of CT examination before rare surgical operations. Such imaging allows detailed preoperative planning, aids proper cardiac intervention, and reduces the risk of complications. 24 It is extremely useful in the evaluation of anatomically unique cases such as the two patients with dextrocardia described herein.
Conclusion
Valve surgery for acquired valvular lesions in patients who have mirror-image dextrocardia with situs inversus is rare. Familiarity with the mitral valve anatomy and lesion classification are the keys to successful mitral valve repair. Thorough preoperative examination and an understanding of the anatomy of patients with dextrocardia associated with situs inversus is necessary to prevent potential complications.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231189129 - Supplemental material for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature
Supplemental material, sj-pdf-1-imr-10.1177_03000605231189129 for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature by Jun Nie, Tiansheng Tang, Ziao Wang, Dafa Zhang, Jun Wei and Weiyong Sheng in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605231189129 - Supplemental material for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature
Supplemental material, sj-pdf-2-imr-10.1177_03000605231189129 for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature by Jun Nie, Tiansheng Tang, Ziao Wang, Dafa Zhang, Jun Wei and Weiyong Sheng in Journal of International Medical Research
Supplemental Material
sj-mp4-3-imr-10.1177_03000605231189129 - Supplemental material for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature
Supplemental material, sj-mp4-3-imr-10.1177_03000605231189129 for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature by Jun Nie, Tiansheng Tang, Ziao Wang, Dafa Zhang, Jun Wei and Weiyong Sheng in Journal of International Medical Research
Supplemental Material
sj-mp4-4-imr-10.1177_03000605231189129 - Supplemental material for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature
Supplemental material, sj-mp4-4-imr-10.1177_03000605231189129 for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature by Jun Nie, Tiansheng Tang, Ziao Wang, Dafa Zhang, Jun Wei and Weiyong Sheng in Journal of International Medical Research
Supplemental Material
sj-mp4-5-imr-10.1177_03000605231189129 - Supplemental material for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature
Supplemental material, sj-mp4-5-imr-10.1177_03000605231189129 for Mitral valve repair in patients with mirror-image dextrocardia and situs inversus: two cases and a review of the literature by Jun Nie, Tiansheng Tang, Ziao Wang, Dafa Zhang, Jun Wei and Weiyong Sheng in Journal of International Medical Research
Footnotes
Acknowledgement
The authors thank the patient for providing consent for publication of this report.
Author contributions
W.S. drafted the original manuscript. T.T. designed the study. Z.W. was responsible for the data collection. All authors read and approved the final manuscript. J.N., T.T., and Z.W. contributed equally to the article. D.Z. and J.W. checked the English descriptions and grammar. J.N. made major revisions to the paper.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no competing interests.
Ethics statement
All studies involving human participants were reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College [Wannan Medical College Yijishan Hospital 2023-(Ethical Review Committee) No. 63]. The patients provided their written informed consent to participate in this study. Written informed consent was also obtained from the patients for publication of this case report and any accompanying images.
Funding
This work was supported by the 2021 Anhui University Humanities and Social Sciences Major Project “Current Situation, Influencing Factors and Intervention Research of Pulmonary Nodule Patients with Anxiety and Depression Symptoms in Southern Anhui Province” (Fund No. SK2021ZD0071).
Supplementary material
Supplementary Video 1
Supplementary Video 2
Supplementary Video 3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.