
Abstract
Objective
This study was performed to analyze the risk factors associated with flexor pollicis longus (FPL) attrition or rupture after volar plating of distal radius fractures.
Methods
Three hundred thirty-eight patients with distal radius fractures were included in this retrospective study. Univariate analysis and multivariate logistic regression analysis were performed to predict risk factors.
Results
Univariate analysis showed that sex, volar tilt, the Soong grade, the plate-to-critical line distance (PCLD), the plate-to-volar rim distance (PVRD), and the time of plate removal were significantly associated with FPL attrition or rupture. Multivariate logistic regression analysis demonstrated that decreased volar tilt, Soong grade 2, PCLD of >2 mm, PVRD of <3 mm, and plate removal at ≥1 year were the risk factors significantly associated with FPL attrition or rupture.
Conclusions
Reduced volar tilt, Soong grade 2, PCLD of >2 mm, and PVRD of <3 mm appear to be risk factors that are significantly associated with FPL attrition or rupture. The findings of this study also suggest that the risk of tendon rupture is lower if a Soong grade 2 plate is removed, the PCLD is >2 mm, the PVRD is <3 mm, or reduced volar tilt is achieved earlier (at <1 year).
Keywords
Introduction
Internal fixation with volar locking plates has become an increasingly popular technique for management of displaced unstable distal radius fractures.1–4 However, this technique is associated with a risk of certain complications such as tendon attrition or even rupture, nerve injury, infection, hardware malfunction, loss of reduction, fracture malunion or nonunion, complex regional pain syndrome, and post-traumatic arthritis.5–8 Among these, flexor tendon rupture is a rare but serious complication. 9 , 10 The flexor pollicis longus (FPL) is the most frequently ruptured tendon, followed by the index flexor digitorum profundus. 11 , 12 Symptoms and signs of FPL attrition or rupture include pain and a rubbing sensation with movement, sometimes preceded by volar radial-sided wrist pain, volar wrist swelling, a popping or clicking sensation, and even an inability to flex the interphalangeal joint of the affected phalanx.13–16 In view of the above problems, we should strive to identify the risk factors for tendon attrition or rupture and to intervene accordingly.
The pathogenesis of FPL attrition or rupture after volar plating of distal radius fractures is multifactorial. Reported risk factors include excessive distal placement of the plate, increased prominence of the distal edge of the plate, prominent screw heads, inbuilt malreduction, and incorrect plate usage. 9 , 10 , 16 , 17 However, no studies have included the use of multiple regression analysis to explore the aforementioned possible factors. In the present study, binomial analysis combined with multivariate logistic regression analysis was performed to investigate the risk factors associated with FPL attrition or rupture. Based on previous studies by other research groups, we hypothesized that the type of plate used, the fracture reduction status, the plate position, whether the pronator quadratus is repaired, and the time of plate removal are significant risk factors associated with FPL attrition or rupture.
Materials and methods
We retrospectively reviewed the records of consecutive patients who underwent surgical repair involving volar plating from February 2011 to February 2018 at three hospitals. This study was approved by the institutional review board of our hospital (No. L-2011-22, 17 October 2011). Informed consent was obtained from all patients before the operation. The inclusion criteria were (1) age of ≥18 years, (2) a fresh closed distal radius fracture (within 14 days from injury), (3) no nerve/vascular/tendon injuries, (4) treatment with volar plating, and (5) available initial and post-reduction standard posteroanterior and lateral wrist radiographs. The exclusion criteria were (1) open fractures, (2) old fractures, (3) pathological fractures, (4) ipsilateral upper limb fractures and/or dislocation, (5) a history of ipsilateral upper limb surgery, and (6) incomplete follow-up data. In accordance with the inclusion and exclusion criteria, 338 patients were enrolled in the study. The reporting of this study conformed to the STROBE statement. 18 All patient details were de-identified.
Demographic information recorded at the time of the original injury included age, sex, fracture side, mechanism of injury, fracture classification, time from injury to surgery, operative approach, type of plate, fracture reduction status, plate position, repair of pronator quadratus, and timing of plate removal (<1 year (early) or ≥1 year). The fractures were classified using the OTA fracture classification system (type A, B, and C). Operative approaches included the classic Henry approach, the modified Henry approach, and the extended flexor carpi radialis approach. The different types of plates comprised the Synthes volar distal radius plate (Synthes, Solothurn, Switzerland), Sanatmetal volar anatomic plate (Sanatmetal, Eger, Hungary), and DVR anatomic plate (Zimmer Biomet, Warsaw, IN, USA). Volar tilt, radial tilt, radial height, and ulnar variance were measured to determine the status of fracture reduction. We measured the Soong grade for each patient according to the methods described by Soong et al. 9 (Figure 1). In addition to the Soong grade, we also chose two other parameters to analyze the position of the plate: the distance between the plate and the volar critical line (the plate-to-critical line distance (PCLD)) and the distance between the most distal extent of the plate and the most distal portion of the volar rim (the plate-to-volar rim distance (PVRD)) (Figure 2). Measurements of the Soong grade, PCLD, and PVRD were performed on standard lateral wrist plain radiographs using a picture archiving and communication system. Each of the radiographs was presented to three independent observers (all senior trainees in orthopedics) in a random fashion, blinding any identifying patient information. Each observer was instructed to measure the above-mentioned parameters from the radiographs. The three observers repeated their measurements in a similar fashion and were also blinded to the results of their first evaluation.

Radiograph illustrating the determination of plate prominence with use of the Soong grade.

Radiograph illustrating the measurements of the plate-to-critical line distance (PCLD) and plate-to-volar rim distance (PVRD). The PCLD is measured with negative values for plates dorsal to the critical line and positive values for prominent plates volar to the critical line. The PVRD is measured with positive numbers for plates proximal to the volar rim and negative values for plates distal to the volar rim.
The main outcome variable was the occurrence of asymptomatic tenosynovitis, symptomatic tenosynovitis, and FPL rupture. The diagnosis of tendon attrition or rupture was mainly clinical, ranging from localized swelling to severe pain and even to the inability to perform thumb flexion. Diagnosing rupture of the FPL was easier than diagnosing attrition of the FPL. We defined tendon attrition symptoms as pain or subdermal crepitus around the wrist during active thumb motion. We performed the tendon irritation test 19 to elicit signs of tendon attrition by keeping the patient’s wrist dorsally flexed at approximately 30° while placing our thumb on the radial side of the patient’s wrist. If we palpated subdermal crepitus on our thumb as the patient flexed and extended his or her thumb, we concluded that the tendon irritation test was positive. The tendon irritation test was performed by an independent observer. An ultrasound examination was performed to confirm tendon attrition or rupture in some equivocal cases.
Statistical analysis
Intraobserver reproducibility was assessed with computer-generated kappa statistics (SAS software; SAS Institute Inc., Cary, NC, USA). A kappa value of <0.00 indicated poor agreement, that of 0.00 to 0.20 indicated slight agreement, that of 0.21 to 0.40 indicated fair agreement, that of 0.41 to 0.60 indicated moderate agreement, that of 0.61 to 0.80 indicated substantial agreement, and that of 0.81 to 1.00 indicated excellent agreement. Student’s t test was performed to compare continuous variables, and the chi-square test was performed to compare categorical variables. A multivariate logistic model was fit for prediction of FPL tendon injury. All variables were included as possible predictors, and a final model was established using stepwise elimination. The level of statistical significance was set at P < 0.05.
Results
The data in this study were detected to be normally distributed. Statistical tests showed that the number of cases in this group exceeded the minimum sample size required for the study. Statistical analysis using the kappa coefficient was implemented to assess agreement between observers for the first and second showings. The kappa coefficients for the reported measurements of volar tilt, radial tilt, ulnar variance, radial height, Soong grade, PCLD, and PVRD showed substantial or excellent agreement for the first and second showings (Table 1). This supports the reproducibility of the measures that were used.
Intraobserver correlation coefficients demonstrating level of agreement in the measured variables.

CI, confidence interval; PCLD, plate-to-critical line distance; PVRD, plate-to-volar rim distance
Three hundred fifty-two patients were initially included, and 14 patients (about 4%) were lost to follow-up. Among the remaining 338 patients who underwent surgical treatment with volar plating, FPL attrition occurred in 18 (5.3%) patients and rupture occurred in 13 (3.8%) patients. FPL tendon rupture was seen between 5 and 96 months. According to the univariate analysis, sex (P = 0.022), volar tilt (P < 0.001), the Soong grade (P < 0.001), the PCLD (P < 0.001), the PVRD (P = 0.001), and the time of plate removal (P = 0.005) were significantly associated with FPL attrition or rupture (Table 2).
Patients’ baseline characteristics.

Data are presented as mean ± standard deviation or number of patients.
PCLD, plate-to-critical line distance; PVRD, plate-to-volar rim distance.
The results of the multivariate logistic regression analysis showed that decreased volar tilt (P = 0.005), Soong grade 2 (P = 0.008), a PCLD of >2 mm (P =0.029), a PVRD of <3 mm (P = 0.003), and plate removal at ≥1 year (P = 0.022) were significant risk factors for FPL attrition or rupture after volar plating of distal radius fractures (Table 3).
Multivariate logistic regression analysis.
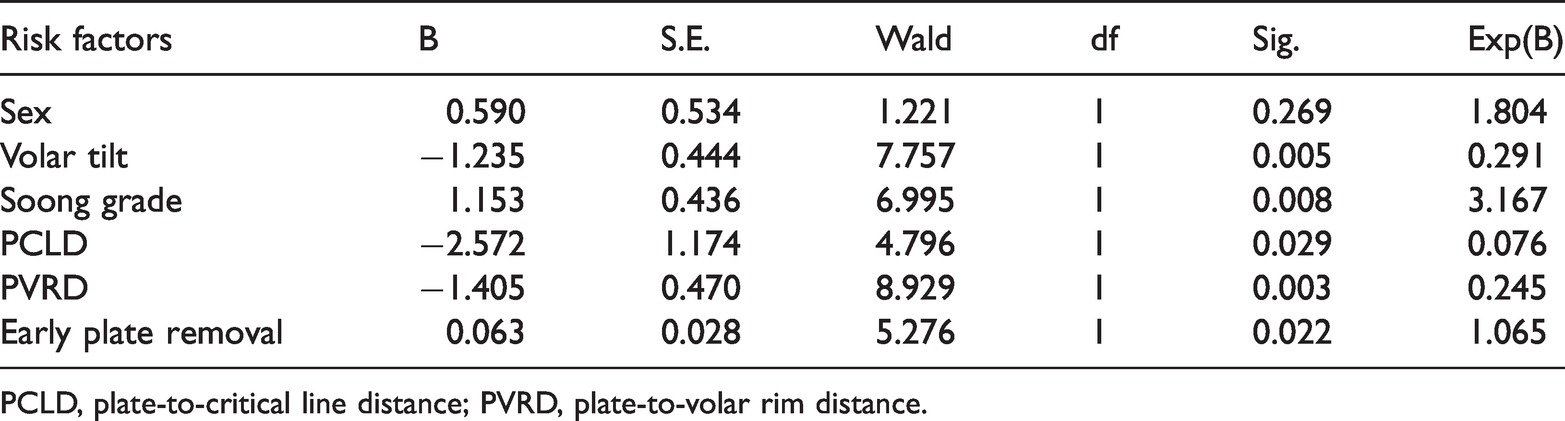
PCLD, plate-to-critical line distance; PVRD, plate-to-volar rim distance.
Discussion
Rupture of the FPL is a known complication of distal radius fractures. The rate of FPL tendon rupture widely ranges from 0.3% to 12% as reported in the literature. 1 , 3 , 4 , 16 ,20–23 Some authors have reported very low rates of tendon rupture. 4 , 24 In clinical practice, however, the incidence of tendon rupture might be higher than this because some patients with FPL rupture may present to other hospitals and others may not seek medical attention. In the present series, FPL attrition occurred in 5.3% (18/338) and rupture in 3.8% (13/338) of the patients. The tendon-related complication rate in this study was within the range reported in previous literature. In the present study, fracture malreduction, plate malpositioning, and plate removal at ≥1 year were the three risk factors associated with FPL attrition or rupture after volar plating of distal radius fractures, which basically verifies our hypothesis. However, different plate designs and whether the pronator quadratus is repaired were not significantly associated with FPL attrition or rupture.
Fracture malreduction as a generally known risk factor for FPL rupture. 2 ,25–28 Orbay and Touhami 2 reported that flexor tendon problems can occur if fracture reduction is lost. Stepan et al. 25 found that postoperative volar tilt significantly reduced the likelihood and amount of FPL tendon–plate contact on ultrasound examination. Wurtzel et al. 28 also demonstrated that the volar tilt was a significant factor in determining the risk of contact between the FPL and the fixation plate. In contrast to the above studies, Selvan et al. 26 emphasized the importance of the radial tilt. If the radial tilt was <25°, the risk of FPL rupture increased. Our results also demonstrated that reduced volar tilt was an independent risk factor for FPL attrition or rupture but that ulnar variance, radial height, and radial tilt were not. We believe that decreased volar tilt is more likely to cause plate prominence on lateral radiographs than reduced radial tilt. In addition, fixed, dorsally tilted fracture fragments of the distal radius increase the volar rim prominence. This might lead to greater contact between the plate and the FPL and thus increase the risk of rupture because of the direct force during the initial injury or prolonged irritation over time from the volar lip prominence. Furthermore, if the distal fragment is tilted in a dorsal position, the alignment of the carpal canal and the trajectory of the FPL would likely be more extended relative to the forearm axis. 28 This change in trajectory causes dorsal displacement of the FPL, further closing the space between the tendon and the volar plate.
The watershed line 2 and the Soong grade 9 are two of the more commonly used means of assessing plate position on the radius. The watershed line is a transverse ridge that lies distal to the pronator quadratus muscle and is located within 2 mm of the joint line on the ulnar side of the radius, 10 to 15 mm from the articular surface on the radial side of the bone. 29 A volar plate that is placed distal to the watershed line could potentially impinge on the traversing flexor tendons, resulting in irritation or rupture. Agnew et al. 30 demonstrated that placement of a plate 3 mm proximal to the watershed line posed a high risk of direct contact with the flexor tendons by magnetic resonance imaging. Kitay et al. 31 found that patients with flexor tendon rupture tended to have plates positioned 2 mm anterior to the volar critical line and <3 mm proximal to the volar rim. Our study corroborates their findings, and their report is the reason for us choosing the distance of 2 mm (PCLD) and 3 mm (PVRD) in our study. The Soong grade has also been discussed as a predictor of flexor tendon irritation or rupture. Previous research has confirmed that higher Soong grades are associated with significantly more flexor tendon complications. 9 , 12 , 28 , 31 Our results further confirmed that both the Soong grade and the quantitative measurements of PCLD and PVRD can help surgeons identify patients at risk for tendon rupture. Patients with Soong grade 2 plates have an increased risk of rupture, as do patients with distal plates that extend within 3.0 mm of the volar rim (PVRD of <3.0 mm) or >2.0 mm volar to the critical line (PCLD of >2.0 mm). All of these findings stress the importance of the plate position.
The time to presentation of FPL rupture varies widely, potentially occurring at any point following volar plate fixation and ranging from 4 to 120 months in the literature. 16 , 21 , 32 Tendon irritation is likely to appear before tendon rupture. Therefore, FPL rupture might be prevented by selective plate removal in patients with tendon irritation. 33 , 34 To explore the FPL mobility, Nanno et al. 35 compared the movement of the FPL on the distal radius during wrist and finger motions using transverse ultrasound before and after removal of a volar plate in patients with distal radius fractures. They found that the FPL had greater mobility after removal of the plate. These variations of the FPL movement patterns can help to depict the release of any adhesion between the FPL and the pronator quadratus on the distal radius and to confirm the efficacy of removing the plate. Therefore, to decrease the risk of rupture, we recommend considering elective hardware removal after union in symptomatic patients, especially for patients with plate prominence of >2.0 mm volar to the critical line (PCLD of >2 mm), plate position within 3.0 mm of the volar rim (PVRD of <3 mm), or lateral radiographs showing prominence of the plate beyond the volar rim (Soong grade 2).
The clinical importance of certain factors, such as age, sex, different plate designs, and whether the pronator quadratus is repaired, remains controversial. A systematic review showed that more than one-third of the population (37%) with flexor tendon rupture were between 60 and 70 years of age, and women (n = 23) were affected almost twice as often as men (n = 11). 24 This can be explained by the higher incidence of distal radius fracture among women secondary to osteoporosis with increasing age. 24 , 26 The decrease in the tensile properties of the tendon with age might also make it more susceptible to attritional wear against the prominent plate edge. However, in the present study, the multivariate logistic regression analysis showed no significant correlation of age and sex with FPL rupture. Thus, further research is needed. Hinchcliff et al. 37 found that the volar plate design did not significantly impact either the mean or median force between the plate and the flexor tendons. However, Limthongthang et al. 11 found that a plate with a Y-shaped design (the FPL plate), in which the bridging segment of the plate between the radial and intermediate columns had been removed, had a significantly smaller contact area between the plate and the FPL relative to other plates. The hospitals involved in the present study did not have the FPL plate; thus, we could not reach the above conclusion. Some investigators have advocated repairing the pronator quadratus as a preventative measure, providing a protective tissue layer between the volar plate and the flexor tendons to prevent the tendons from rubbing directly against the plate. 33 , 38 We doubt the effect of this repair technique. Many distal radius fractures can lead to pronator quadratus damage during the initial injury, making repair difficult. This repair technique might increase the adhesion between the FPL and the pronator quadratus on the distal radius.
A main limitation of this study is its retrospective design; the accuracy of the demographic information was mainly dependent upon documentation. Another limitation is that although we found no difference in FPL rupture in relation to the three different plates used, we acknowledge that there might be differences in the rate of tendon rupture among the plates. However, we were not able to detect such differences because of the small number of plate types used. A third limitation is that although many factors were considered in this study, there were still some factors that could not be fully incorporated, such as the position of the wrist, 28 prominence of the screw heads, 3 displacement of the distal ulna, and the distal radioulnar dissociation. 39 Finally, although three independent observers repeatedly measured the relevant parameters, it was still difficult to completely eliminate errors.
Conclusion
Reduced volar tilt, Soong grade 2, PCLD of >2 mm, and PVRD of <3 mm were risk factors significantly associated with FPL attrition or rupture in this study. The findings of this study also suggest that the risk of tendon rupture is lower if a Soong grade 2 plate is removed, the PCLD is >2 mm, the PVRD is <3 mm, or reduced volar tilt is achieved earlier (at <1 year). In addition, we recommend that clinicians plan to remove the plate when signs of symptomatic tenosynovitis (swelling and pain) are noted in the clinical examination.