
Abstract
The most common osseous metastatic regions for colorectal cancer are the lumbar and sacral vertebrae and the pelvis. There are few reported cases of isolated solitary tibial metastasis, and simultaneous bilateral solitary tibial metastases in colorectal cancer are even rarer. A 62-year-old female patient was admitted to our inpatient clinic 3 years after receiving initial chemotherapy for a rectosigmoid adenocarcinoma with liver metastasis. The patient complained of left leg pain. Radiographs and magnetic resonance imaging revealed a 3- × 3-cm mass in the right proximal tibia and a 2- × 7-cm mass in the middle third of the left tibia; both were highly suggestive of bone metastases. Bilateral tibial metastases were confirmed after tumor excision and prophylactic open reduction and internal fixation. The postoperative course was relatively uneventful. Colorectal cancer with bone metastases is uncommon, and most metastases are found at a single site in an extremity. We believe this is the first published case of simultaneous bilateral tibial metastases in a patient with colorectal cancer.
Introduction
Colorectal cancer is a major public health burden and the third leading cause of cancer-associated deaths worldwide. 1 Organs, such as the liver and lungs, are the most common sites of distant metastases. Patients with bone metastases have a poor prognosis, with a median survival of <10 months.2,3 The incidence of osseous metastases from colorectal cancer is reportedly between 4.7% and 10.9% in clinical cases. In autopsy case series, incidence rates of 10.7% to 23.7% were observed.1,2,4–7
Considering the anatomical proximity of the colon to the paravertebral venous plexuses, the most common bone metastatic regions are the lumbar and sacral vertebrae, and the pelvis. 4 There are few reported cases of isolated solitary tibial metastasis,2,4,7 and simultaneous bilateral solitary tibial metastases in colorectal cancer are even rarer. To the best of our knowledge, this patient is the first reported case of simultaneous bilateral solitary tibial metastases of colorectal cancer.
Case report
In April 2015, a 62-year-old woman was admitted to our inpatient clinic with a suspected rectosigmoid adenocarcinoma with liver metastasis. The patient underwent low-anterior resection and liver tumor resection. Pathological examination confirmed pT4bN2bM1a, stage IVa cancer, and 12 cycles of Avastin-FOLFIRI adjuvant chemotherapy (bevacizumab, leucovorin-calcium, fluorouracil, irinotecan hydrochloride) were administered, followed by the leucovorin, fluorouracil and oxaliplatin (FOLFOX) 7 regimen for tumor recurrence 1 month later. The patient tolerated chemotherapy well and was asymptomatic until July 2018, when she came to our clinic with a chief complaint of left leg pain that was aggravated by standing or walking. Mild limited range of motion owing to dull pain was also reported. No traumatic event was mentioned. Radiography showed cortical erosion with periosteal reaction in the left tibial shaft, which was highly suggestive of tumor involvement (Figure 1).

Preoperative radiographs. The left tibial shaft has cortical erosion with periosteal reaction (1.5 × 6 cm) (white arrow). (a) anterior-posterior view; (b) lateral view.
Magnetic resonance imaging of the legs illustrated a 3- × 3-cm mass located in the right proximal tibia and a 2- × 7-cm mass in the middle third of the left tibia; both were highly suggestive of bone metastases (Figure 2). Although preoperative positron emission tomography-computed tomography (PET-CT) was ordered, the examination was not completed because of the patient’s concern about the amount of radiation and because her health insurance did not totally cover the examination fee. The preoperative Eastern Cooperative Oncology Group (ECOG) performance status was grade one, and estimated survival was approximately 8 months in unselected patients after diagnosis of bone metastases in colorectal cancer, with a 5.7% 5-year survival rate. 8 , 9 Therefore, the main concern was intolerable pain under the maximum pain medication dose. Owing to the relatively high risk of sustaining a pathological fracture according to Mirels’ scoring system, 10 prophylactic internal fixation was indicated and performed.

Bilateral lower limb magnetic resonance imaging. (a) T1-weighted turbo spin echo image showing a 3- × 3-cm mass located in the right proximal tibia and a 2- × 7-cm mass in the left middle third of the tibia; both masses were highly suspicious for bone metastases (white arrow). (b) Right leg T2-weighted short-tau inversion recovery (STIR) image showing a tumor-like lesion in the proximal tibial bone marrow (white arrow). (c) Left leg T2 STIR image showing a tumor-like lesion in the tibial shaft bone marrow (white arrow).
The right leg tumor was surgically excised, and bone curettage was performed, with 95% alcohol irrigation. The bone defect was then grafted with bone cement. The right tibia was fixed with a lateral buttress plate, and the left tibia was fixed with an intramedullary nail (the right and left tibia were operated separately) (Figure 3). Whole-body technetium 99m bone scans were performed 3 weeks after the operation and showed uptake signals around the coccyx and bilateral tibia mixed with postoperative changes (Figure 4).
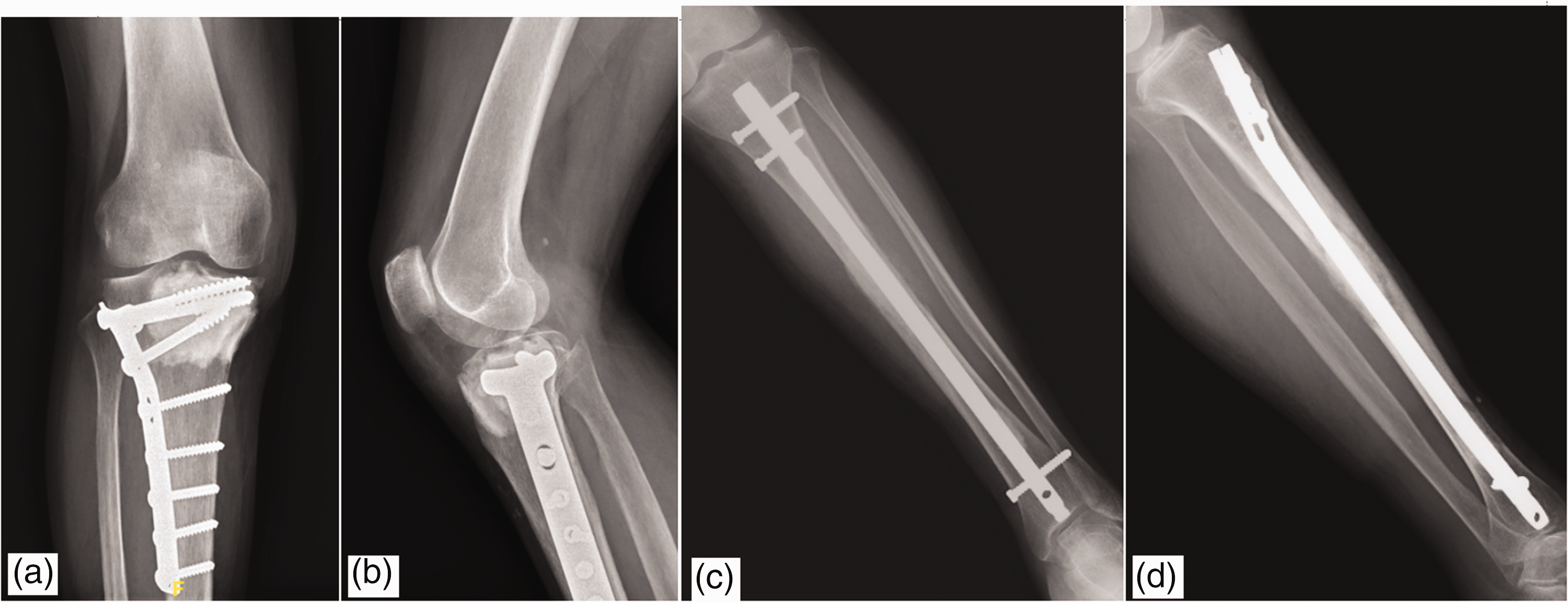
Postoperative radiographs. We performed tumor excision accompanied by 95% alcohol irrigation and prophylactic internal fixation with a lateral buttress plate (8H6S) in the right tibia (a, b) and a prophylactic intramedullary nail in the left tibia (c, d) (the right and left tibia were operated separately).
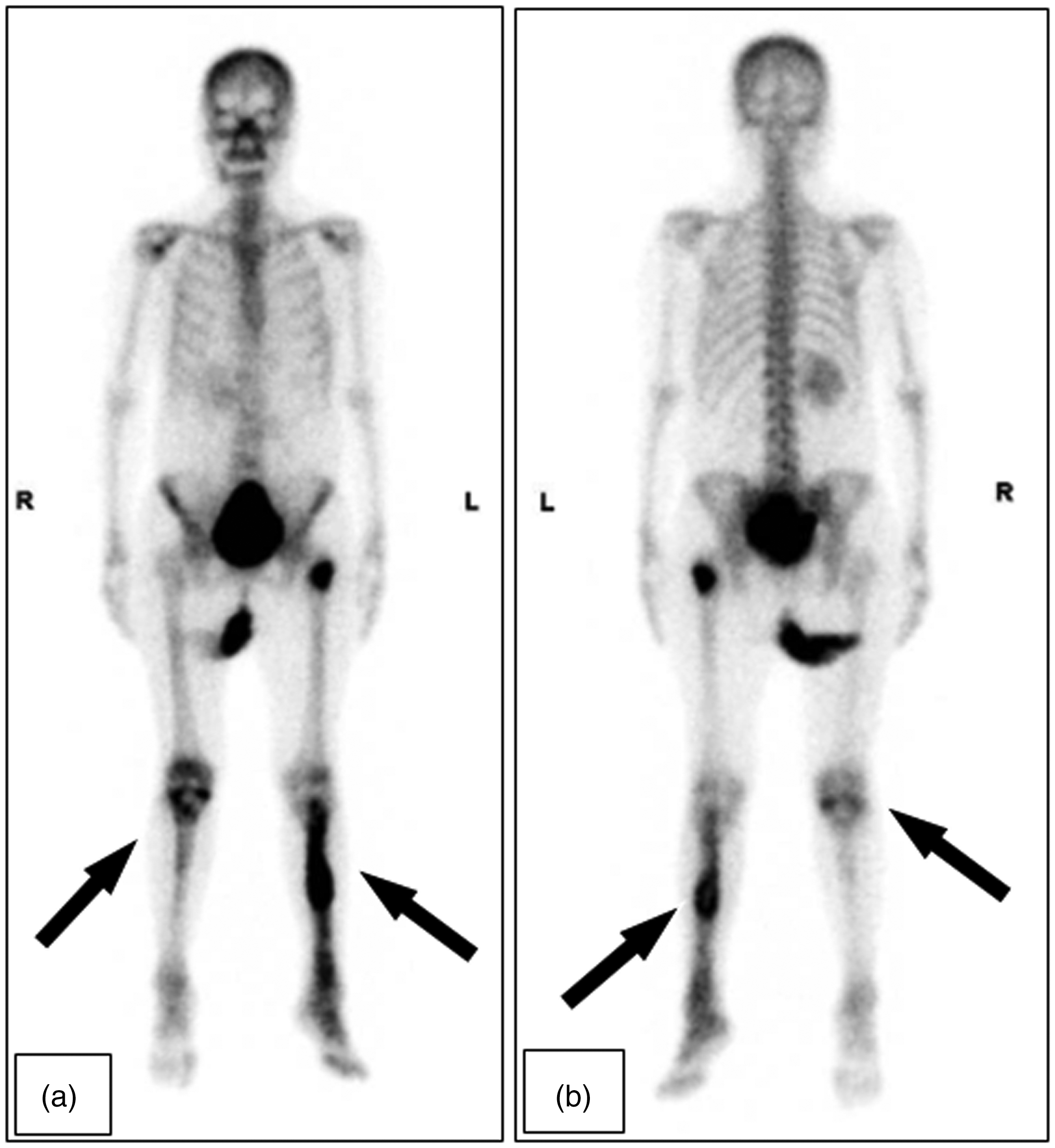
Whole-body bone technetium 99 m scans. Postoperative technetium 99 m scans showing uptake signals around the coccyx and bilateral tibia (black arrows). (a) anterior view; (b) posterior view.
The postoperative course was relatively uneventful, with right leg splinting and ambulation with partial weight-bearing. The preoperative left leg pain subsided, and the patient underwent early active range of motion exercises after immobilization with a left long leg splint for 3 weeks. Further adjuvant radiotherapy was scheduled. Pathology reports for both legs indicated metastatic adenocarcinoma of colorectal origin. The bilateral tibial pathological results are presented in Figure 5.
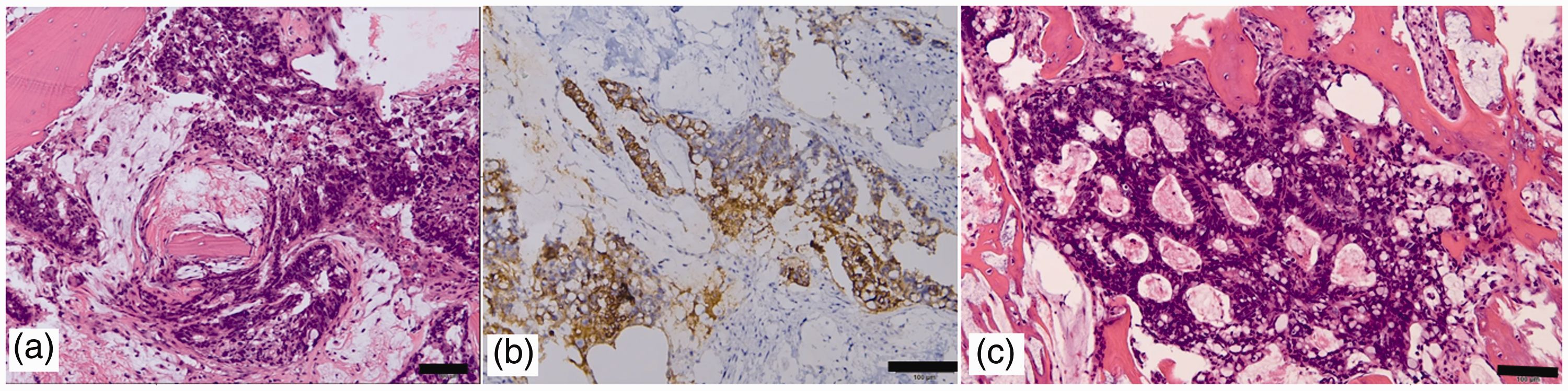
Right tibial pathological and immunohistochemical analysis of the biopsy specimen. (a) Microscopically, the sections show metastatic carcinoma composed of hyperchromatic columnar cells with intracellular mucin infiltrating the bone marrow spaces in a complex glandular pattern (scale bar: 100 mm). (b) Immunohistochemically, the neoplastic cells stained positive for cytokeratin (CK)20, and negative for CK7, estrogen receptor (ER), and thyroid transcription factor-1 (TTF-1) (scale bar: 100 mm). (c) Left tibia pathological and immunohistochemical analysis of the biopsy specimen. Microscopically, metastatic adenocarcinoma in a glandular pattern and focal mucin production are seen (scale bar: 100 mm).
Discussion
Bone metastases occur frequently in patients with breast, prostate, multiple myeloma, and lung cancer. Osseous metastases are much less frequent in colorectal cancer cases. 4 Colorectal cancer commonly metastasizes to the liver (>70%), lungs (20%–30%), and peritoneum. In contrast, bone metastasis is uncommon (4.7%–10.9% in clinical cases) and often indicates advanced disease with a poor prognosis (5-year survival rate <5%). 11 Pathologic detection of signet-ring cells appears to be associated with a high incidence of bone metastases. 12
The first reported case of solitary tibial metastasis in a patient with colon cancer was published by Kose in 2009. 4 One study by Kanthan et al., 13 using bone scans and plain radiography, retrospectively reviewed 5352 cases of primary colorectal carcinoma and found a very low incidence (1.1%) of isolated solitary skeletal metastases.
Metastatic colorectal cancer is usually osteolytic or mixed osteolytic/osteoblastic. 14 The tumor may be deposited on cortical or cancellous bone. 3 Clinically, in the early stages, patients are sometimes asymptomatic. However, bone metastases can lead to widespread symptoms, such as pain (usually unrelieved with nonsteroidal anti-inflammatory drugs), 15 nerve compression, and even pathological fractures. The most commonly involved metastatic bony sites are the spine (65%), hip/pelvis (34%), long bones (26%), and other sites (17%).11,16 A valveless drainage system of veins named Batson's plexus is thought to be the most likely route of skeletal seeding because of the connection between the spinal veins around the lumbar region and the iliofemoral venous system. 17 Interestingly, irinotecan or oxaliplatin exposure during treatment is thought to be associated with an increased incidence of osseous metastases. 12 Some authors believe that the increasing incidence associated with irinotecan or oxaliplatin exposure was correlated with the improved survival rate of patients who received irinotecan or oxaliplatin for metastatic colorectal carcinoma treatement. 4 Additionally, improved radiological and PET scan equipment were considered important for increased early detection. 3 In our case, the patient had received several cycles of irinotecan therapy.
Bone scan is considered the most effective method for early detection of occult osseous metastases 1 because some bone metastases are asymptomatic in the early stages. In a retrospective study, Santini et al., 2 reported an average duration of 11 months between making a diagnosis of primary colorectal cancer and detecting osseous metastases.
Our case is classified as metachronous bone metastasis because bone metastasis was detected 3 years after the initial diagnosis of colorectal cancer. Owing to a poor 5-year prognosis and survival of approximately 8 months in unselected patients after a diagnosis of bone metastases in colorectal cancer, 9 our case stresses relieving intolerable pain and providing a return to bilateral lower limb function to support daily activities and improve quality of life, as first considerations.
Preoperative potential bone reconstruction strategies for the middle tibial shaft include bone allograft transplantation and a custom prosthesis. Bone allograft transplantation may be considered if the lesion site has marked unreducible cortical destruction resulting in unstable bridging length by plating or nailing intraoperatively. A custom prosthesis can be considered if a pathological fracture extends to the joint line and the fracture is non-reducible after tumor excision. Our patient underwent plating and interlocking nail after tumor excision because the bone defect was controlled, with no shortening or rotation deformity after tumor excision. Unfortunately, the patient died owing to multiorgan failure without bilateral tibial bone pain complaints 1.5 years after the operation.
Colorectal cancer with bone metastasis is uncommon (4.7%), and most cases are found at a single site in an extremity. Simultaneous bilateral tibial metastases, as presented in our case, are extremely rare. Early detection of bone metastases significantly improves prognosis; thus, routine bone scan screening is suggested in patients with advanced colorectal cancer.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211027773 - Supplemental material for Colorectal cancer with first known case of simultaneous bilateral tibial metastases
Supplemental material, sj-pdf-1-imr-10.1177_03000605211027773 for Colorectal cancer with first known case of simultaneous bilateral tibial metastases by Ta Li Hsu and Karl Wu in Journal of International Medical Research
Footnotes
Acknowledgment
We greatly thank all the members of FEMH Orthopaedic Department of Surgery.
Ethics statement
The Research Ethics Review Committee of the Far Eastern Memorial Hospital waives the requirement for ethical approval of case reports. We obtained verbal informed consent from the patient, and she confirmed that she understood that her diagnosis, data, and treatment course were being collected for publication. Additionally, we completely deidentified all patient details, and this case report conforms to the CARE guidelines. 17 Written informed consent was obtained from the patient for the publication of this case report and the associated images.
Availability of data and materials
All data associated with the case are presented in the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.