
Abstract
Objective
To compare the accuracy of multi-slice spiral computerized tomography (MSCT) with colonoscopy for diagnosing synchronous colorectal carcinoma (SCC).
Methods
We retrospectively analyzed all consecutive patients admitted to our institution with colorectal carcinoma between 19 September 2014 and 31 January 2020. Data on SCC patients who had undergone MSCT and colonoscopy were analyzed. Information on tumor location, tumor size, missed diagnosis by MSCT or colonoscopy, T stage, pathological type, and reasons for missed diagnosis was recorded and used to assess the diagnostic accuracies of MSCT and colonoscopy.
Results
Twenty-three cases met the inclusion criteria. MSCT plus colonoscopy had a significantly higher diagnostic accuracy (93.5%) than colonoscopy alone. There were significant differences in missed diagnosis rates of proximal cancer (34.8%) and distal cancer (4.3%) by colonoscopy. For MSCT, the missed diagnosis rate for tumors with a median long diameter of 1.25 cm (interquartile range 0.80, 1.50) was significantly lower than that for larger tumors (long diameter 4.00 cm; 3.00, 6.00).
Conclusions
MSCT is a valuable diagnostic tool for SCC that can effectively minimize the missed diagnosis rate of primary tumors when combined with colonoscopy.
Introduction
Synchronous colorectal carcinoma (SCC) is defined as two or more primary colorectal cancers occurring simultaneously or within 6 months after the first colorectal cancer. 1 Although the detection of multiple primary malignant neoplasms is rare, recent advances have gradually increased their detection rate. The incidence of synchronous multiple primary cancers ranges from 1% to 8%, 2 while that of metachronous multiple primary cancers is 0.18% to 9%. 3
SCC and single colorectal cancer have similar prognoses in terms of accurate diagnosis and surgical resection. 4 A missed cancer diagnosis thus has serious implications, and high diagnostic accuracy significantly improves the survival rates and prognoses. Multi-slice spiral computerized tomography (MSCT) and colonoscopy are widely used to localize, diagnose, stage, and preoperatively assess colorectal cancer. However, most studies of MSCT have focused on single tumors,5 –13 and few have studied its use in SCC.1,14 –16 Various factors can affect colonoscopy, including failure to reach the cecum and view the entire colon, which may in turn contribute to a missed diagnosis.17,18 We encounter a high missed diagnosis rate of SCC in the first colonoscopy in our daily practice, while MSCT performs well for diagnosing SCC.
In this study, we retrospectively analyzed data from SCC patients who had undergone MSCT and colonoscopy. We compared the approaches in terms of diagnostic accuracy, missed diagnosis rates of proximal and distal parts of SCCs, the causes of missed diagnosis, and impacts of tumor T stage and pathological type on the missed diagnosis.
Materials and methods
The reporting of this study conforms to the STROBE guidelines. 19
Study population
We retrospectively analyzed all consecutive patients (n = 2909) admitted for colorectal carcinoma between 19 September 2014 and 31 January 2020, and collected data for patients with synchronous multiple primary colorectal carcinomas who had complete clinical and imaging data available at our institute (The Affiliated Traditional Chinese Medicine Hospital of Southwest Medical University). The diagnostic inclusion criteria were: 1) cancer diagnosis confirmed by pathology; 2) colorectal cancers diagnosed at the same time or within 6 months; 3) tumors located in different intestinal segments or adjacent intestinal segments (if in the same intestinal segment, tumors had to be of different pathological types, or at least 2 cm apart); 4) each tumor had pathological features and transfer pathways; and 5) T stage Tis or T1 to 4. The exclusion criteria were: 1) colorectal cancers with local recurrences; 2) patients with ulcerative colitis or familial adenomatous polyposis; and 3) T stage TX or T0. This was a retrospective study that did not require approval by the institutional ethics committee, and the need for informed consent was waived.
MSCT scanning device
CT scans were carried out using a second-generation dual-source CT (Somatom Definition Flash, Siemens, Forchheim, Germany) following intravenous injection of contrast material, with the following scanning parameters: voltage: 120 kV; current: 350 mA, thickness and layer spacing: 5 mm. The images were reconstructed using 1-mm overlapping slice thickness and 1-mm intervals and loaded onto the picture archiving and communications system (syngo.via workstation; Siemens). Scans were conducted using 80 to 100 mL of a contrast agent with an iodine content of 370 mg/mL (Ultravist 370, Bayer, Berlin, Germany) administered at a flow rate of 3.0 mL/s.
Bowel preparation was carried out prior to colonoscopy. The day before the examination, all patients were advised to eat a light and easily digestible diet and to avoid indigestible food (e.g. maize, potato, peanut, apple, pear, grape, shiitake mushroom, flammulina). At 4 to 6 hours before the examination, all patients were then instructed to take 2 to 3 L (250 mL/10 minutes) isotonic solution mixed with polyethylene glycol electrolyte powder within 2 hours. The patients were asked to walk appropriately during the medication period and then press their abdomen lightly to speed up excretion. If the patient was admitted for intestinal obstruction, colonoscopy was completed after releasing the intestinal obstruction.
Two senior radiologists viewed and recorded the general data for the SCC patients and the location and size of the tumors. They also recorded missed diagnoses for MSCT and the first colonoscopy, and assessed the reasons for the missed diagnosis of SCC. Tumor T stage and pathological type were evaluated by a senior pathologist.
Tumors were grouped as follows: right-sided colon (cecum, ascending colon, and right half of the transverse colon), left-sided colon (left half of transverse colon and descending colon), and rectosigmoid colon (rectum and sigmoid colon).
Statistical analysis
All data were analyzed using IBM SPSS Statistics for Windows, version 21 (IBM Corp., Armonk, NY, USA). Measured data with a normal distribution were expressed as mean ± standard deviation and differences between two groups were compared by independent-sample t-tests. Non-normally distributed data and graded data were expressed as median and quartiles (Q1; Q3), and differences between two groups were compared by the Mann–Whitney U test. Counted data were compared between paired samples using McNemar’s test and between independent samples using the χ2 test. All statistical tests were two-sided with a test level (α) of 0.05. Causes of missed diagnoses according to the two methods were evaluated based on the frequency of occurrence.
Results
Twenty-three patients met the inclusion criteria (Figure 1), including 18 men and 5 women (mean age 66.2 years (range 33–82 years). Sixteen patients had a history of smoking and 12 had a history of alcohol consumption. Clinically, the main presentations were abdominal pain and changes in stool characteristics. One patient had intussusception and six had ileus. Fifteen patients were positive for tumor markers, including CEA, CA125, CA19-9, and CA72-4.

Flow diagram of the study.
Of the 23 SCC patients, 3 were in the right-sided colon group (1 ascending colon and ascending colon cancer and 2 hepatic flexure and transverse colon cancer), 1 was in the right and left-sided colon groups (ascending colon and splenic flexure cancer), 7 were in the right-sided and rectosigmoid colon groups (Figures 2 and 3) (1 ascending colon and sigmoid colon cancer, 1 ascending colon and rectal cancer, 1 hepatic flexure and sigmoid colon cancer, 2 hepatic flexure and rectal cancer, 2 transverse colon and rectal cancer), 2 were in the left-sided and rectosigmoid colon groups (1 transverse colon and rectal cancer and one splenic flexure and sigmoid colon cancer), and 7 were in the rectosigmoid colon group (1 sigmoid colon and sigmoid colon cancer, 3 sigmoid colon and rectal cancer, and 3 rectal and rectal cancer).

A 33-year-old man with synchronous malignant adenoma transformation in the sigmoid colon (Tis stage, 8 × 4 cm) and eminence-type adenocarcinoma with mucinous adenocarcinoma in the transverse colon (T3 stage, 4 × 4 cm), complicated by intussusception. (a, b) Axial and coronal contrast-enhanced computed tomography (CT) images showing slightly lower density mass involving the transverse colon in intussusception. (c) Axial contrast-enhanced CT image showing a mass with homogeneous and obvious enhancement involving the sigmoid colon, causing luminal stenosis. (d) Colonoscopy image showing a mass in the sigmoid colon; however, the colonoscope was unable to pass through the mass, resulting in a missed diagnosis in the transverse colon.

A 79-year-old woman with synchronous ulcer-type adenocarcinoma in the transverse colon (Tis stage, 6 × 8 cm) and eminence-type adenocarcinoma in the rectum (Tis stage, 1 × 1.5 cm). However, the adenocarcinoma in the transverse colon was diagnosed 5 months after diagnosis of the rectum adenocarcinoma by computed tomography (CT) and colonoscopy. (a) Axial contrast-enhanced CT image showing a mass with homogeneous enhancement involving the rectum, resulting in luminal stenosis. (b) Axial contrast-enhanced CT image showing a suspiciously thickened colon wall (white arrow) in the transverse colon disturbed by colorectal contraction and a high amount of colonic content. (c) Colonoscopy revealed a mass in the rectum; however, the colonoscope was unable to pass through the mass, resulting in a missed diagnosis in the transverse colon.
Of the 46 colorectal cancers, 35 were adenocarcinomas (Figures 2 and 3) (5 protruded-type adenocarcinoma with mucinous adenocarcinomas, 17 ulcer-type adenocarcinomas, 12 protruded-type adenocarcinomas, and 1 ulcer-type mucinous adenocarcinoma), and 11 patients had malignant adenoma transformations (Figure 2). Of the 46 colorectal cancers, 14 patients were Tis stage, 1 was T1 stage, 13 were T2 stage, 16 were T3 stage, and 2 patients were T4 stage.
Of the 46 SCC tumors, MSCT missed the diagnosis in 4 cases (8.7%), including 1 ascending colon cancer, 1 transverse colon cancer, and 2 sigmoid colon cancers. Colonoscopy missed the diagnosis in nine cases (19.6%), including eight proximal cancers (2 ascending colon cancers, 2 hepatic flexure cancers, 1 transverse colon cancer, and 3 sigmoid colon cancers) (Figure 2 and 3) and one distal carcinoma (sigmoid colon cancer).
MSCT and colonoscopy exhibited diagnostic accuracies of 91.3% and 80.4%, respectively, according to McNemar’s test, but the difference in diagnostic accuracy was not significant (Table 1). The combination of MSCT and colonoscopy had a diagnostic accuracy of 93.5%, which was significantly higher than that of colonoscopy alone (P = 0.031; Table 2), but not significantly different from that of MSCT alone (Table 3).
Diagnostic accuracies of multi-slice spiral computerized tomography versus colonoscopy.

+, diagnosis; −, missed diagnosis; MSCT, multi-slice spiral computerized tomography.
Diagnostic accuracies of colonoscopy with and without multi-slice spiral computerized tomography.

+, diagnosis; −, missed diagnosis; MSCT, multi-slice spiral computerized tomography.
Diagnostic accuracies of multi-slice spiral computerized tomography with and without colonoscopy.

+, diagnosis; −, missed diagnosis; MSCT, multi-slice spiral computerized tomography.
There was a significant difference (corrected χ2 = 4.675, P = 0.031) in missed diagnosis rates between proximal (34.8%) and distal cancers (4.3%) for colonoscopy (Table 4). There was also a significant difference in missed diagnosis rates between smaller tumors (median long diameter 1.25 cm (0.80, 1.50)) and larger tumors (median long diameter 4.00 cm (3.00, 6.00)) for MSCT (Z = −3.235, P = 0.001) (Table 5). However, there were no significant differences in missed diagnosis rates of tumors in relation to T stage or pathological type for MSCT or colonoscopy (Table 6).
Missed diagnoses of distal versus proximal cancers of the colon by colonoscopy (corrected χ2 test).

Diagnosis in relation to size of colon tumor size by multi-slice spiral computerized tomography (rank sum test).

Impacts of tumor T stage and pathological type on missed diagnosis by multi-slice spiral computerized tomography and colonoscopy (corrected χ2 test).
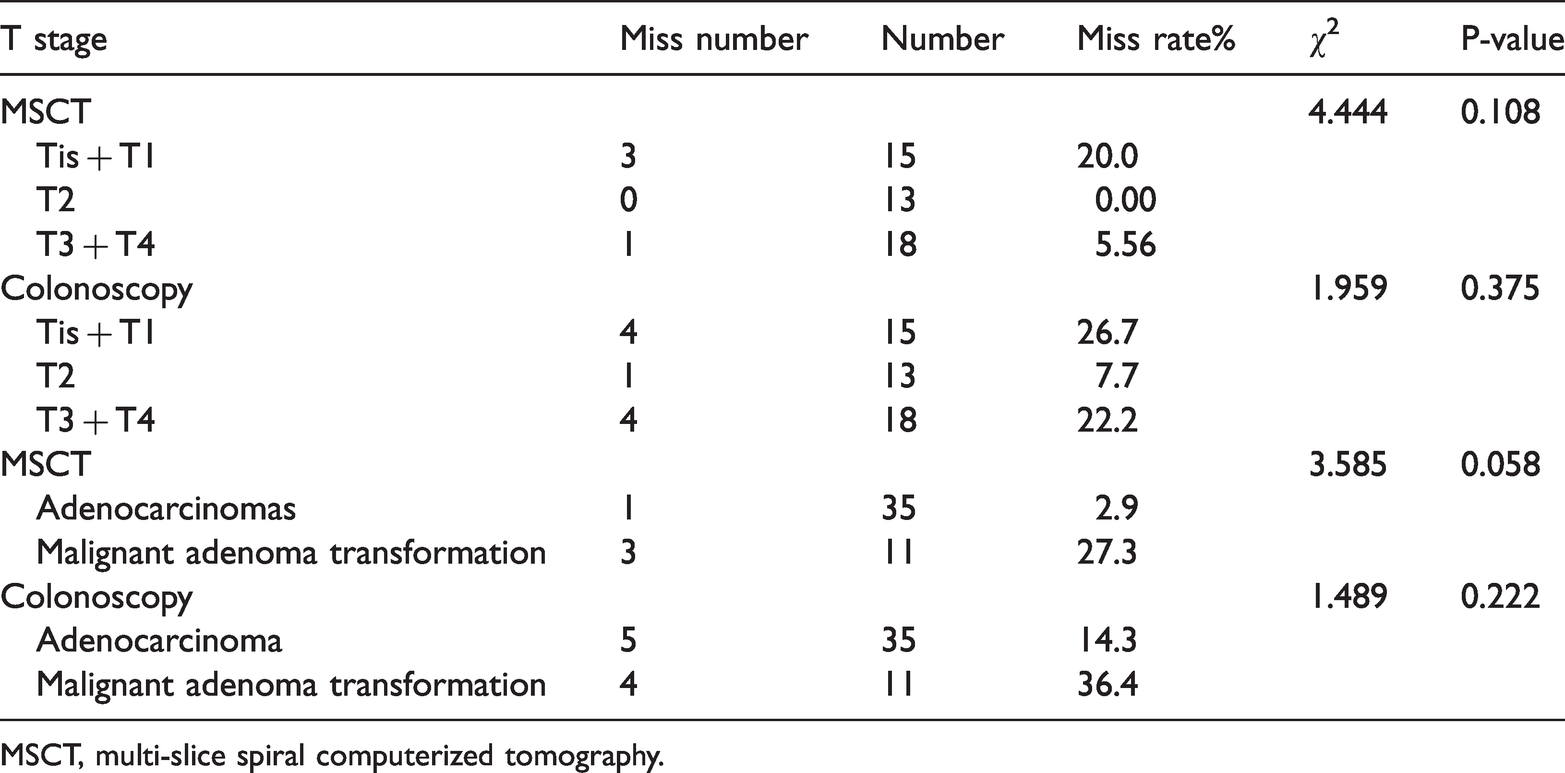
MSCT, multi-slice spiral computerized tomography.
Missed diagnoses on MSCT resulted from the round or oval shape and the small volume of the tumors (Figure 3) and technical factors (excessive intestinal content and colon contraction) (Table 6), and missed diagnoses for colonoscopy were caused by poor bowel preparation (Figures 2 and 3) and failure of the colonoscope to pass through the stricture caused by the tumor (Table 7) (Figure 2).
Missed diagnoses by multi-slice spiral computerized tomography and colonoscopy.

MSCT, multi-slice spiral computerized tomography.
Discussion
This study showed that combining MSCT and colonoscopy could effectively reduce the rate of missed diagnoses of SCC. Colonoscopy mainly missed the diagnosis of tumors in the proximal colon. The missed diagnosis rate of SCC for MSCT in relation to tumor size was low. Missed diagnoses on MSCT were mainly caused by the round or oval shape and small volume of the tumors and by technical factors (excessive intestinal content and colon contraction), while missed diagnoses for colonoscopy were due to poor bowel preparation and failure of the colonoscope to pass through the stricture caused by the tumor.
Our analysis suggested that advanced age, smoking history, alcohol consumption, and male sex were risk factors for SCC, consistent with previous findings.4,20
Preoperative MSCT is crucial for precise localization of the lesion during SCC diagnosis. Laparoscopic surgery has been widely used to treat colorectal cancer21 –23; however, palpation and colonoscopy may fail to accurately locate the tumor, 24 especially in the descending colon, due to colonic stenosis and SCC localization in different segments.1,6 MSCT may aid preoperative planning and precise positioning in these cases.
The current data showed that the combination of MSCT and colonoscopy was superior to colonoscopy alone for diagnosing SCC. Although colonoscopy is highly efficient for diagnosing colon cancer, it has some limitations1,14 due to colonic elongation, colonic tortuosity, advanced diverticular disease, poor bowel preparation, colonic obstruction, and colonic stenosis, which may contribute to a missed diagnosis.17,18 In contrast, MSCT has multiple advantages for colon cancer diagnosis, including noninvasiveness, safety, and high cost-effectiveness.25 –30 However, technical factors associated with CT examination (excessive intestinal content and colon contraction), a round or oval shape and small tumor volume, pathological factors (colon mucinous adenocarcinoma and malignant adenoma transformations), and intussusception, may all lead to a missed diagnosis. 31 Michele et al. 6 compared the accuracies of colonoscopy and CT (for visible lesions) in localizing colonic lesions (single tumors) in a prospective multicenter study, and demonstrated no significant difference between the two preoperative tools (510/661 vs. 499/661 correctly localized lesions). The current analysis did not establish which method was more advantageous for diagnosing SCC when used alone, possibly due to the small sample size. Although both methods resulted in missed diagnoses, the combination of MSCT and colonoscopy could effectively reduce the missed diagnosis rate.
Most colonoscopy-associated missed diagnoses involved proximal cancers, possibly because of failure of the colonoscopy in terms of cecal intubation or obstruction due to poor bowel preparation and colonic stenosis. However, the whole colon can be observed by conventional MSCT.
Our data show that missed diagnoses by MSCT mainly resulted from technical factors (excessive intestinal content and colon contraction) and the round or oval shape and small volume of the tumors, which affect tumor visibility. Small colorectal tumors cannot be seen clearly on CT images, leading to missed diagnosis by MSCT. 31
Our analysis showed that MSCT-assisted diagnosis was unaffected by T stage and pathological type; however, this result may have been due to our small sample size. MSCT has previously shown good value for the diagnosis and T staging of digestive tract tumors. 32 In addition, T stage and pathological type do not result in misdiagnosis by colonoscopy, given that colonoscopy can observe all tumors as long as there are no factors affecting observation,17,18 such as colonic elongation, tortuosity, advanced diverticular disease, poor bowel preparation, colonic obstruction, or colonic stenosis.
SCC is a rare entity and this study was therefore limited by its small sample size. However, we will continue to collect data and expand the study. In addition, this was a single-center, retrospective study.
In conclusion, the current study showed that MSCT could improve the diagnostic accuracy of SCC when combined with colonoscopy. We recommend that abdominal CT be routinely performed in patients with SCC because colonoscopy may fail to observe the whole colon.