
Abstract
Percutaneous mechanical thrombectomy is a safe and effective treatment for addressing thrombosis in various embolic diseases. In recent years, this approach has also been actively applied in the management of acute embolic occlusion of the superior mesenteric artery. A pseudoaneurysm as a complication of this operation is remarkably rare. This is the first case report of the diagnosis and treatment of a pseudoaneurysm that developed as a complication after the application of percutaneous mechanical thrombectomy via an AngioJet device for thrombolysis in the superior mesenteric artery.
Keywords
Background
Acute superior mesenteric artery embolism (ASMAE) is a life-threatening condition that can lead to acute mesenteric ischemia. Without effective treatment, the consequences are devastating. Despite the improvements in living standards, the mortality rate of ASMAE remains fairly high, ranging from 60% to 90% during the past few decades.1–3 In recent years, percutaneous mechanical thrombectomy (PMT) has gradually become a very prevalent approach in the treatment of thrombosis. PMT effectively improves patients’ clinical symptoms and prognosis and reduces the incidence of exploratory laparotomy. Several reports have described the success of applying PMT for the treatment of ASMAE in the early stage.4,5 The development of a pseudoaneurysm as a complication of this operation is remarkably rare. We herein describe a man who was initially diagnosed with ASMAE and underwent PMT via an AngioJet device. After the operation, a pseudoaneurysm developed in the superior mesenteric artery. This is the first case report to describe the diagnosis and treatment of a pseudoaneurysm in superior mesenteric artery after the application of PMT.
Case report
A 37-year-old man presented to a general practitioner because of an 8-hour history of sudden-onset acute pain around the umbilicus. Ten days before the symptoms occurred, he had been diagnosed with infective endocarditis, and a blood culture revealed hemolytic streptococcus during hospitalization. A complete antibiotic treatment course was completed before the patient presented to our center (Hwa Mei Hospital, University of Chinese Academy of Sciences). After treatment, no bacterial growth was found in a late blood culture, and cardiac color ultrasound revealed no mitral valve or aortic valve vegetations. In addition, the patient had no other pertinent medical history, such as a connective tissue disorder. During this period, he developed no signs of peritoneal irritation or symptoms of intestinal necrosis, such as black stool. A blood panel showed a white blood cell count of 6.4 × 109/L. The patient maintained consciousness, and his blood pressure was within the normal range. Computed tomography (CT) angiography of the abdominal region showed superior mesenteric artery embolization.
Considering that the patient had no signs of intestinal necrosis, emergency surgery was performed in the digital subtraction angiography catheter room after the patient had provided written informed consent. During the operation, the right femoral artery was punctured, and a 6-Fr AngioJet thrombectomy catheter (Solent Omni, Boston Scientific, Marlborough, MA, USA) was used to achieve the thrombectomy. We operated the AngioJet catheter five times, and the total duration of the aspirations was 150 s. Subsequent imaging (Figure 1) showed that the blood flow of the distal main artery was significantly improved without obvious contrast agent extravasation. The patient’s symptoms improved after the thrombectomy, and no liver or kidney damage was detected after the surgery. However, 7 days after the endovascular procedure, the patient developed recurrent acute abdominal pain accompanied by abdominal muscle tension. CT angiography of the superior mesenteric artery indicated the presence of a pseudoaneurysm in middle part of the distal superior mesenteric artery (28 × 25 × 30 mm) with active extravasation (Figure 2). The patient was immediately scheduled for abdominal surgery under general anesthesia. During laparotomy, we found that the blood supply of the bowel was acceptable, no intestinal necrosis was found. The pseudoaneurysm was carefully resected, and some of the thrombus was further removed by a 3-Fr Fogarty catheter. No infected vegetation was detected during the whole process. Furthermore, we repaired the superior mesenteric artery, which contained two holes with rupture-induced hemorrhage (2 × 2 mm) (Figure 3). For this procedure, we did not use patches because of the small diameter of the superior mesenteric artery. After the operation, the blood flow normalized and the peritoneal cavity was surgically closed. Two weeks postoperatively, the patient recovered without complications and was discharged with a prescription of oral aspirin. The patient provided written consent for publication of this case report. We performed follow-up by telephone, and no symptoms or complaints were reported 1 month postoperatively.

(a) The superior mesenteric artery embolism (red arrow) in this patient is shown in the angiography image. (b) AngioJet thrombectomy catheter (Solent Omni; Boston Scientific, Marlborough, MA, USA) was applied for thrombolysis. After the operation, the blood flow was improved and no obvious contrast agent extravasation was observed.
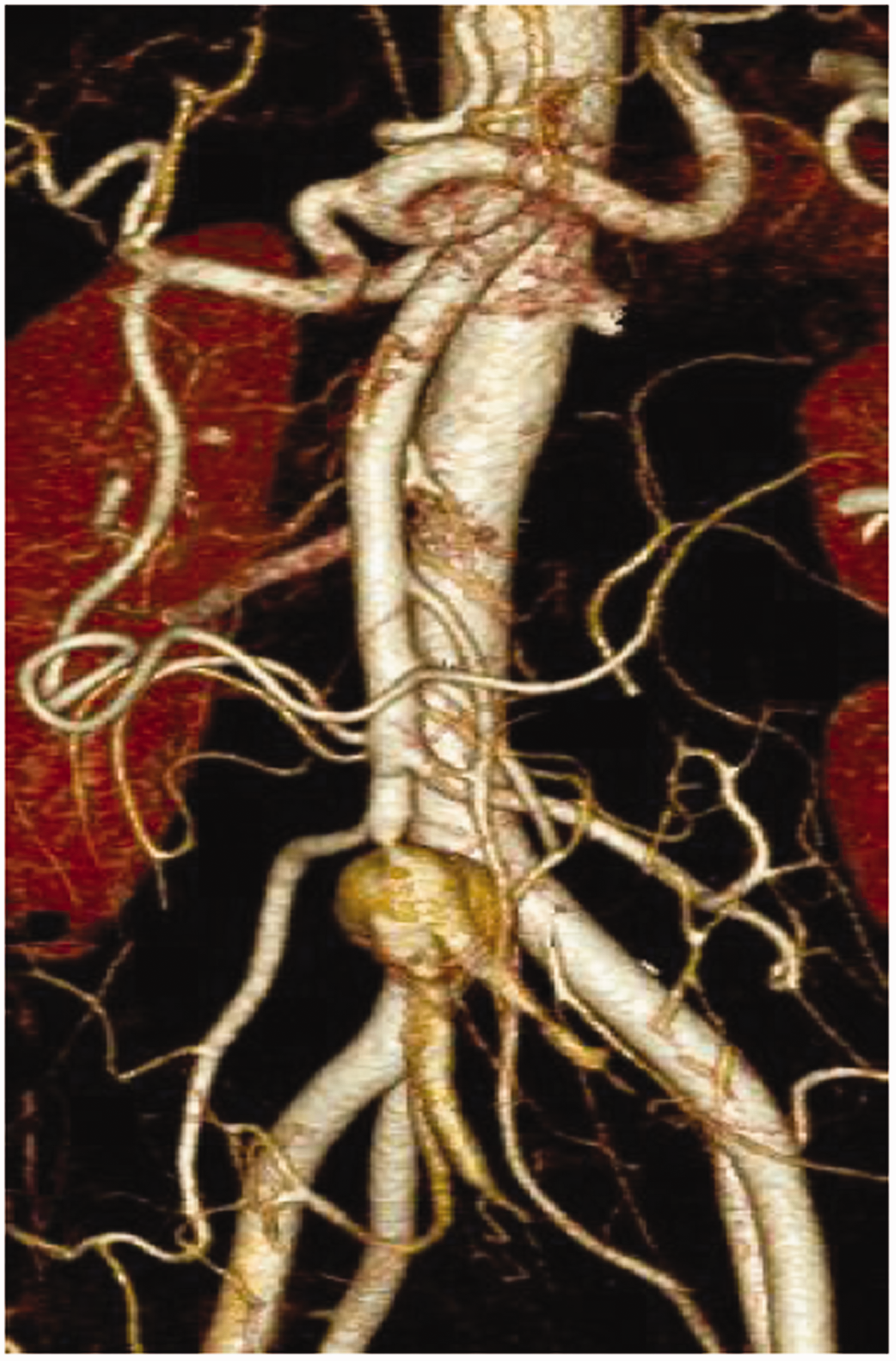
Computed tomography angiography of the superior mesenteric artery indicated the presence of a pseudoaneurysm in the middle distal region of the superior mesenteric artery (28 × 25 × 30 mm in size).

During abdominal open surgery, two arterial ruptures with bleeding (white arrows) were observed. The lesion sites were repaired by 7-0 polypropylene sutures (black arrows).
Discussion
In recent years, endovascular therapy (mechanical thrombectomy and thrombolysis) has been successfully used in the management of thrombi and emboli in various diseases diagnosed early in the clinical course. It has been widely used not only in the treatment of acute deep venous thrombosis but also in acute embolism of lower limb arteries.6,7 Thrombectomy devices such as the Rotarex debulking device (Straub Medical, Wangs, Switzerland) and AngioJet thrombectomy catheter (Solent Omni; Boston Scientific) are more commonly used for such treatments. Some scholars have attempted using these devices for superior mesenteric artery embolism and have achieved good results; however, these retrospective series were small.8,9
Although percutaneous thrombectomy devices have been widely applied in clinical practice in recent years, relatively little is known of critical points such as safety and competitive device performance. The AngioJet procedure is based on the Venturi effect: an electrolyte solution is introduced under high pressure into the catheter, and the thrombus is comminuted under continuous aspiration. A commonly reported complication after mechanical thrombectomy is transient kidney injury, which occurs as an incidence rate of approximately 22.8%. 10 No cases of pseudoaneurysms after thrombectomy have been reported. In the present case, this rare complication occurred after PMT. During the operation, the guide wire smoothly passed through the thrombus, and no untoward intraprocedural events occurred. We believe that vascular damage might be caused by high mechanical stress induced by the AngioJet on the vessel wall, leading to pseudoaneurysm formation. Some recent studies compared the percutaneous Rotarex and AngioJet thrombectomy devices in terms of their effectiveness and in vitro safety, 11 revealing that percutaneous thrombectomy devices have a risk of dissection and damage to the vascular layers based on the hematoxylin and eosin staining results of arterial specimens.
In the present case, we used PMT because, compared with catheter-directed thrombolysis, the AngioJet device can more effectively remove the embolus in a shorter amount of time. Additionally, the target vessel is not distorted, and the catheter of the AngioJet device can easily cross the embolic lesion. We used a nitinol hydrophilic guidewire (Radiofocus; Terumo, Tokyo, Japan) to cross the embolic lesion and smoothly arrive at the distal aspect of the superior mesenteric artery. No other untoward intraprocedural events occurred. This case also reminds us that careful attention should be paid when performing mechanical thrombectomy. It is important to stop the operation whenever necessary. The number of repeated aspirations is usually fewer than three when using the AngioJet thrombectomy catheter. In the present case, however, we performed five aspirations. Moreover, if the thrombectomy results are not sufficient or when the thromboembolus is difficult to remove, the operation may need to be stopped. To address this issue, bare stents can sometimes be effectively employed to reconstruct the blood supply. Additionally, violent operations should be avoided during the procedure. Before the patient in this case was transferred to our department, he was diagnosed with infective endocarditis and had completed an antibiotic course. Although no bacterial growth was found in the late blood culture, the vasculature itself may have been adversely affected by inflammatory factors and other systemic stimulations.
Although there was some debate on the second surgical intervention in the present case, we chose open surgery instead of endovascular treatment mainly for the following two reasons. First, the patient was a young man who was physically strong and could tolerate open surgery. Second, endovascular treatment would have been associated with a risk of infection when the covered stent and related embolization materials were implanted.
Conclusion
PMT by the AngioJet device is a treatment option for thrombosis of acute superior mesenteric artery embolism. However, we should pay extra attention to potential complications, especially the rare but severe complication of pseudoaneurysm formation.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
This case report is compliant with all relevant laws, institutional guidelines, and hospital standards. The ethics committee of Hwa Mei Hospital ruled that no formal ethics approval was required in this case study. Written informed consent was obtained prior to the preparation and submission of this manuscript (available upon request).
Funding
This work was supported by Ningbo Health Branding Subject (Grant No. PPXK2018-01).