
Abstract
Objective
To determine the levels of carcinoembryonic antigen (CEA), proliferating nuclear antigen Ki67 and p53 in pseudomyxoma peritonei (PMP) of appendiceal origin and to correlate the levels with clinicopathological characteristics and overall survival.
Methods
This retrospective study collected data on clinicopathological features and immunohistochemical staining of CEA, Ki67 and p53 in patients with PMP of appendiceal origin. Overall survival was evaluated using Kaplan–Meier plots. Median survival time was estimated by Log-rank tests. Potential prognostic factors were evaluated by Cox proportional hazards regression models.
Results
A total of 141 patients with PMP of appendiceal origin were enrolled in the study with a median age of 54 years. Of these, 93 (66.0%) were diagnosed with low-grade mucinous carcinoma, 43 (30.5%) with high-grade mucinous carcinoma and five (3.5%) with high-grade with signet ring cells. CEA exhibited ubiquitous immunopositivity in most cases and was not associated with overall survival. Ki67 labelling index (LI) and p53 status were related to histological grade and overall survival. The main pathological indicators affecting survival included histological grade, lymph node involvement, angiolymphatic invasion, Ki67 LI and p53.
Conclusion
Combined analysis of high Ki67 LI and aberrant p53 may provide the basis for evaluating the biological behaviour of PMP and predicting clinical outcome.
Introduction
Pseudomyxoma peritonei (PMP) is an extremely rare syndrome with an estimated incidence of 1–2 per million per year.1,2 PMP is characterized by extensive intraperitoneal mucinous effusions resulting from an accumulation of gelatinous ascites or disseminated lesions of neoplastic mucinous epithelia.1,2 Clinical manifestations include abdominal pain and abdominal distension. Imaging indicates non-specific space-occupying lesions in the abdomen and pelvis. 3 Abdominal puncture for the collection of mucinous ascites samples and laparotomy surgery in parallel with histopathology facilitate the diagnosis of PMP.4,5 Carcinoembryonic antigen (CEA) is one of the most widely used tumour serum markers, especially for diagnosing gastrointestinal tumours and for predicting tumour progression or remission. 6 Previous studies have indicated that proliferating nuclear antigen Ki67 and p53 status were closely related to development, differentiation, metastasis and prognosis of various malignancies.7–13 However, the significance of these factors in PMP has not been previously reported. This current study retrospectively reviewed PMP cases of appendiceal origin that had undergone cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC). The study collected clinicopathological data, evaluated the expression profiles of CEA, Ki67 and p53, and explored their relationship with the clinicopathological characteristics and prognosis.
Patients and methods
Patient recruitment
This retrospective study reviewed demographic and clinical characteristics from a chart review of all consecutive patients with PMP of appendiceal origin that were treated with CRS and HIPEC between February 2013 and March 2019 at the Department of Peritoneal Cancer Surgery, Beijing Shijitan Hospital, Capital Medical University, Beijing, China. Clinicopathological findings were reviewed including histological grade, lymph node involvement and perineural and angiolymphatic invasion. Pathological diagnosis was confirmed by haematoxylin and eosin staining of tissue sections. Expression of CEA, Ki67 and p53 was determined by immunohistochemistry on formalin fixed paraffin-embedded tissue samples as described below. All patients that met the diagnostic criteria were enrolled in the current study. PMP was classified into four categories according to Peritoneal Surface Oncology Group International standards. 1 Patients with PMP presenting as ‘acellular mucin’ were excluded from this study.
The study protocol was approved by the Medical Ethics Committee of Beijing Shijitan Hospital, Capital Medical University, Beijing, China (no. sjtkyll-lx-2020-51) and the study was conducted in accordance with the declaration of Helsinki. All patients or their authorized legal guardians provided written informed consent.
Immunohistochemical staining
Paraffin-embedded biopsy tissue blocks were cut into 4 µm sections, deparaffinized and rehydrated. The tissue sections were then incubated overnight at 4°C in a moist chamber. Immunohistochemical staining was performed using primary mouse monoclonal antibodies against Ki67 (clone UMAB107 ready to use; OriGene China, Beijing, China), p53 (clone DO7 ready to use; OriGene China) and CEA (clone COL1 ready to use; OriGene China) that were processed in automated staining equipment (INTELLIPATH FLX®; Biocare Medical, Pacheco, CA, USA). The negative control for each marker was mouse serum immunoglobulin G instead of primary antibody. Tonsil was used as positive control for Ki67, ovarian serous carcinoma was used as a positive control for p53 and colon cancer was used as a positive control for CEA according to the manufacturer’s instructions. All of the pathological sections were reviewed independently by two pathologists (F.Y. and F.S.) that were blinded to the clinical and follow-up status.
The results of the immunohistochemical staining were interpreted as follows: (i) positive CEA staining was defined as brown granular staining in the membrane and cytoplasm; (ii) positive Ki67 staining was defined as brown granular staining in the nucleus. Ki67 labelling index (LI) was calculated as ‘number of positive cells/total count cells ×100’ and it was divided into low (<50%) or high (≥50%); (iii) P53 expression status was scored into three groups: normal, negative and excessive immunostaining. ‘Normal’ referred to a weak focal nuclear staining (resembling that in normal epithelium) in <50% of tumour nuclei. ‘Negative’ indicated a complete lack of nuclear staining (even though the nuclei of normal epithelial and stromal cells showed a normal pattern). ‘Excessive’ was defined when strong nuclear staining was present in the majority of tumour cells (≥50%). Both negative and excessive staining were considered as an aberrant p53 pattern.14,15
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). Categorical data were compared using χ2-test or Fisher's exact test. The overall survival was calculated from the date of confirmed diagnosis to the date of last follow-up or death. Median survival time was estimated by Kaplan–Meier plots and Log-rank tests. Item-level model comparison was proposed for the Wald test based on the observed information matrix. Potential prognostic factors were evaluated by Cox proportional hazards regression models. A P-value of <0.05 was considered statistically significant.
Results
This retrospective study enrolled 141 patients with PMP of appendiceal origin (69 males [48.9%]; 72 females [51.1%]) with a median age of 54 years (range, 25–79 years). The follow-up duration ranged between 2 and 217 months. Of the 141 patients with PMP, 93 (66.0%) were diagnosed with low-grade mucinous carcinoma (LGMC), 43 (30.5%) with high-grade mucinous carcinoma (HGMC) and five (3.5%) with high-grade with signet ring cells (HGMC-S). The clinical manifestations of PMP were generally non-specific, such as abdominal discomfort, abdominal pain, distension, loss of appetite, nutritional compromise, weight loss and intestinal obstruction. Imaging indicated non-specific space-occupying lesions in the abdomen and pelvis, peritoneal effusion, as well as thickening and omental caking. Imaging examinations, including computed tomography, were used to predict and monitor recurrence and progression. Liquid density shadows and slightly more heterogeneous appearance were widely distributed in the abdominal cavity, surrounding the liver and stomach, and located in the intestinal space (Figure 1a).

Representative clinical features of pseudomyxoma peritonei: (a) imaging indicated non-specific space-occupying lesions in the abdomen and pelvis, with peritoneal effusion; (b) multiple colloidal mucinous nodules; (c) destructive invasion of the intestinal canal, such as the spleen, from the serosa. The colour version of this figure is available at: http://imr.sagepub.com.
The intraperitoneal tumours consisted of multiple colloidal mucinous nodules (Figure 1b) or jelly-like mucous masses. Tumours often invaded the peritoneum and the surface of the abdominal viscera. Some tumours destroyed the pelvic and abdominal organs, such as the spleen (Figure 1c). Microscopically, mucous epithelial components were floating in the mucus lake and epithelial atypia could be identified to different extents between patients. LGMC presented as irregular mucous glandular structures, floating clusters or flat strips of neoplastic mucinous epithelium with lightly enlarged hyperchromatic nuclei and nuclear stratification (Figure 2a). HGMC presented as cribriform structures and enlarged, vesicular nuclei with full-thickness stratification, disappearance of nuclear polarity, prominent nucleoli and increased mitosis (Figure 2b) or destructive stromal invasion. HGMC with typical signet ring cells were defined as HGMC-S (Figure 2c).

Representative histopathological features of pseudomyxoma peritonei: histological morphology of low-grade mucinous carcinoma (LGMC) (a), high-grade mucinous carcinoma (HGMC) (b) and high-grade with signet ring cells (HGMC-S) (c) (all haematoxylin and eosin; scale bar 50 µm); strong positive staining for carcinoembryonic antigen in LGMC (d), HGMC (e) and HGMC-S (f); weak focal nuclear staining of p53 in LGMC (g); complete lack of stained tumour nuclei for p53 in HGMC (h); strong positive staining for p53 in HGMC-S (i); low Ki67 LI in LGMC (j); high Ki67 LI in HGMC (k) and HGMC-S (l) (d–l, EnVision staining; scale bar 50 µm). The colour version of this figure is available at: http://imr.sagepub.com.
The CEA immunostaining exhibited ubiquitous immunopositivity (135 of 141 patients [95.7%]) in the membrane and cytoplasm of PMP tumour cells and there was no differential expression with increased histological grades. CEA immunoreactivity was also found in the mucus in some cases (Figures 2d–2f). Scattered expression of normal p53 with differential intensity of staining was observed more frequently in LGMC (Figure 2g). Aberrantly expressed p53 was more likely to have diffusely, consistently strong positive staining in HGMC and HGMC-S (Figure 2h and 2i). Ki67 was minimally expressed in LGMC, but highly expressed in HGMC and HGMC-S (Figures 2j–2l).
The median survival time of the cohort of 141 PMP patients was 72.8 months. A total of 34 patients died: 11 with LGMC, 20 with HGMC and three with HGMC-S. The median overall survival was longer in women than in men (not reached versus 59.7 months, respectively; P = 0.01) and in LGMC than in HGMC or HGMC-S (86.0 versus 45.7 or 11.4 months, respectively; P < 0.001). Patients with lymph node involvement or angiolymphatic invasion had reduced overall survival than those without these risk factors (20.0 versus 83.0 months, respectively, P < 0.001; 40.0 versus 83.0 months, respectively, P < 0.001). Univariate analysis identified pathological indicators affecting overall survival: histological grade (P < 0.001; Figure 3a), Ki67 (P < 0.001; Figure 3b), p53 (P = 0.001; Figure 3c), lymph node involvement (P < 0.001) and angiolymphatic invasion (P < 0.001) (Table 1). CEA expression and perineural invasion had no significant effect on overall survival.

Kaplan–Meier survival curves of patients with pseudomyxoma peritonei stratified according to the following: (a) histological grade; (b) Ki67 immunostaining; (c) p53 status; (d) Ki67 and p53 subgroups. The colour version of this figure is available at: http://imr.sagepub.com.
Univariate analysis of overall survival of patients (n = 141) with pseudomyxoma peritonei.

LGMC, low-grade mucinous carcinoma; HGMC, high-grade mucinous carcinoma; HGMC-S, high-grade with signet ring cells; CEA, carcinoembryonic antigen; LI, labelling index; NS, no significant association (P ≥ 0.05).
The CEA immunoreactivity was not related to histological grade (data not shown). The Ki67 LI was high in HGMC and HGMC-S but low in LGMC (P < 0.001) (Table 2). Aberrant staining of p53 was detected more frequently in HGMC and HGMC-S than in LGMC (P < 0.001). The p53 status was significantly associated with histological grade (P < 0.001), Ki67 LI (P = 0.001), lymph node involvement (P = 0.004) and angiolymphatic invasion (P = 0.001). The Ki67 LI was significantly associated with histological grade (P < 0.001), p53 (P < 0.001) and perineural invasion (P = 0.018).
The difference in clinicopathological characteristics between patients (n = 141) with pseudomyxoma peritonei stratified according to Ki67 and p53 immunostaining levels.
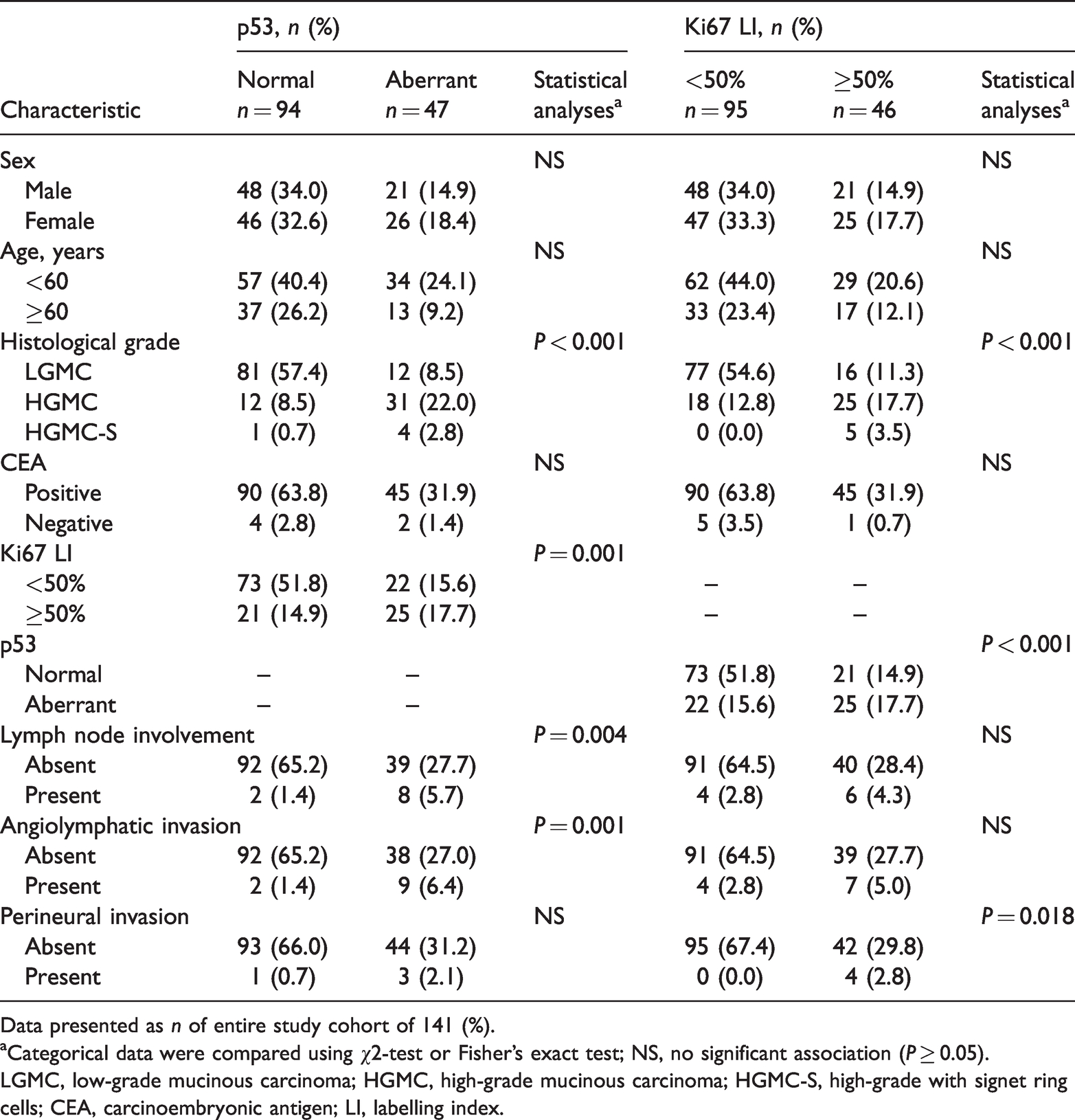
Data presented as n of entire study cohort of 141 (%).
aCategorical data were compared using χ2-test or Fisher's exact test; NS, no significant association (P ≥ 0.05).
LGMC, low-grade mucinous carcinoma; HGMC, high-grade mucinous carcinoma; HGMC-S, high-grade with signet ring cells; CEA, carcinoembryonic antigen; LI, labelling index.
The histological grade was the only prognostic factor for overall survival of patients with PMP as determined by multivariate analysis (Table 3).
Multivariate analysis of overall survival of patients (n = 141) with pseudomyxoma peritonei.
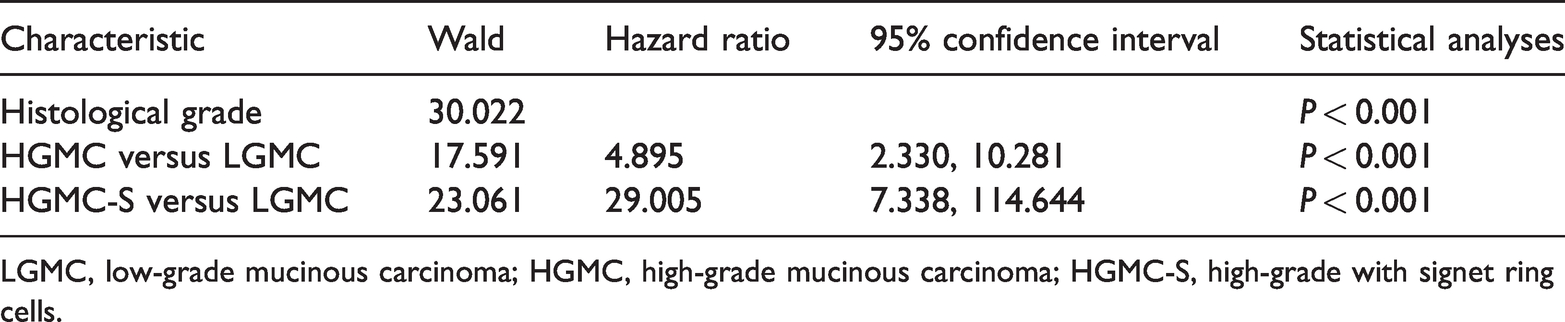
LGMC, low-grade mucinous carcinoma; HGMC, high-grade mucinous carcinoma; HGMC-S, high-grade with signet ring cells.
The patients were divided into four groups based on the Ki67 LI and p53 status: low Ki67 and normal p53; low Ki67 and aberrant p53; high Ki67 and normal p53; high Ki67 and aberrant p53. The patients with low Ki67 and normal p53 had a better prognosis compared with the other three subgroups (P ≤ 0.001 for all comparisons; Figure 3d, Table 4).
Multivariate analysis of the association between Ki67/p53 status and the overall survival of patients (n = 141) with pseudomyxoma peritonei.

Discussion
The serum marker CEA is commonly used in gastrointestinal tumours as it is valuable for monitoring tumour progression or remission. 6 However, serum CEA might not be an ideal marker of the aggressiveness and progression of PMP tumours. 16 Immunohistochemical staining of CEA may help to distinguish a benign tumour from a malignant tumour and it might be involved in predicting prognosis.17,18 In general, Ki67 is associated with the prognosis of multiple tumours by reflecting the level of tumour cell proliferation, but Ki67 alone might not predict the aggressiveness and progression as demonstrated by previous studies in breast and other cancers.19,20 P53 is an important tumour suppressor gene and it plays multifaceted roles in the development and progression of malignancies. 21 Usually, wild-type p53 is maintained at a low level, while in response to cellular stress, p53 is activated through multiple mechanisms. 22 Activated wild-type p53 inhibits tumorigenesis, whereas mutant p53 loses its suppressive functions. 22 Strong and diffuse expression of p53 is generally interpreted as an immunohistochemical marker for TP53 gene mutations. 23 The result of immunohistochemical staining of p53 protein was consistent with gene mutations. 23 High Ki67 LI and aberrant p53 have synergistic effects on tumorigenesis in other tumours such as breast cancer and gastroenteropancreatic neuroendocrine carcinoma.24,25 The expression patterns of CEA, Ki67 and p53 have not been previously reported in PMP specimens of appendiceal origin.
In this current study, CEA exhibited ubiquitous immunopositivity in the membrane and cytoplasm of epithelium cells of different histological grades. In some cases, CEA displayed immunoreactivity in the mucinous island, implying that this glycoprotein was probably shed from the surface of the PMP tumour cells into the mucinous ascites. However, the expression of CEA was not related to overall survival. Histological grade is an independent prognostic parameter for overall survival. 26 Aberrant p53 or high Ki67 LI correlated with high histological grade in the current study. Patients with a lower level of Ki67 and normal p53 had better prognosis that those patients in the other three subgroups in the current study. High histological grade, high expression of Ki67 and aberrant p53 conferred worse overall survival of patients with PMP in the current study. These current findings were consistent with a previous report. 15 Based on the current analysis, it was clear that some patients with aberrant p53 have low Ki67 and vice versa, so looking at just one of the markers would not be adequate. Combined analysis of high Ki67 LI and aberrant p53 may provide the basis for evaluating the biological behaviour of PMP and predicting clinical outcome.
In addition, considering the results of the immunohistochemical staining of Ki67 and p53 might contribute to a more precise histological classification of PMP, a comprehensive understanding of tumorigenesis and biological behaviour and a personalized treatment plan. Previous studies have shown that the mutation rate of the KRAS and GNAS genes were 58–100% and 40–77% in patients with PMP, respectively.27–31 In addition, the P53, SMAD4 and PIK3CA genes had mutations consistent with the polygenic effects of tumorigenesis. 32 Although a number of studies have looked at genetic mutations and molecular markers,27–31 the mechanisms of PMP development remain unclear. PMP has traditionally been considered as a benign tumour, with a wide spectrum of progression, from slow-growing, moderate lesions to rapidly progressive infiltrative disease. 33 After treatment with CRS and HIPEC, PMP tumours remain prone to recurrence and progression, extensively invading and infiltrating the adjacent tissues/organs.34,35
In conclusion, the biological characteristics of PMP need to be further investigated, so that recurrence may be prevented or delayed after operation and overall survival might be improved without increasing the incidence of postoperative complications. The histological grade in addition to the combined detection of p53 and Ki67 may provide the basis for the assessment of development, progression and prognosis of PMP in the future.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211022297 - Supplemental material for Prognostic significance of CEA, Ki67 and p53 in pseudomyxoma peritonei of appendiceal origin
Supplemental material, sj-pdf-1-imr-10.1177_03000605211022297 for Prognostic significance of CEA, Ki67 and p53 in pseudomyxoma peritonei of appendiceal origin by Fengcai Yan, Feng Shi, Xinbao Li, Hong Chang, Mulan Jin and Yan Li in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Beijing Municipal Natural Science Foundation, China (no. 7172108), the Youth Research Fund of Beijing Shijitan Hospital (no. 2019-q11), the Beijing Municipal Administration of Hospitals’ Ascent Plan (no. DFL20180701), the Special Fund for the Capital Characteristic Clinical Medicine Development Project (no. Z161100000516077) and the Beijing Municipal Grant for Medical Talents Group on Peritoneal Surface Oncology (no. 2017400003235J007).