
Abstract
Diffuse large B-cell lymphoma (DLBCL) commonly presents with systemic manifestations including fever, weight loss, and night sweats. Uncommonly, patients with DLBCL can present with musculoskeletal manifestations mimicking polymyalgia rheumatica (PMR). Herein, the case of a 61-year-old woman who presented with pain in the bilateral shoulders, arms, hands, knees, pelvic girdle, and neck with bouts of fever, is presented. Laboratory workup for infectious and connective tissue diseases was non-revealing, except for elevated inflammatory markers. A positron emission tomography (PET)/computed tomography (CT) scan was suggestive of PMR, but also revealed enlarged lymph nodes initially thought to be reactive in nature. However, a lymph node biopsy showed findings consistent with DLBCL. This case highlights the importance of a thorough investigational workup when cases with features of PMR do not meet the proper criteria for this diagnosis to be made, in order not to miss a hematopoietic neoplasm with a PMR-like presentation.
Keywords
Introduction
Polymyalgia rheumatica (PMR) is a common idiopathic systemic inflammatory disease that affects patients older than 50 years, and particularly women of Northern European ancestry. 1 Since PMR is clinically characterized by aching pains in the proximal muscle groups with morning stiffness, 2 this diagnosis cannot be rendered with certainty without excluding other entities with overlapping clinical features, such as polymyositis, elderly onset seronegative rheumatoid arthritis, late onset systemic lupus erythematosus, tuberculosis, hypothyroidism, and malignancies. 3 In rare cases, certain non-Hodgkin lymphomas can present with features mimicking PMR. Herein, the case of a 61-year-old woman who presented with pain in the bilateral shoulders, arms, hands, knees, pelvic girdle, and neck with minimal morning stiffness along with nocturnal bouts of fever, is reported. Initially thought to have PMR, she was found to have diffuse large B-cell lymphoma after thorough investigation.
Case report
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. As this is a case report, ethical permission was not required.
A 61-year-old female with previous medical history of diabetes mellitus type 2 presented to the Rheumatology clinic of the American University of Beirut Medical Center, in September 2020, with a 2-week history of pain in the bilateral shoulders, arms, hands, knees, pelvic girdle, and neck. The patient had also been experiencing minimal morning stiffness, and reported nocturnal bouts of fever. On physical exam, the patient had tenderness of both wrists with mild swelling and no weakness. Review of systems was otherwise negative.
Laboratory workup included blood studies that showed elevated C-reactive protein (131.5 mg/l), erythrocyte sedimentation rate (27 mm/h), and ferritin (794 ng/ml). All connective tissue and infectious disease studies in the current case were non-revealing (Table 1). The patient was started on 100 mg aceclofenac, orally, three times daily for 1 week, followed by a course of 15 mg prednisolone, orally, once daily for 1 week, with no improvement in symptoms. As part of excluding any malignant or inflammatory process, a chest X-ray was performed and showed normal findings. In addition, a computed tomography (CT) scan of the abdomen and pelvis showed findings within normal limits. To exclude a vasculitis process, the patient underwent a whole-body positron emission tomography (PET)/CT scan with fluorine-18-fluorodeoxyglucose (18F-FDG) that revealed bilateral and symmetrical increased 18F-FDG uptake in the large joints of the upper and lower extremities, suggestive of an inflammatory process such as PMR or rheumatoid arthritis (Figures 1a–e). Additionally, supra- and infradiaphragmatic 18F-FDG-avid lymph nodes were noted, as well as increased activity in the spleen and bone marrow (Figure 1a and Figure 2). These findings were initially thought to be most likely related to polyarthropathy and less likely related to a lymphoproliferative disease. For further evaluation, an ultrasound-guided right cervical lymph node biopsy was performed.
Summary of the present and previously reported cases of diffuse large B-cell lymphoma mimicking polymyalgia rheumatica.
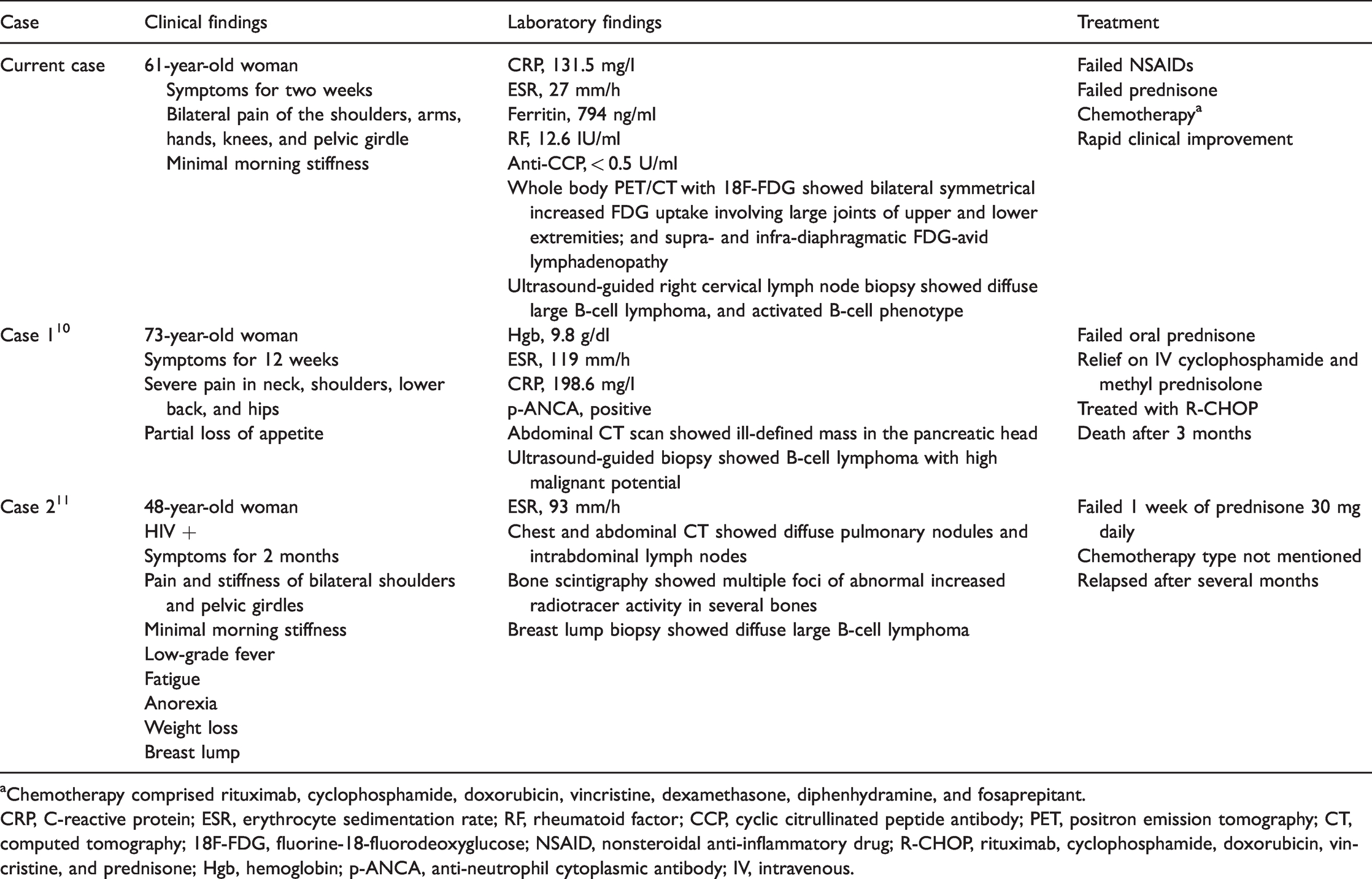
aChemotherapy comprised rituximab, cyclophosphamide, doxorubicin, vincristine, dexamethasone, diphenhydramine, and fosaprepitant.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; RF, rheumatoid factor; CCP, cyclic citrullinated peptide antibody; PET, positron emission tomography; CT, computed tomography; 18F-FDG, fluorine-18-fluorodeoxyglucose; NSAID, nonsteroidal anti-inflammatory drug; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; Hgb, hemoglobin; p-ANCA, anti-neutrophil cytoplasmic antibody; IV, intravenous.

Representative images from fluorine-18-fluorodeoxyglucose positron emission tomography (18F-FDG PET)/computed tomography (CT) scans: (a) maximum intensity projection image of a whole-body 18F-FDG PET/CT showing bilateral symmetrical mild-to-moderately increased FDG uptake in the large joints of the upper and lower extremities as well as moderate-to-intensely FDG-avid supra- and infra-diaphragmatic lymphadenopathy, namely in the submandibular, right jugulocarotid, right supraclavicular, right paratracheal, aortopulmonary, subcarinal, common iliac and left external iliac regions. The spleen is mildly prominent measuring 14 cm craniocaudally with diffuse mildly increased FDG uptake, equal to that of the liver. There is also diffuse mildly increased FDG uptake throughout the bone marrow; and axial 18F-FDG PET/CT images through (b) the shoulders, (c) the elbows, (d) the hips, and (e) the knee joints, showing bilateral symmetrical, mild-to-moderately increased FDG uptake along the joints, probably along the synovial lining, with maximum standardized uptake value ranging from 3.9 in the left elbow joint to 7.7 in the right knee joint, associated with a small amount of effusion, mainly in the elbow and knee joints (white arrows).
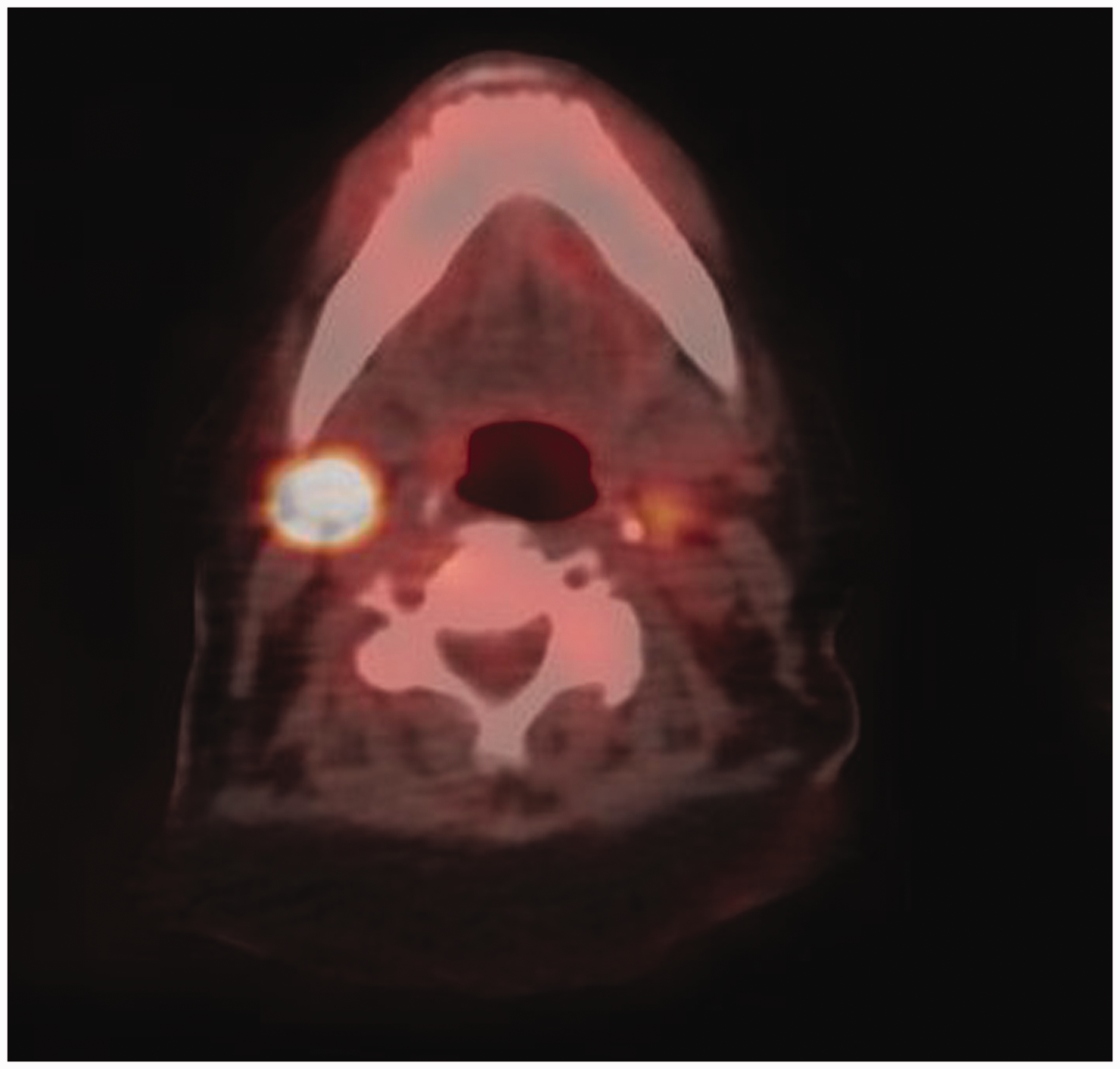
Axial fused fluorine-18-fluorodeoxyglucose positron emission tomography (18F-FDG PET)/computed tomography (CT) image of the neck showing an intensely FDG-avid enlarged right submandibular lymph node with maximum standardized uptake value of 17.2.
The lymph node biopsy showed a diffuse population of large atypical lymphocytes with irregular nuclei, prominent nucleoli, and increased mitotic activity (Figure 3), and with a Ki-67 proliferation index of approximately 80%. Immunohistochemistry was performed with appropriate controls and showed that the atypical cells were positive for CD20 antigen, apoptosis regulator BCL-2, B-cell lymphoma 6 protein, multiple myeloma oncogene 1, and negative for cluster of differentiation 3, membrane metalloendopeptidase (CD10), lymphocyte activation antigen CD30, cytokeratin AE1/AE3, and Epstein-Barr virus-encoded RNA (analysed by in situ hybridization). These findings were consistent with a diffuse large B-cell lymphoma, activated B-cell phenotype (per the Hans algorithm). 4 Brain magnetic resonance imaging was negative for any metastatic disease. A bone marrow biopsy showed no evidence of involvement by lymphoma. Subsequently, the patient was started on chemotherapy comprising 700 mg rituximab, 1400 mg cyclophosphamide, 90 mg doxorubicin, 2 mg vincristine, 12 mg dexamethasone, 25 mg diphenhydramine, and 150 mg fosaprepitant, intravenously, every 3 weeks for a total of six cycles, each cycle every 3 weeks and high-dose methotrexate (15 mg, intravenously, every 3 weeks for a total of six cycles). She showed moderate improvement of her symptoms after the second cycle of chemotherapy. A whole-body PET/CT scan with 18F-FDG, performed after 3 months of initial presentation and six cycles of treatment, showed findings of disease remission with decreased bilateral symmetric 18F-FDG uptake involving the large joints of the upper and lower extremities. Clinically, the patient reported feeling better, and showed no signs of peripheral arthritis.
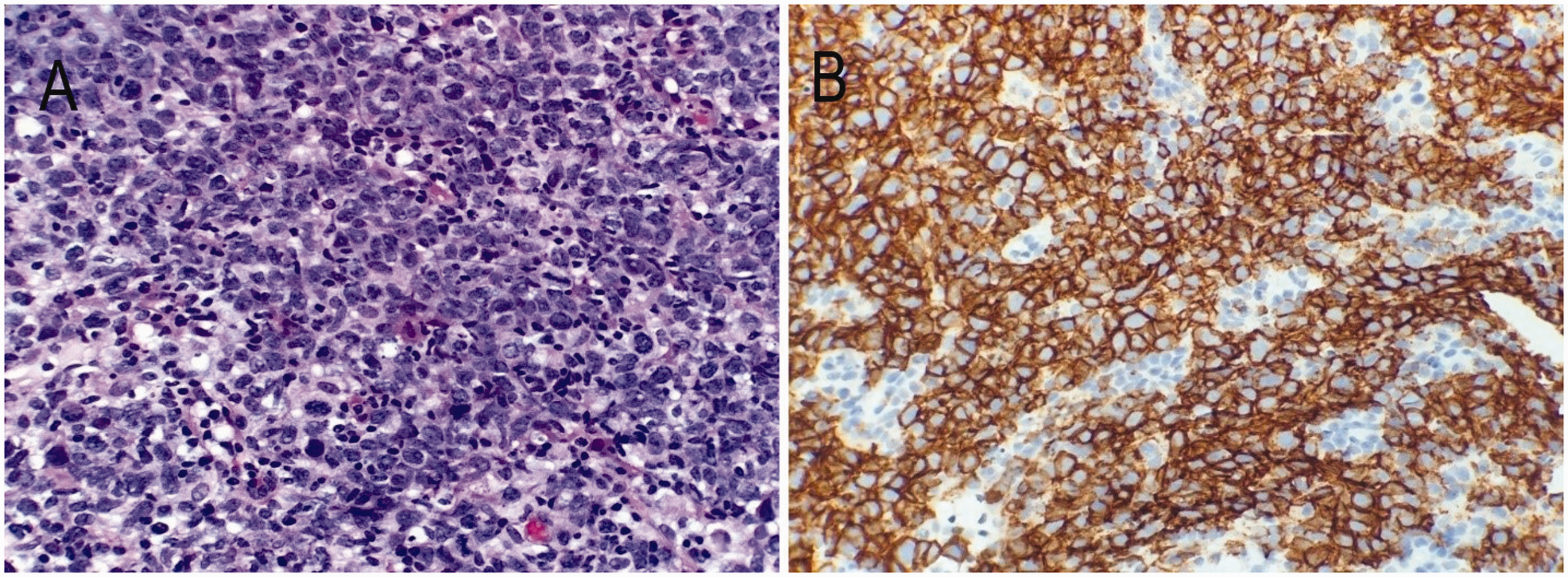
Representative photomicrographs from immunohistopathology analyses of lymph node biopsy tissue sections, showing: (a) diffuse population of large atypical cells with irregular nuclei, prominent nucleoli, and increased mitotic activity (hematoxylin and eosin stain, original magnification, × 400); and (b) strong and diffuse immunostaining of CD20 antigen in the atypical infiltrate (original magnification, × 400).
Discussion
Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin lymphoma. 5 About one-third of patients present with B symptoms, such as fever, weight loss, and night sweats, 6 however, other symptoms may occur and are related to extra-nodal sites of involvement, most commonly the gastrointestinal system. 6
The relationship between non-Hodgkin lymphoma, including DLBCL, and PMR is multifaceted. Patients with PMR are shown to have around a 1.4 times increased risk of non-Hodgkin lymphoma compared with the general population. 7 Additionally, a spectrum of diseases including hematological and solid malignancies can mimic PMR. 8 Of note, musculoskeletal involvement has been reported in about 7–25% of patients with non-Hodgkin lymphoma during the course of their disease, 9 however, there have been few reports that have specifically described cases of DLBCL mimicking PMR (summarized in Table 1).10,11
In the case presented herein, the reason for increased 18F-FDG uptake by the large joints is unclear, but might be related to lymphoma-associated polymyalgia symptoms that occur as a paraneoplastic syndrome. 12 Certain cellular risk factors, such as intercellular adhesion molecule 1 expression and the nuclear factor-κB1 promotor insertion/deletion polymorphism, -94ins/delATTG, may lead to the proliferation of mature B-cells that secrete multiple cytokines, which might contribute to the PMR-like presentation.13–16 Interestingly, some of these cytokines can act as independent prognostic markers for DLBCL. 15 Notably, a concomitant inflammatory disorder might still have been present contributing to the patient’s symptoms.
The 18F-FDG PET/CT is a very useful tool for evaluation of DLBCL versus an active PMR. 17 Periarticular accumulation is the most common pattern of 18F-FDG uptake in patients with PMR, 18 while a high intensity uptake of 18F-FDG (i.e. standardized uptake value) in the lymph nodes is suggestive of a lymphoproliferative disorder. 19 Since lymphadenopathy is an atypical feature of PMR, 20 a lymph node biopsy is recommended in any patient presenting with PMR-like symptoms and 18F-FDG-avid lymph nodes, to avoid missing a hematopoietic neoplasm.
Conclusion
The present case highlights the importance of a thorough investigation in patients presenting with PMR-like symptoms. Additionally, it emphasizes the need for a tissue biopsy from 18F-FDG-avid lymph nodes in such patients, to rule out hematopoietic neoplasms with PMR-like paraneoplastic manifestations, as observed in the reported case presentation.
Footnotes
Acknowledgements
The authors acknowledge the help of all colleagues at the American University of Beirut Medical Center.
Author contributions
IU and AB conceived and supervised the study; SN and AAG analysed data; GEH wrote the manuscript; AT and IU revised the manuscript; and all authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.