
Abstract
Objectives
External valvuloplasty (eVP) is a reconstructive surgical method to repair the function of the terminal and preterminal valves. We evaluated the 6-month outcomes of eVP regarding the diameter of the great saphenous vein (GSV).
Methods
Patients from five vein centres were included in this observational study. Follow-up involved detailed duplex sonography of the GSV. The venous clinical severity score (VCSS) and the C class of the clinical, aetiologic, anatomic and pathophysiologic (CEAP) classification were recorded.
Results
We enrolled 210 patients, with a follow-up rate of 58%; eVP was sufficient in 95.24% of the patients. The GSV diameters decreased significantly from 4.4 mm (standard deviation (SD): 1.39) to 3.9 (SD: 1.12), 4 cm distal to the saphenofemoral junction (SFJ); from 3.7 mm (SD: 1.10) to 3.5 mm (SD: 1.02) at the mid-thigh; from 3.6 mm (SD: 1.14) to 3.3 mm (SD: 0.94) at the knee and from 3.1 mm (SD: 0.99) to 2.9 mm (SD: 0.78) at the mid-calf. VCSS decreased significantly from 4.76 (SD: 2.13) preoperatively to 1.77 (SD: 1.57) 6 months postoperatively.
Conclusions
GSV function can be restored by eVP; diameters over the total length of the GSV decreased significantly.
Keywords
Introduction
Chronic venous disease is a frequent problem with high socioeconomic impact in Western countries. 1 Varicose veins mainly develop because of reflux in superficial or deep veins, 2 although reflux is limited to the superficial system in one-third of the patients. 3 Concerning the superficial venous system, reflux mostly occurs in the great saphenous vein and increases with age. 4 Furthermore, reflux is associated with the vein’s diameter.5,6 The great saphenous vein diameters at the saphenofemoral junction and the thigh could be relevant, as they can correlate with the venous clinical severity score (VCSS). 7 In this context, a value of 5 mm in the lower thigh is a reported cut-off. 5 Moreover, there is an association between a great saphenous vein diameter of 5 mm and a competent terminal valve. 8 Generally, there is a positive correlation between truncal diameters and higher clinical (“C”) classes of the clinical, aetiologic, anatomic and pathophysiologic (CEAP) classification6,9 and the presence of venous symptoms. 6 Therefore, eliminating reflux is the principle of all treatment strategies. Currently, surgical and endovenous methods are widely used. 10 The great saphenous vein is removed during high ligation and stripping, whereas the vein is destroyed or occluded during endovenous thermal or non-thermal procedures. 10 Only a few vein-sparing procedures attempt to restore the vein's function, which is generally a high-level goal in many surgical treatments. As treatment methods, ambulatory selective varices ablation under local anaesthesia (ASVAL), Cure Conservatrice et Hémodynamique de l'Insuffisance Veineuse en Ambulatoire strategy (CHIVA), and external valvuloplasty (eVP) have been described.11–13 eVP is a reconstructive surgical method aimed at repairing the function of the terminal and preterminal valve. 14 In our department, we achieve this by implanting a u-shaped patch at the saphenofemoral junction, 15 although other devices can be used.12,16,17 This patch covers the great saphenous vein to reduce the vein’s diameter, which permits the valve leaflets to open and close sufficiently again. 14 However, this procedure is limited to approximately 15% of all varicose veins patients. 15 Although excellent long-term results with a recurrence rate of 4.6% after 68.5 months and improved venous hemodynamics have been described after eVP,17–19 there is a lack of data because most studies are single-centre. 20 Therefore, we performed this prospective multicentre study involving five high-volume vein centres in Germany. The short-term (6 weeks) results of the safety and functionality of eVP were published recently. 14 The aim of the current study was to elucidate the outcomes 6 months after eVP, with specific evaluation of the great saphenous vein diameters at several anatomical levels.
Material and methods
eVP
eVP was performed as previously described14,21 according to a standardised protocol and under a preoperative single dose of antibiotic. Specifically, the great saphenous vein was exposed via a standard inguinal approach, and all side branches were ligated. After identifying the saphenofemoral junction and the common femoral vein, we modified a preformed 4- × 2-cm non-absorbable polyurethane patch with a u-shaped gap (VenoPatch®; B. Braun Melsungen AG, Melsungen, Germany) around the great saphenous vein (Figure 1). The patch was fixed like a cuff with 4 to 5 sutures to reduce the diameter of the vein to ≤ 5 mm to repair the terminal and preterminal valves. The restored valve’s function after eVP was controlled intraoperatively by an indicator vein, as previously described.14,15 Afterwards, the two flaps of the patch were fixed on the common femoral vein by two additional sutures. Finally, multiple phlebectomies of side branches were performed. We added elastic compression bandages for 1 day postoperatively and recommended the use of compression hosiery with an ankle pressure of 18 to 23 mmHg (German class 2) for 6 weeks.
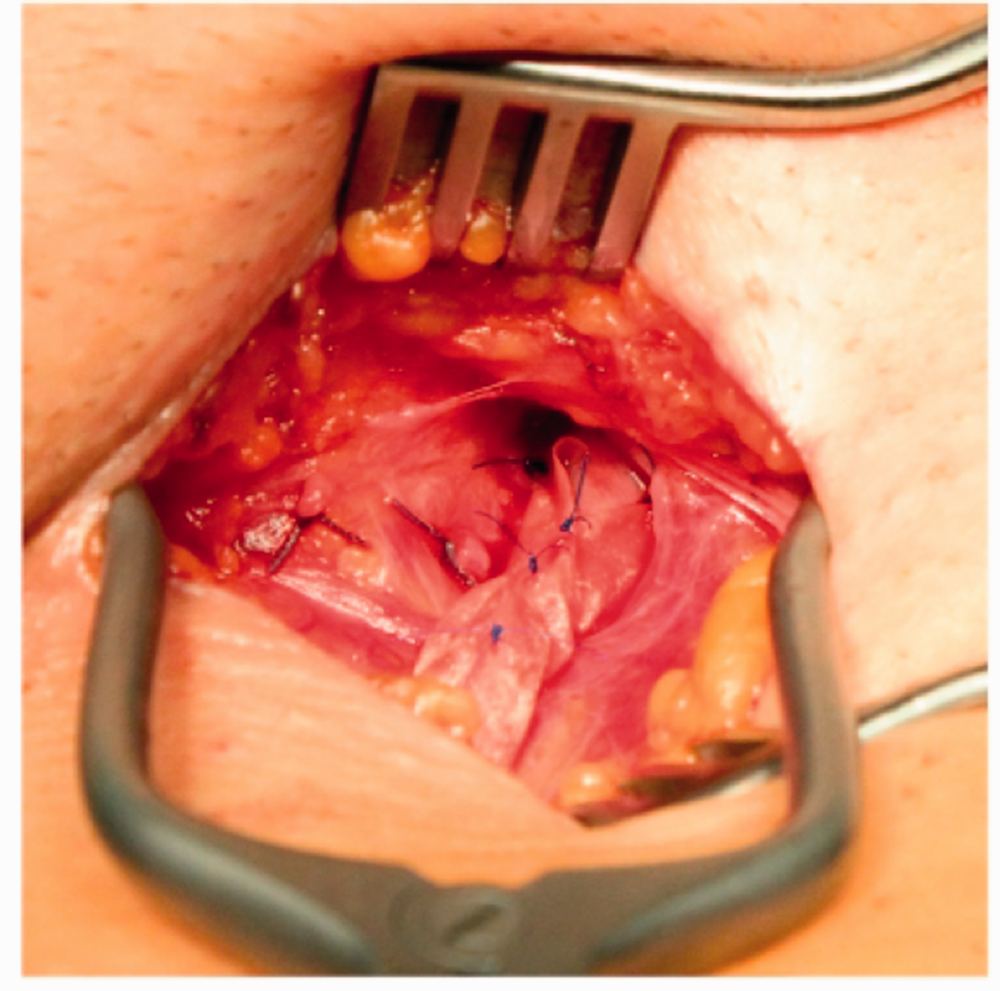
Scheme of external valvuloplasty.
Reflux of more than 0.5 s was considered pathological. 22 Patients with a great saphenous vein diameter at the level of the terminal valve between 5 and 12 mm and duplex-sonographically visible, mobile valvular leaflets of the terminal and preterminal valves were eligible for eVP.
Follow up
Follow-up examination involved detecting reflux in the great saphenous vein, especially at the saphenofemoral junction, to assess the functional results of eVP. eVP was considered sufficient if there was no reflux or occlusion of the GSV at the saphenofemoral junction. Additionally, the great saphenous diameters were measured at the following previously defined points: 4 cm distal to the saphenofemoral junction, at the mid-thigh, at the knee and at the mid-calf. Reflux was measured according to Hach stage (Hach I: reflux at the saphenofemoral junction and insufficiency of the anterior accessory great saphenous vein; Hach II: reflux to the knee; Hach III: reflux to the calf and Hach IV: reflux in the entire vein, from the saphenofemoral junction to the ankle. 23 The VCSS and the C class of the CEAP classification were also recorded.24,25
Ethics
The study was approved by the Ethics Committee (Registry Number 5024 -14 in 2014) of the medical faculty of the Ruhr University of Bochum. Patients provided written informed consent.
Statistical analysis
Statistical analyses were performed using PSPP (GNU PSPP Statistical Analysis Software, Release 1.2.0-g07fb-4db; Free Software Foundation, Boston, MA, USA) and Microsoft Excel (Microsoft, Redmond, WA, USA) (paired Student's t-test, χ2 test). We performed an intention-to-treat analysis, and p<0.05 was considered significant.
Results
Patients
Initially, we included 359 symptomatic patients with great saphenous vein reflux in this observational study between 2015 and 2019; 210 patients were available for the 6-month follow-up by an intention-to-treat analysis, representing a follow-up rate of 58%.
General outcomes
The patients’ mean age was 48.1 years (standard deviation (SD): 10.8). The patients had a mean height of 1.68 m (SD: 0.08) and a mean weight of 78.03 kg (SD: 16.07). The mean body mass index was 27.58 (SD: 5.48). Even though 95.24% (200/210) of our patients underwent duplex sonography, which indicated sufficient eVP; we identified nine patients (4.29%) with treatment failure after 6 months. We detected one superficial vein thrombosis of the great saphenous vein, which was treated with compression therapy and anticoagulation with fondaparinux at 2.5 mg per day for 45 days. Overall, 88.57% (186/210) of the participants were satisfied with the outcome, and 92.86% (195/200) indicated they would undergo eVP again. Furthermore, the great saphenous vein was considered suitable as a bypass graft in 90.95% of the patients (Table 1).
Assessment of overall outcomes 6 months after external valvuloplasty (eVP) (eVP and the great saphenous vein (GSV) were assessed by duplex sonography).

Data are n (%).
Preoperatively, there were 111 (52.8%) patients with stage C2 disease and 50 (23.8%) patients with stage C3 disease according to the CEAP classification. After eVP, there were 137 (65.2%) patients with spider veins or telangiectasia, and 62 (29.52%) patients received additional sclerotherapy within the 6-month follow-up. No patients had stage C5 or C6 disease (Table 2). The mean total VCSS was 4.76 (SD: 2.13) preoperatively, 2.58 (SD: 1.78) 6 weeks after surgery and 1.77 (SD: 1.57) 6 months postoperatively.
Clinical class of the CEAP classification before and 6 months after external valvuloplasty (eVP).
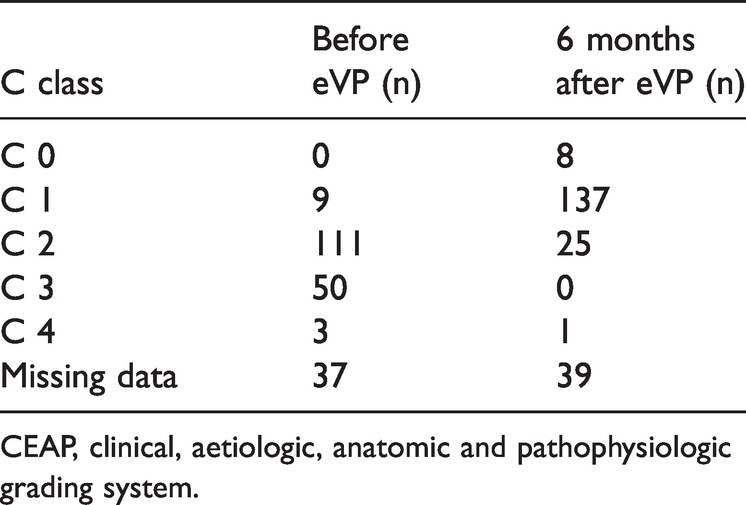
CEAP, clinical, aetiologic, anatomic and pathophysiologic grading system.
Reflux
Initially, most patients (141/210, 67.14%) had Hach stage I with reflux in the saphenofemoral junction continuing into the anterior accessory great saphenous vein. Three patients were classified as Hach 0, which represents a competent terminal valve preoperatively, but an incompetent preterminal valve, according to Stücker class 2. 26 Reflux changed after eVP treatment (Table 3).
Extent of reflux in the great saphenous vein before and 6 months after external valvuloplasty (eVP).

Hach 0 is defined preoperatively as a competent terminal valve, but an insufficient preterminal valve.
SFJ, saphenofemoral junction.
Diameter of the great saphenous vein
The mean diameter of the great saphenous vein at the saphenofemoral junction at the level of the terminal valve was 7.3 mm (SD: 1.91) before treatment. The mean diameter of the great saphenous vein 4 cm distal to the saphenofemoral junction was 4.4 mm (SD: 1.39) preoperatively, 3.8 mm (SD: 0.97) 6 weeks postoperatively and 3.9 mm (SD: 1.12) 6 months postoperatively. The mean diameter of the great saphenous vein at the mid-thigh was 3.7 mm (SD: 1.10) preoperatively, 3.4 mm (SD: 1.00) 6 weeks postoperatively and 3.5 mm (SD: 1.02) 6 months postoperatively. The mean diameter of the great saphenous vein at the knee was 3.6 mm (SD: 1.14) before eVP, 3.4 mm (SD: 0.97) 6 weeks after eVP and 3.3 mm (SD: 0.94) 6 months after eVP. Finally, the mean diameter of the great saphenous vein at the mid-calf was 3.1 mm (SD: 0.99) preoperatively, 2.9 mm (SD: 0.84) 6 weeks postoperatively and 2.9 mm (SD: 0.78) 6 months postoperatively. The values before and after eVP were statistically significant (p<0.05) whereas there was no significant difference between 6 weeks and 6 months (Table 4).
Diameters of the great saphenous vein (GSV) before and six months after external valvuloplasty (eVP) (SFJ: saphenofemoral junction).

Discussion
Our data demonstrated that the diameters of the great saphenous vein decreased significantly 6 months after eVP. Joh et al. showed that the diameters of the vein at the saphenofemoral junction and at the knee were significantly decreased 10 years after eVP. However, the authors could not demonstrate a reduction in the overall length of the vein. Notably, the authors did not precisely define the measurement points, and they reinvestigated only 32 limbs. 17 Furthermore, 61.3% of the patients had reflux in the proximal great saphenous vein, which could have influenced the results. 17 Sarac et al. 18 also found a decreased diameter of the great saphenous vein at the saphenofemoral junction. The authors described a significant reduction from 5.6 mm preoperatively to 3.1 mm postoperatively on the first postoperative day. Seven years after the treatment, the authors reported a mean diameter at the saphenofemoral junction of 4.5 mm, but did not state the significance level. 18 Geier et al. 15 measured the diameter of the great saphenous vein in their study with a 5-year follow-up. The authors reported a significant reduction in the great saphenous vein diameter from 7.1 mm to 4.3 mm at the great saphenous junction and from 6.5 mm to 4.5 mm 3 cm distal to the junction. 15 However, the surgical techniques differed in previous studies. Sarac et al. used a polytetrafluoroethylene (PTFE)-covered nitinol frame, and Lane et al.18,19 used a specially designed “exostent” device. Only the methods of Joh et al. and Geier et al. were similar to our technique, although Geier et al.15,17 used a piece of Dacron (Invista Inc., Wilmington, DE, USA) as a wrap.
In our previous study, we demonstrated decreased great saphenous vein diameters 6 weeks after eVP. 14 Patients were encouraged to wear compression stockings for 6 weeks postoperatively, which could have influenced the 6-week follow-up results. 14 In the current analysis, we demonstrated a significant decrease in the diameter of the great saphenous vein over its entire length 6 months after eVP. This indicates restored vein function because there were no statistically significant differences between the 6-week and 6-month results. Nevertheless, it remains unclear which factors are responsible for these findings. According to the ascending theory, 11 decreased venous volume in the leg following multiple phlebectomies can also decrease truncal diameter.27,28 Because all of our patients underwent multiple additional phlebectomies, the interpretation of these data is limited. Furthermore, 29.52% of our patients underwent additional sclerotherapy of spider veins or reticular veins during follow-up. It seems unlikely that the occlusion of spider veins affected the venous reservoir and subsequently the venous diameter of the great saphenous vein; however, this could have influenced our results.
The descending theory focuses on saphenous vein reflux with centrifugal progression of the disease, 29 which is the crucial point of eVP. Because reflux can develop in a multicentric way, 29 both factors (eVP and multiple phlebectomies) may have influenced our data concerning the reduction in the vein's diameters. Only long-term follow-up studies will address this issue.
eVP appears to be an effective treatment considering that 95.24% of our patients showed no reflux at the saphenofemoral junction 6 months postoperatively. Generally, reflux improved significantly, and the results are similar to findings in our previous study. 14 Surprisingly, three patients had great saphenous vein reflux from the saphenofemoral junction to the calf (Hach III stage) in this analysis. Unfortunately, eVP was insufficient treatment in nine patients; however, no further interventions to the great saphenous vein have been necessary to date. Nevertheless, it is feasible that these patients will require earlier additional treatment to address recurrent varicose veins, as reflux at the saphenofemoral junction is one of the most common causes of recurrent varicose veins. 30 However, the vein was preserved as a potential bypass graft in 9 of 10 cases. Overall, 88.57% of the patients were satisfied with the treatment, and 92.86% stated they would undergo eVP again, similar to the 6-week results in our previous study. 14 The most frequent reasons for dissatisfaction were new or remaining varicosities (n=4), restless legs or paraesthesia (n=2), hyperpigmentation (n=2) or non-improvement of symptoms (n=2). Even though C class grade decreased significantly, 65.2% (137/210) of our patients had spider veins or telangiectasia, and nearly one third (29.52%) underwent additional treatment with sclerotherapy.
Limitations
This study has certain limitations. First, we had a high lost-to-follow-up rate, and we reinvestigated only 210 of 359 patients, which represents a follow-up rate of only 58%. We attempted to motivate patients to participate in the follow-up examination using multiple phone calls. However, as re-examinations mainly took place in the afternoon, the majority of patients did not respond for occupational reasons. Nevertheless, the population’s general data were similar to the preoperative and 6-week data, indicating a comparable study population. 14 eVP is limited to approximately 15% of all patients 15 and patients with reflux at the saphenofemoral junction and continuing reflux in the accessory anterior saphenous vein benefit the most from eVP. 14 Therefore, our data represent a highly selective group of patients, which is a further limitation. Moreover, we had a high number of missing data for the reflux measurements, which is another strong limitation. Overall, this was an intention-to treat-analysis, and we evaluated 210 patients from five vein centres, which is a strength of this study. In contrast to other studies,15,17,18 we measured the diameter of the great saphenous vein over its entire length at predefined measurement points, which represents another advantage.
Conclusion
eVP appears to be a sufficient treatment strategy to reduce venous reflux at the saphenofemoral junction; 95.24% of our patients achieved sufficient venous reconstruction of the function of the terminal and preterminal valves. Furthermore, the C class of the CEAP classification and VCSS scores improved significantly after eVP. The diameters of the entire great saphenous vein decreased significantly 6 months after eVP.
Footnotes
Acknowledgment
This manuscript was created under a rehabilitation scholarship from the Ruhr University Bochum (supported by Bauerfeind AG).
Declaration of conflicting interest
Markus Stücker received consulting fees from Bauerfeind AG.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
TH, AM and MS searched the literature and conceived the study. BG, SRS, NF, DS, HS and DM were involved in protocol development and patient recruitment. TH was responsible for obtaining ethical approval. EB and DM conducted the statistical analyses. DM and TH wrote the first draft of the manuscript. All authors analysed and interpreted the data, critically revised the first draft for intellectual content and approved the final version of the manuscript.