
Abstract
Objective
Diagnosing periprosthetic joint infection (PJI) can be challenging. The ability to distinguish between septic and aseptic failure of a joint prosthesis is crucial for treatment strategy optimisation and prognosis prediction. Preoperative tissue cultures are included in many diagnostic algorithms; however, studies report different degrees of concordance (63%–85%) with intraoperative cultures. This study aimed to investigate the diagnostic performance of tissue biopsies in the preoperative diagnostic process with the 2018 International Consensus Meeting criteria as a reference and to describe the concordance between microbiological findings in pre- and intraoperative biopsies.
Methods
This observational retrospective study included 44 patients requiring revision surgery of a total hip or knee arthroplasty, where the diagnostic workup included biopsies of periprosthetic tissue. The accuracy of preoperative biopsies was calculated, and concordance between microbiological findings in pre- and intraoperative biopsies was described.
Results
The accuracy was 59%, with a sensitivity of 50% and specificity of 79%. Full concordance between microbiological findings in pre- and intraoperative biopsies was found in 64% of the cases.
Conclusion
An open biopsy of periprosthetic tissue cannot reliably confirm or exclude PJI, and, therefore, should not be performed.
Keywords
Introduction
Diagnosing periprosthetic joint infection (PJI) continues to be a major challenge. The ability to distinguish between septic and aseptic failure of a joint prosthesis is critical, given that the treatment for PJI necessitates unique surgical strategies and the precise identification of any pathogen and its susceptibility pattern to targeted antibiotic treatment. There are different algorithms to diagnose PJI;1–3 one of the most widely applied is the 2018 International Consensus Meeting (ICM) criteria. 2 Joint biopsy with sampling of periprosthetic tissue is proposed in the preoperative diagnostic workup. The procedures can be performed arthroscopically through needle biopsy or as open incisional biopsies; neither approach has been proven superior.4–7 Most studies investigating the accuracy of preoperative tissue biopsies in the diagnosis of chronic PJI use intraoperative biopsies as a reference and report a high sensitivity (range: 82%–100%), specificity (range: 97%–98%) and accuracy (range: 91%–97%).6–10 The 2018 ICM criteria 2 are widely used to define PJI in clinical practice and should be considered a useful reference to evaluate the accuracy of diagnostic biopsies.
Microbiological findings in preoperative biopsies may not entirely correspond to the intraoperative findings. Studies assessing the agreement between preoperative and intraoperative biopsies show concordance rates ranging from 63% to 85%.7,11,12
This observational retrospective study aimed to investigate the diagnostic performance of tissue biopsies as part of the preoperative diagnostic process with the 2018 ICM criteria as a reference. Moreover, we sought to investigate the concordance between pre- and intraoperative tissue biopsy microbiological culture results.
The aim of the study was to analyse whether an open biopsy of periprosthetic tissue can reliably confirm or exclude PJI.
Methods
Patients who required revision surgery of total hip or knee arthroplasty because of non-functioning components with pain, loosening or both were included in our study. All patients were treated at Uppsala University Hospital, and all patient data were de-identified. The reporting of this study conforms to the STROBE guidelines. 13
The indication for revision surgery was determined by an experienced arthroplasty revision surgeon. All patients underwent a full diagnostic workup 2 before revision surgery, including periprosthetic tissue biopsies. Patients with acute exogenous or haematogenous PJI and patients with verified chronic PJI (fistula or chronic antibiotic treatment) were excluded. The median time between the index surgery and the diagnostic workup with preoperative tissue cultures was 29 months (range: 4–169). Patients were not given antibiotics for ≥4 weeks preceding the pre- or intraoperative biopsy procedure to minimise the risk of antibiotic-induced false-negative results. 14
The preoperative biopsy samples were taken in a separate session, in sterile conditions in an operating theatre with the patient under general anaesthesia. The biopsies were obtained in an open incision with sampling of the periprosthetic tissue near the prosthesis in an open anterolateral approach at the hip and an anterior approach at the knee. For every biopsy site, a new forceps was used to prevent contamination. Prophylactic perioperative antibiotics as a single dose of cloxacillin (2 g) were administered once all samples had been obtained. Revision surgery was then performed in all cases, and at least five intraoperative tissue biopsies for culture were obtained. All tissue samples were placed in sterile tubes and immediately transferred to the microbiological laboratory. In accordance with standard procedure, cultures were discontinued and declared negative if no growth was reported after 14 days. 15 The median time period between the diagnostic workup with preoperative tissue cultures and revision surgery was 47 days (range: 8–181).
The preoperative workup and the intraoperative findings were used to define PJI in accordance with the 2018 ICM criteria. 2 Microbiological findings were considered relevant if at least two tissue biopsy cultures detected the same pathogen. On the basis of these results, the accuracy of the preoperative biopsies was calculated and concordance between pre- and intraoperative cultures was noted.
To evaluate the concordance between the preoperative and intraoperative microbiological results from the tissue biopsies, categorisation was performed, as follows:
(1) Full concordance: the same pathogen was identified in pre- and intraoperative tissue biopsy cultures (2) Preoperative (preop) pathogen: pathogen detection only in preoperative tissue biopsy culture (3) Intraoperative (intraop) pathogen: pathogen detection only in intraoperative tissue biopsy culture (4) Discordance: different pathogens in the pre- and intraoperative tissue biopsy cultures
This study design was reviewed and approved by the Human Research Ethics Committee in Uppsala, Sweden (Dnr 2019-03126). Patient consent for this study was not required by the Human Research Ethics Committee.
Statistics
Values for sensitivity, specificity, positive (PPV) and negative predictive value (NPV) and accuracy were calculated with their 95% confidence intervals (CIs). All reported p-values were two-sided, with a significance level of 0.05. Fisher's exact test was used to compare pathogen detection rates between pre- and intraoperative tissue samples. Statistical analyses were performed using IBM SPSS Statistics for Windows v. 27.0 (IBM Corp., Armonk, New York, USA).
Results
This study included 44 patients (18 women) who required revision surgery of total hip (n = 31) or knee arthroplasty (n = 13). The median age was 67 (range: 50–86) years.
After the preoperative workup and obtaining the intraoperative findings, 33 of 44 patients fulfilled the 2018 ICM criteria for PJI. The diagnostic accuracy of the preoperative biopsies was 59%, with a sensitivity of 50% and specificity of 79%. The PPV was 83%, and the NPV was 42% (Table 1).
Diagnostic accuracy of preoperative tissue biopsies (n = 44).

ICM, International Consensus Meeting; PPV, positive predictive value; NPV, negative predictive value.
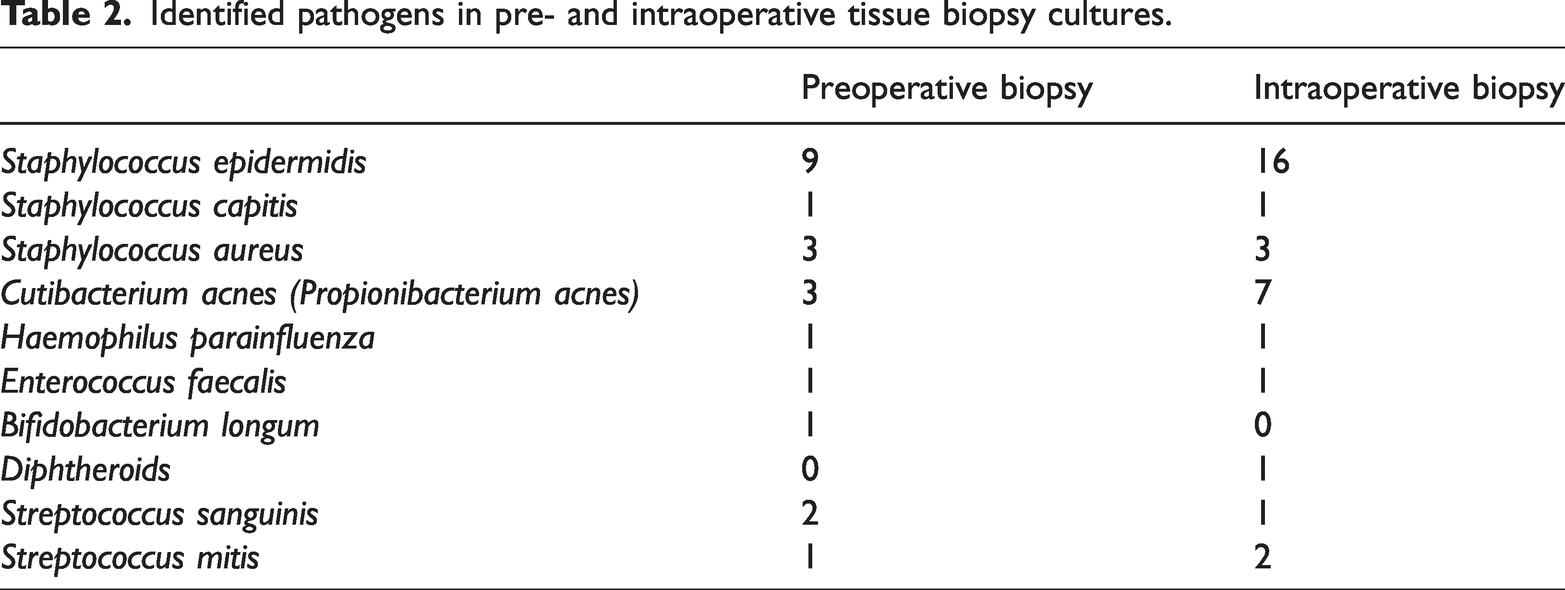
Pathogens detected in the pre- and intraoperative tissue biopsies are presented in Table 2. The most common pathogen was Staphylococcus epidermidis followed by Cutibacterium acnes.
Identified pathogens in pre- and intraoperative tissue biopsy cultures.
The same pathogen was identified in the pre- and intraoperative tissue biopsy cultures (full concordance) in 28 cases. In four cases, no pathogen was found in the intraoperative tissue biopsy culture, but a pathogen was isolated from the preoperative samples (preop pathogen). In 11 cases, no pathogen was found in the preoperative tissue biopsy; however, a pathogen was isolated from intraoperative samples (intraop pathogen). In one case, different microbiological findings were noted in the pre-and intraoperative tissue biopsy cultures (discordance) (Figure 1).

Concordance between pre- and intraoperative tissue biopsy culture results.
Discussion
Positive preoperative biopsies may be useful in confirming a PJI diagnosis. A specificity of 79% and PPV of 83% were shown in this study. In contrast, we found a sensitivity of 50% and NPV of 42%, indicating that negative preoperative biopsies are not sufficiently reliable to exclude PJI. Additionally, full concordance between pre- and intraoperative tissue cultures was shown in only 64% of the cases, which is of questionable reliability.
A comparable study of 63 patients that included exclusively chronic PJI after TKA showed a sensitivity of open incisional biopsies of 47% and a specificity of 77%. 16 Furthermore, a recent meta-analysis 17 showing a specificity of 96% and a sensitivity of 67% with preoperative tissue cultures also indicated that a large percentage of patients with negative biopsy culture results were later deemed to have PJI. In several studies6–10 the evaluation of preoperative cultures as a diagnostic method for PJI was made by comparing only preoperative with intraoperative cultures, the results of which may be inconclusive for diagnosing PJI. In this study, we used the 2018 ICM criteria as a reference when calculating accuracy, which comprises more factors than intraoperative cultures alone. We considered this approach the best reference to evaluate the accuracy of the diagnostic biopsies.
In other studies of PJI assessment, in 7% to 15% of the cases, no pathogen was found in biopsies obtained pre- or intraoperatively.18–20 We identified no pathogen in any of the biopsies in 9% of our patients, even though the patients fulfilled the ICM 2018 criteria for PJI. Poor sensitivity in pre- and intraoperative cultures can be explained by the low bacterial load in chronic low-grade infections, planktonic pathogens or prior antimicrobial treatment.21,22 In our study, all patients had a drug holiday of 4 weeks prior to the preoperative work-up and revision surgery to avoid false-negative results. This drug holiday period is commonly used9,23,24 although shorter drug holiday periods, such as 2 weeks, have been reported. 25 Another challenge in PJI diagnostics is the difference between microbiological findings in pre- and intraoperative tissue biopsies. During open revision surgery, the joint is extensively exposed, which may provide more reliable tissue cultures. Sampling from non-infected regions of the joint is a cause of culture-negative biopsies, 26 which can occur when obtaining tissue biopsies preoperatively, especially in late PJI cases caused by low-virulence pathogens, as in our study.
Full concordance between pre- and intraoperative tissue cultures was shown in 64% of the patients in our study. A study by Fink et al. 9 found a higher full concordance rate of 85% between pre-and intraoperative tissue biopsies compared with our study results. A pathogen was isolated solely from preoperative samples in 9% of the patients in our study, and in 25% of the patients, a pathogen was found only intraoperatively. In comparison, in a study by Karczewski et al. 27 including patients with a high suspicion of PJI (in accordance with the European Bone and Joint Infection Society definition), 1 no pathogen was detected in preoperative tissue biopsies; however, pathogens were detected in 42% of the intraoperative biopsies. Reasons for this lack of concordance in cultures comprise factors associated with weakening of bacterial detection, such as low bacterial load in chronic low-grade infections, presence of pathogens in biofilm, prior antimicrobial treatment, contamination during preoperative biopsy assessment or inadequate processing of samples. Other possible causes of differences between the results of the two sampling procedures are deviations in the analysis process of the tissue biopsies (errors by the microbiologist, skin contamination from staff members), suppression of one pathogen by another during culture and contamination during the preoperative tissue biopsy procedure. 9 In contrast to the difficulty detecting causative bacteria, positive culture may represent contamination and does not automatically define infection except for high-virulence pathogens, which are rarely contaminants.21,22 In cases with an additional or different pathogen detected intraoperatively compared with preoperatively or a pathogen found only in intraoperative biopsies, the possibility of contamination during the diagnostic procedure cannot be ruled out. One patient in our study had completely different microbiological findings in the pre- and intraoperative biopsies, and all microbiological findings (pre- and intraoperative) where considered when choosing appropriate antibiotic treatment.
This study has several limitations, including the small sample size. There are studies with larger cohorts, such as the study by Fink et al. that included 508 patients with PJI after THA or TKA 9 and a study by Meermans et al. 28 that included 120 patients with PJI after THA or TKA. There are also studies with smaller cohorts, such as a study by Simon et al. that evaluated open biopsies from 32 patients with chronic PJI after THA and which reported comparable results to those in our study. 24 A recent study by Niemann et al. of 38 patients with PJI after THA and TKA reported a sensitivity of 67% and specificity of 89%. 29 These studies compared the results of intraoperative biopsies with those of preoperative biopsies when calculating accuracy. 24 A study by Klaber et al. of 126 patients with PJI after THA and TKA used the ICM 2013 criteria as a reference and obtained open biopsies. 25 The sensitivity and specificity reported in the study were 69% and 89%, respectively. 25 We used the 2018 ICM criteria as a reference when calculating accuracy and evaluated the entire panel of preoperative and intraoperative diagnostics and not only the intraoperative cultures. The 2018 ICM criteria are currently the most widely used in PJI diagnosis; however, there are other diagnostic criteria, such as those of the Infectious Diseases Society of America (IDSA) 3 and those of the European Bone and Joint Infection Society (EBJIS). 1 We are well aware of the possibility that using another algorithm could have affected the number of diagnosed PJIs in this study,30–32 and using another algorithm may have affected the accuracy in this study. The ICM 2018 criteria miss low-grade infections to a certain extent; 32 however, other criteria, such as those of the EBJIS can over-diagnose PJI. 33
As an additional limitation, at our hospital, the standard procedure is to incubate cultures for 14 days, as in several other hospitals.9,24,29 Incubation periods for low-virulence organisms can require additional time and may result in negative cultures if evaluated too soon. 34 The 14-day incubation period might have contributed to lowering the detection rate of low-virulence bacteria because these bacteria may require up to 21 days of incubation for detection. 35 However, a longer incubation period may lead to a higher risk of finding contaminants. 36 Although the 14-day incubation period could have impacted our results, we used the same incubation time for all biopsy cultures. Unfortunately, we do not have the benefit of histological examination of the tissue biopsies, and we could not use histology as part of the diagnostic criteria for PJI. The use of histology of the tissue biopsies in the diagnostic criteria would have been an advantage, as shown in other studies, 7 and its use could have affected the overall accuracy in this study.
Low sensitivity in preoperative tissue biopsy cultures and the lack of full concordance make clinical decisions associated with treatment strategies of chronic PJI difficult. Broad empirical antimicrobial treatment is intended to be used and started immediately after suspected PJI in revision surgery. 37 This treatment can continue until the intraoperative tissue cultures are available, irrespective of the pathogen identified in the preoperative assessment, especially in low-grade infections. 38 A systematic review from 2018 20 reported no consensus in the literature on a standardised protocol for antibiotic use, especially in culture-negative PJI.
As the accuracy of preoperative tissue biopsies varies in different studies, methodological studies are needed that address the question of where the difference between these studies lies. Furthermore, there is a need for studies investigating when the risk exceeds the benefit, and whether preoperative tissue biopsies contribute to the diagnosis of PJI.
Conclusion
An open biopsy and bacterial culture of periprosthetic tissue cannot reliably confirm or exclude PJI, and, therefore, should not be performed.
Footnotes
Author contributions
Both authors (HE and SL) contributed substantially to the conception and design of the study and acquisition, analysis and interpretation of the data. Both authors (HE and SL) were involved in drafting the manuscript and both provided final approval of the version to be published. Both authors (HE and SL) have participated sufficiently in the work to take public responsibility for appropriate portions of the content and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Availability of data and materials
The dataset generated and analysed during the current study is available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.