
Abstract
Background
Although low bone mineral density (BMD) is associated with an increased risk of fracture, few studies have assessed fracture rates in patients with human immunodeficiency virus (HIV).
Methods
The occurrence of subclinical fractures in patients with HIV was assessed. Pearson’s chi-square test was used to analyze the relationship between subclinical fractures and related factors.
Results
Fifty patients with HIV were included, among whom 11 were diagnosed with subclinical fractures. These 11 patients had a mean body mass index of 24.127 ± 3.482 kg/m2, smoked a mean of 142.091 ± 3.482 cigarettes/month, drank a mean of 61.545 ± 13.026 mL/day of alcohol, had a mean CD4+ T cell count of 247.727 ± 181.679 cells/mm3, had a mean duration of acquired immunodeficiency syndrome (AIDS) of 4.27 ± 0.786 years, and had a mean BMD of the third lumbar spine of 0.810 ± 0.063 g/cm3. The AIDS duration and BMD of the third lumbar spine were significantly associated with subclinical fractures. The BMD of the third lumbar spine was negatively correlated with subclinical fractures.
Conclusion
A significant negative correlation was found between the BMD of the third lumbar spine and subclinical fractures.
Keywords
Introduction
In patients with acquired immunodeficiency syndrome (AIDS), CD4+ T lymphocytes are attacked and the immune system is destroyed after infection with human immunodeficiency virus (HIV), resulting in various opportunistic infections or tumors and, in severe cases, death. 1 AIDS is a disease involving multiple organ systems throughout the body. In addition to lesions of the immune system, multisystem opportunistic infections and malignancies contribute to the complex clinical pathology of AIDS.2,3 AIDS is now one of the most serious public health problems worldwide, and no cure has yet been found. 4 Subclinical fracture in patients with AIDS, introduced by Gazzola et al. 5 in Italy, is a type of fracture that is incidentally found on radiographs of patients without clinical symptoms. Although the clinical symptoms are not obvious, subclinical fractures have a significant impact on clinical fractures in patients, and they are associated with an increased risk of vertebral fracture. Subclinical fractures have also been associated with increased mortality in patients with AIDS. 6
Bone mineral density (BMD) is an important indicator of bone strength. It reflects the degree of osteoporosis and is an important parameter for predicting the risk of fracture. 7 In recent years, low BMD and osteoporosis have been reported in men and women infected with HIV. Low BMD is more common in people with than without HIV.8,9 Age and steroid use are risk factors for subclinical fractures, while associations with alcohol use and substance abuse are weak. 5 Although the increased incidence of low BMD in patients with HIV causes an increased risk of fracture, few studies have assessed fracture rates in patients with HIV. There is increasing evidence that patients with HIV have a higher risk of osteoporotic fractures than the general population. 10
In the present study, we evaluated the incidence of subclinical fractures in patients with HIV. We also explored the independent risk factors for subclinical fractures in patients with HIV and the effect of BMD on subclinical fractures in these patients.
Methods
Patients
Patients with HIV who underwent orthopedic surgery at Beijing Ditan Hospital from January 2019 to April 2020 were recruited for this study. The inclusion criteria were an age of 20 to 55 years, male sex, diagnosis of HIV, no history of orthopedic surgery before admission, no history of anti-HIV treatment, and no history of steroid or antiretroviral drug use. The exclusion criteria were an age of <20 or >55 years; female sex; poor cardiac function, pulmonary function, or liver and kidney function; open fractures requiring emergency orthopedic surgery; HIV negativity; a history of anti-HIV treatment; and a history of steroid or antiretroviral drug use.
Ethics
This study was approved by the Ethics Committee of Beijing Ditan Hospital. Written informed consent was obtained from all patients and their families.
Judgment of subclinical fracture
The spinal deformity index (SDI) was calculated as follows. Standard T4–L4 lateral spine films were taken, the anteroposterior height of each vertebral body was measured, the height ratio was calculated, and the degree of fracture of each vertebral body was recorded in a semiquantitative manner with assignment of the following values: 0, normal vertebral body shape; 1, 20% to 25% vertebral compression; 2, 25% to 40% vertebral compression; and 3, ≥40% vertebral compression. The SDI was calculated as the sum of all fracture severity scores. Patients were diagnosed with subclinical fractures of the vertebral body when the SDI was 1 or >1. The occurrence of subclinical fractures in patients with HIV was assessed.5,8
Dual-energy X-ray absorptiometry was used to measure the BMD at the spine (QDR 2000 dual-energy X-ray densitometer; Hologic Inc., Marlborough, MA, USA). Two energy levels of photon beam ionizing radiation were used to measure the BMD (g/cm2), T score, standard deviation, and Z score from the mean value of 30-year-old normal people, and the standard deviation of the mean value obtained from subjects of the same age and gender. A T score of −1.0 standard deviation or higher is considered normal, a T score between −1.0 and −2.5 standard deviations is consistent with osteopenia, a T score of less than −2.5 standard deviations is consistent with osteoporosis, and a T score of less than −2.5 standard deviations with brittle fracture is consistent with severe osteoporosis.
Clinical indicators
The following patient data were recorded on admission: age, smoking status (measured as number of cigarettes/month), drinking history (alcohol consumption measured in mL/day, referring to alcohol consumption converted into 40% alcohol concentration alcoholic beverage), history of AIDS, height, weight, and body mass index (BMI). The peripheral blood CD4+ T cell count in cells/mm3 was measured by the Dynabeads assay 11 as follows. A total of 125 μL of fresh blood was placed in an EDTA tube (Solarbio, Beijing, China). Next, 350 μL of phosphate-buffered saline (Solarbio) and 25 μL of magnetized suspended particles were added. The tube was placed on a shaker at room temperature for 10 minutes. The magnetized particles were separated with a special magnetic densitometer and washed twice with phosphate-buffered saline. A total of 50 μL of lysing solution was used. Finally, the CD4+ T cells were counted with an epifluorescent microscope (Thermo Fisher, Waltham, MA, USA).
Statistical analysis
Data are presented as mean ± standard deviation. In terms of data stratification, the average of each variable was calculated. The high group was defined as higher than the average, and the low group was defined as lower than or equal to the average. The t-test and Pearson’s chi-square test were used to analyze the relationships between subclinical fractures and related factors in patients with HIV. All preoperative correlates were entered into a multifactorial linear regression model to quantify the severity of multicollinearity by calculating the variance inflation factor. Because our study focused on the effect of BMD on subclinical fractures in patients with HIV, we made judgments by linear fitting. Finally, we constructed receiver operating characteristic (ROC) curves and applied the area under the curve (AUC) to assess the precision and sensitivity of the BMD of the third lumbar spine, duration of AIDS, and age in diagnosing the severity of subclinical fracture in patients with HIV. Further, neural network models were constructed using the BMD of the third lumbar spine, duration of AIDS, and number of subclinical fractures to explore the predictive value of the former two for subclinical fractures.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). A P value of <0.05 was considered statistically significant.
Results
Baseline clinical data
An independent-samples t-test was used to tabulate the indicators of the patients’ clinical characteristics (Table 1). Age, the CD4+ T cell count, the duration of AIDS, and the BMD of the third lumbar spine were significantly correlated with subclinical fractures in patients with HIV (P < 0.001 for all).
Patients’ demographic data.

Data are presented as mean ± standard deviation.
Independent-samples t test was used to compare continuous data.
*P < 0.05.
BMI, body mass index; AIDS, acquired immunodeficiency syndrome; BMD, bone mineral density.
Chi-square results
Pearson’s chi-square test was performed to assess the relationship between relevant clinical parameters and subclinical fractures in patients with HIV. The results showed that age (P < 0.001), smoking (P = 0.025), the CD4+ T cell count (P < 0.001), the duration of AIDS (P < 0.001), and the BMD of the third lumbar spine (P < 0.001) were significantly associated with subclinical fractures in patients with HIV. However, neither the BMI nor alcohol consumption was significantly associated with subclinical fractures in patients with HIV (Table 2).
Association between clinical characteristics and subclinical fracture.

Pearson’s chi-squared test was used.
*P < 0.05.
BMI, body mass index; AIDS, acquired immunodeficiency syndrome; BMD, bone mineral density.
Multiple linear regression
The multiple linear regression analysis showed that age and the duration of AIDS were positively correlated with subclinical fractures in patients with HIV and that the BMD of the third lumbar spine was negatively correlated with subclinical fractures in patients with HIV (Table 3).
Effect of clinical characteristics (P < 0.05 in independent-samples t-test) on subclinical fracture (yes/no) based on multiple linear regression.
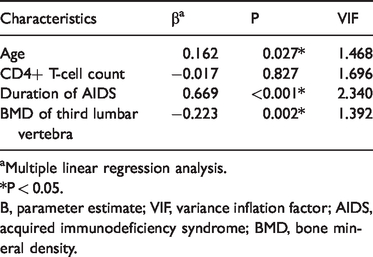
aMultiple linear regression analysis.
*P < 0.05.
Β, parameter estimate; VIF, variance inflation factor; AIDS, acquired immunodeficiency syndrome; BMD, bone mineral density.
Scatter plot
The BMD of the third lumbar spine was negatively correlated with subclinical fractures in patients with HIV (Figure 1(a)), and the duration of AIDS was positively correlated with subclinical fractures in patients with HIV (Figure 1(b)).
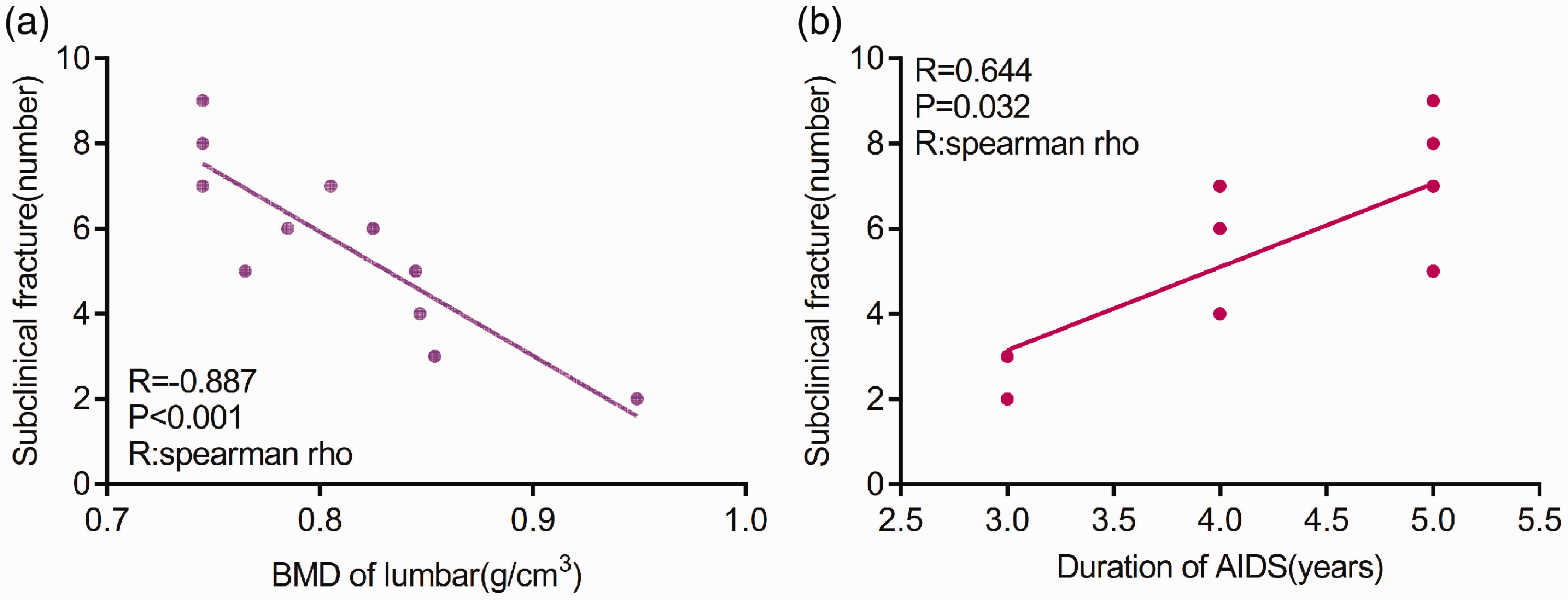
Correlation analysis. (a) The BMD of the third lumbar spine was negatively correlated with subclinical fractures in patients with HIV. (b) The duration of AIDS was positively correlated with subclinical fractures in patients with HIV.
ROC curve
ROC curves were constructed to determine the effects of patient-related parameters on subclinical fractures in patients with HIV, and the AUC was used to determine the degree of confidence. The AUC of age, the duration of AIDS, and the BMD of the third lumbar spine was 0.959, 0.998, and 0.953, respectively (P < 0.001 for all) (Figure 2).

ROC curves. (a) ROC curve of age for subclinical fractures. (b) ROC curve of duration of AIDS for subclinical fractures. (c) ROC curve of the BMD of the third lumbar spine for subclinical fractures.
Neural network model
A neural network is a type of nontraditional multiple nonlinear model that has no requirements regarding variable type. The pathogenesis of a disease is a complex process affected by multiple factors. Traditional statistical methods often require normality and independence of variables, greatly limiting the prediction of disease. The advantages of a neural network are suitable for the prediction of disease risk. Additionally, the construction of a neural network prediction model can avoid interference by subjective factors. After training, the neural network prediction model in the present study reached the best effect, in which the gradient was 9.9641 × 10−6, validation was 0 (Figure 3(a), mean squared error was 0.0037106 at epoch 698 (Figure 3(b)), and relativity was 0.99437 (Figure 3(c)). Through verifying the predicted value of the data against the actual value, we found only small differences (Figure 3(d)). The neural network model revealed close relationships among the BMD of the third lumbar spine, the duration of AIDS, and subclinical fractures. Based on these results, we can speculate that the severity of BMD of the third lumbar spine and duration of AIDS might be predictive indexes of subclinical fracture.

Neural network model. (a) The neural network prediction model reached the best effect with a gradient of 9.9641 × 10−6 and validation of 0. (b) The mean squared error was 0.0037106 at an epoch of 698. (c) The relativity was 0.99437. (d) Only small differences were found through verification of the predicted value of the data against the actual value.
Discussion
The results of this study indicate that the prevalence of subclinical fractures in patients with HIV in China is 22.0%. The results of the multivariate linear regression showed that age was positively correlated with subclinical fractures in patients with HIV, the duration of AIDS was positively correlated with subclinical fractures in patients with HIV, and the BMD of the third lumbar spine was negatively correlated with subclinical fractures in patients with HIV (P < 0.05).
In this study, we found a positive correlation between age and the occurrence of subclinical fractures in patients with HIV. A cross-sectional study by Torti et al. 12 showed that the incidence of subclinical fractures in HIV-positive patients (26.9%) was twice that in healthy people (12.9%) and that HIV-positive patients were more likely to have osteoporosis. Furthermore, in a study of a healthy population, the probability of subclinical fracture was greater in elderly than young individuals. 13 Premaor and Compston 14 also suggested that among patients with HIV, a longer life span was associated with a higher prevalence of chronic diseases. Compared with the general population, the risk of osteoporosis and fractures (including vertebral fractures) is higher in patients with HIV, and harmful effects on bone health have been recognized.
A longer duration of AIDS is associated with a higher likelihood that the patient will develop subclinical fractures. We speculate that the following two factors contribute to this association. First, the HIV virus itself can directly invade and destroy bone cells and the bone marrow microenvironment. 15 Second, antiretroviral drugs can also cause bone loss. 16 Patients with HIV are more likely to sustain a subclinical fracture than those without HIV because the body’s bone mass is affected by the duration of their AIDS illness, and even low-energy trauma or a fall from a low height is sufficient to initiate a fracture. 17
BMD is an important marker of bone quality, reflects the degree of osteoporosis, and is an important basis for predicting the risk of fracture. Many studies have shown that the prevalence of bone disease in HIV-positive individuals is significantly higher than that in non-HIV-infected populations.10,18,19 People living with HIV have lower BMD than those living without HIV. 20 In one study, low BMD increased the risk of subclinical fractures in patients with AIDS; 67% of HIV-infected patients had osteopenia and approximately 15% had osteoporosis. 21 The present study showed an increased risk of subclinical fractures in HIV-infected patients with a lower BMD of the third lumbar spine, consistent with the above findings. Numerous studies have shown that antiretroviral therapy is associated with bone loss and decreased BMD and consequent subclinical fractures. 16 Das et al. 22 proposed that the risk of hip BMD loss may be increased in women aged >40 years taking antiretroviral regimens containing teicoplanin. Recent observational studies have shown a rapid decline in BMD in people living with HIV during the first 2 years of antiretroviral therapy.23,24 Antiretroviral therapy for AIDS can have both direct and indirect effects on phosphate and vitamin D metabolism, resulting in decreased BMD due to impaired bone mineralization. 25 Therefore, the selection of antiretroviral drugs with less bone toxicity is recommended. The mechanisms underlying the onset of bone mineral loss in HIV-infected individuals are unknown. Abnormalities in bone and mineral metabolism may be due to direct HIV viral invasion of bone cells and the bone marrow microenvironment, chronic T-cell activation and abnormal production of cytokines affecting osteoblast and osteoclast function, calcium homeostasis disorders, parathyroid hormone function, vitamin D metabolism, opportunistic or neoplastic diseases, and side effects of drugs.15,26 HIV infection of osteoclasts and bone marrow stromal cells, including apoptosis of osteoblasts and release of proinflammatory cytokines induced by HIV Gp120, is involved in the impairment of bone development and maturation. 27 According to Calmy et al., 28 HIV disrupts the function of osteoblasts and osteoclasts and breaks the original balance, which in turn affects the osteoprotegerin/receptor activator of the NF-κB/receptor activator of NF-κB ligand (OPG/RANK/RANKL) system and causes massive bone loss in patients with AIDS. Decreased BMD is associated with factors such as age, sex, low BMI, a high viral load, and a low CD4+ T-lymphocyte count.18,29,30 In addition, HIV can reportedly induce apoptosis of osteoblasts (bone marrow stem cells), which can continuously activate various types of proinflammatory cytokines and tumor necrosis factor in osteoblasts to induce apoptosis of osteoblasts, thus affecting bone mass in patients with AIDS.31,32 Other factors, such as a low blood calcium level, hypogonadism, hyperthyroidism, hyperparathyroidism, renal failure, heavy use of drugs such as opioids or heroin, abuse of glucocorticoids, menopause, smoking, and heavy drinking, can also lead to a higher risk of subclinical fracture in patients with than without HIV infection.33–36
Our study has two main limitations: First, the data sample was small and the results may have been subject to error. Studies with larger sample sizes are required to improve the accuracy of the analysis results. Second, further exploration is needed regarding the mechanisms involved in the influence of the BMD of the third lumbar spine on subclinical fractures in patients with HIV.
Conclusions
The multivariate regression analysis showed a significant negative correlation between the BMD of the third lumbar spine and subclinical fractures in patients with HIV, suggesting the necessity of regular X-ray examination and BMD screening.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by the Scientific Research Common Program of Beijing Municipal Commission of Education (KM201810025029), Capital’s Funds for Health Improvement and Research (2018-2-2174), and Beijing Municipal Science & Technology Commission (No. Z191100006619060).