
Abstract
Objective
To examine the sociodemographic and clinical characteristics of psychiatric patients with recurrent psychiatric readmissions (RPR).
Methods
A retrospective study was conducted at Hamad General Hospital in Qatar on psychiatric patients with recurrent readmissions from August 2018 to January 2019.
Results
Of 380 psychiatric patients admitted during the study period, 40 (10.5%) were readmitted within 30 days of discharge. Most of the patients who were readmitted were single, male and unemployed. Psychotic spectrum disorder was the most frequent psychiatric condition and was diagnosed in 18 (45%) patients. A total of 30% of the patients were receiving treatment with anti-psychotics, and a similar number received more than one medication. Most patients showed poor or no compliance. Only 12.5% of patients stayed in the hospital for more than 5 weeks in their last admission during the study period.
Conclusions
Poor compliance, male sex and single status were the most common demographic and clinical features of patients with RPR. Post-discharge psychiatric care should be tailored to meet the requirements of patients prone to RPR.
Keywords
Introduction
Recurrent psychiatric readmissions place additional strain on the health care system and make treatment more expensive.1–5 A higher readmission rate is generally considered an indicator of poor inpatient psychiatric services; post-discharge care, external stressors and other non-clinical factors are also recognized contributors.6–8 Psychiatric readmission has been studied extensively, and attempts have been made to identify its predictors.9–11 Age, educational level, socioeconomic status, psychiatric diagnosis, psychiatric treatment, previous history of psychiatric hospitalization, length of hospital stay, adherence to treatment post-discharge and substance abuse are frequently reported to be associated with a higher incidence of psychiatric readmission; however, there is no consensus on the predictors of readmission.3,5,11,12
Readmission after psychiatric discharge can stem from the natural progression of the patient’s underlying disease, a new illness or problem unrelated to the index admission, or the consequence of poor communication regarding the dose and schedule of medication or follow-up plans.11,13,14 With appropriate in-hospital and post-discharge care, however, a substantial number of readmissions can be prevented. A systematic review of 34 studies found the pooled median of avoidable readmissions to be 27.1%. 15 A subsequent observational study from 12 academic medical centres in the USA reported that approximately 27% of readmissions were potentially preventable. 16 Although these studies did not focus exclusively on psychiatric readmissions, careful monitoring of predictors of readmission and taking remedial action could reduce the readmission rate in the psychiatric care setting. 12
Factors affecting psychiatric readmissions are not restricted to the clinical domain but are multifaceted, encompassing individual, environmental and clinical dimensions.1,5,9,13,17–36 However, there is no consensus on the predictors of psychiatric readmission; for example, a large-scale cross-sectional analysis in the USA showed that length of stay is associated with risk of readmission within 30 days post-discharge. 31 However, a national case register study did not find that the length of hospital stay was an independent risk factor for readmission within 30 days, though age up to 45 years, short duration between index admission, and readmission and prior hospitalization were identified as risk factors. 37 Such discrepancies among reported potential risk factors were also documented in a recent systematic review. 11 The review found that sociodemographic variables and length of hospital stay were frequently reported predictors of psychiatric readmission; however, in most of the studies, several relevant factors (such as social support and prior hospitalization) were not discussed or accounted for.
Despite non-uniformity in terms of readmission time and study cohort, most studies underscore the need to identify factors that can minimize unplanned readmissions.12,37 Furthermore, considering the disparities among different countries in terms of in-hospital care protocols and post-discharge social support, it is vital to examine readmission patterns in countries with distinct demographic and socioeconomic structures. The Middle East has distinct sociodemographics; however, there have been only a few reports on psychiatric readmission from this region.38,39 Al-Shehhi et al. 38 investigated psychiatric readmissions during 1 year and reported that gender, employment status, adherence to medication and history of a previous admission were independent predictors of readmission. In another notable study that involved two hospitals from two countries in the Middle East (Egypt and Saudi Arabia), perceived social support, medication adherence and duration of last hospital admission were factors identified as playing a role in readmission within 6 months. 39 Qatar is in the Middle East and has a high human development index and high per capita income; however, there are no reports on the demographic and clinical aspects of psychiatric readmission in Qatar.
The ‘revolving door’ phenomenon is a term coined to define recurrent psychiatric readmissions. 40 Such patients are often chronically ill and need specific attention in terms of in-hospital psychiatric care, transitional care and post-discharge care. 41 However, little information is available on the demographic and clinical characteristics of such patients. This descriptive study aimed to analyse the sociodemographic and clinical characteristics of patients with recurrent psychiatric readmissions in Qatar.
To mitigate the burden of mental disorders, research is needed on a range of risk factors associated with readmission. However, in this study, we focused only on sociodemographic factors related to readmission.
Method
Study design and sample
This retrospective chart review was conducted over 6 months from August 2018 to January 2019 at Hamad General Hospital in Qatar. Participants were patients admitted to the hospital’s emergency department within 30 days of discharge after receiving psychiatric treatment. Only patients who showed the revolving door phenomenon (recurrent readmission) during the study period were considered 40 and their second or subsequent readmission was included. All these patients were in the current period of treatment and were selected consecutively. Data on the last admission and readmissions within 30 days of the previous admission were extracted from the computerized medical records.
Setting
The Mental Health Service at Hamad Medical Corporation is the primary provider of specialized mental health care and treatment in Qatar. The Mental Health Service provides a range of acute and community-based services, including outpatient clinics, inpatient care, consultation/liaison, child and adolescent mental health services, geriatric psychiatry and emergency services, which are provided in different locations across the country. The Mental Health Service also provides residency training in psychiatry and various fellowship programs, in addition to teaching medical students from Qatar University and Weil Cornel medical college. The Accreditation Council for Graduate Medical Education International accredited the residency training in 2013.
Procedure
The readmission rate was defined based on the proportion of patients who had repeat hospitalization for non-elective reasons within 30 days of discharge. 8 Good compliance was defined as patients who followed the prescribed schedule and medication dosages; poor compliance was defined as patients who took only a portion of their prescribed medications, and non-compliance was defined as patients who did not take the prescribed medicine. Socioeconomic status was defined based on the monthly household income as per the national standard. Violence was defined according to the World Health Organization as the ‘intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation’. 42 This definition encompasses all forms of violence, which are further divided into self-inflicted, interpersonal and collective violence. If the patient was living with family in the same house, he/she was considered to have social support, and lack of social support was defined as living in a separate part of the house or living alone. The data were collected using a structured questionnaire that included items on date of most recent admission, nationality, age group, marital status, availability of social support, education level, employment status, financial status, forensic history, history of violence, substance abuse, psychiatric diagnosis, previous admissions, duration of illness, compliance, length of stay for the last admission, involuntary admission, treatment received in the last entry and discharge to community care.
Ethical statement and consent
Ethical approval was obtained from the mental health research committee (approval number QRS/PSY/T002/2018). As this was a retrospective study and the participants were anonymous, the review board of the Hamad Medical Corporation Mental Health Service waived the requirement for informed consent.
Statistical analysis
Continuous variables are presented as the mean and standard deviation and categorical variables as the number (percentage). SPSS Statistics for Windows, Version 22 (IBM Corp., Armonk, NY, USA), was used for data entry and statistical analysis.
Results
During the study period, 40 (10.5%) of 380 patients who received psychiatric treatment were readmitted within 30 days of the index admission. A total of 30% (n = 12) of the readmitted patients were women. No patient was older than 64 years, and 9 (22.5%) were aged 20 years or younger. Of the readmitted patients, 19 (47.5%) were from Qatar, 13 (32.5%) were from Asia, 7 (17.5%) were from Africa and 1 (2.5%) was from the USA; 29 (72.5%) of the patients were single, 10 (25%) were married and 1 (2.5%) was divorced (Table 1).
Patient demographic and socioeconomic characteristics (n = 40).
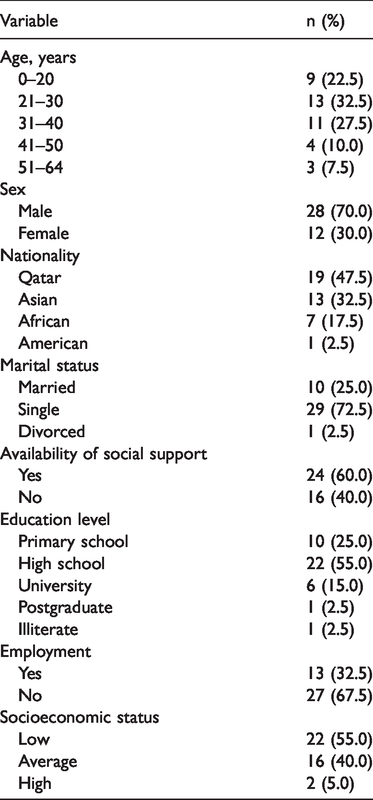
Twenty-four (60%) of the patients had social support and 13 (32.5%) were employed. Socioeconomic status was classified as low in 22 (55%) patients, average in 16 (40%) and high in 2 (5%). Of all readmitted patients, 32 (80%) had primary school or high school education, 1 patient (2.5%) was illiterate and 6 (15%) had tertiary education (Table 1).
Most patients (n = 28, 70%) had no forensic history, 9 (22.5%) were current or former prisoners and 3 (7.5%) had a prosecution order. A total of 10 patients (25%) had no history of violence; 13 (32.5%), 11 (27.5%) and 1 (2.5%) had a history of harming others, deliberate self-harm and harm to property, respectively. There were 5 patients (12.5%) with a history of perpetrating more than one type of violence. Substance abuse was noted as a problem during admission in 7 patients (17.5%); most of the patients (65%, n = 26) were not admitted for suicidal tendencies (Table 2).
Behavioural and clinical characteristics of patients (n = 40).

Psychotic spectrum disorder was the most frequent diagnosis, n = 18 (45%), and 12 (30%) patients had a diagnosis of mood disorder. The duration of illness was less than a year in 14 (35%) patients, 1 to 2 years in 6 (15%) patients, 3 to 4 years in 2 (5%) patients and ≥5 years in 18 (45%) patients. Twelve patients (30%) were receiving anti-psychotics, 7 (17.5%) were taking anti-depressants and 12 (30%) were on more than one medication. There were 5 patients (12.5%) who received no treatment and 3 (7.5%) who received a depot injection (Table 2; Figure 1).

Spectrum of psychiatric disorders (a) and treatment modalities (b) among patients (n = 40).
The length of hospital stay during the last admission was less than a week for 13 patients (32.5%), 1 to 2 weeks for 14 (35%) and 3 to 4 weeks for 8 (20%). Five patients (12.5%) stayed in the hospital for ≥5 weeks. The admission was voluntary in 31 patients (77.5%). Of patients, 22 (55%) had a history of one to two psychiatric admissions and 9 (22.5%) were admitted five or more times. Compliance was poor in 17 patients (42.5%) and good in 13 (32.5%). Ten patients (25%) were deemed non-compliant, and 9 patients (22.5%) were referred to a community psychiatry centre (Table 2).
Subgroup analysis of sex was also performed. In the group aged up to 20 years, the proportion of men and women was 21.4% and 25%, respectively. Approximately 54% of men and 75% of women were aged 20 to 40 years. None of the women and 25% of the men were older than 40 years. Involuntary admission was documented in approximately 17% of women and 25% of men. Approximately 54% of men and 83% of women had no suicidal tendencies. Substance abuse was documented in 25% of men but not in any women. Compliance was deemed good in approximately 39% of men and 16.7% of women.
Discussion
Although this study focused mainly on the sociodemographic features of readmitted patients, we firmly believe that rather than just attempting to reduce readmissions, psychiatric hospitals could examine the types of individuals who are repeatedly admitted and create interventions aimed at improving the functionality and the long-term outcome of these patients in the community.
In this study, the rate of readmission within 30 days of the last admission was 10.5%. Readmission rate within 30 days was reported to be 13% in a national case register study from Israel and 16% in a large study from the USA.37,43 However, data on 30-day readmission rates in the Middle East are not available; the 1-year readmission rate was reported to be 39% in a study from Oman. 38 Although our readmission rate compares favourably with the rates reported in these international studies, an exact comparison is difficult because of the potential differences in inclusion criteria, clinical practices and post-discharge care services across the different studies. Another difference is that only recurrent admissions were considered in the present study.10,17,25–28,44–46
Most of the patients readmitted in our study were men. Male sex is reported to be a predictor of psychiatric readmission. Lin et al. 47 found that being male was associated with an increased risk of readmission irrespective of the duration of follow-up. Male sex has also been explicitly addressed in the context of the revolving door phenomenon and found to be a risk factor. 48 Woo et al. and other researchers have reported similar findings.46,49 In our subgroup analysis of patient sex, substance abuse and suicide-related factors were predominantly observed in men, although the difference did not reach statistical significance. Single relationship status has also been identified as a significant predictor of readmission. 49 In a study conducted in two Arab hospitals, male patients who were unemployed, unmarried and had no education beyond primary school had an increased risk of early readmission. 39 That most of our patients had not been educated to high school level and most were single and unemployed supports the previously reported effects of education level and employment status.39,49
Poor or no compliance was observed in most patients in this study. Poor adherence to medications is an independent predictor of readmission in several studies.38,50–53 In our study, 32% of the patients tended to harm others, and most had no suicidal ideation. Approximately 75% of our patients displayed some type of violence, although most did not have any forensic history. These results are in line with those reported in other studies.11,34,38 In our study, the absence of any specific trend in the relative incidence of readmission with an increase in the length of stay indicates that length of stay at index admission may not necessarily affect the readmission rate. 51 Furthermore, most of our patients were of low to average socioeconomic status, supporting the view that socioeconomic status may affect readmission rate.7,13,54
In the present study, psychotic spectrum disorder was the most common diagnosis, followed by mood disorder. Morris et al. 34 identified psychotic disorders in 26%, mood disorders in 36% and substance use disorders in 51% of patients readmitted to the emergency department within 30-day post-discharge. Interestingly, another 30-day post-discharge readmission study identified psychotic disorders in more than 50% of patients. 31 We identified substance abuse in only 17.5% of patients, none of who were women. The suggestion that substance abuse shows cultural or regional variability can be partly attributed to such variations.14,17,21,28,29 Anti-psychotic agents were prescribed for 30% of our patients and a similar percentage was receiving more than one medication. Approximately 18% of patients were prescribed an anti-depressant; for 7.5% of these patients, treatment was administered as a depot injection. Treatment via depot injection is reportedly a risk factor for readmission, whereas the use of an orally administered anti-psychotic agent is a protective factor. 11 However, because most of our patients were readmitted despite being on medication, further exploration of the effect of psychiatric medication on readmission, and specific focus on post-discharge compliance, is required.
The main limitation of this descriptive study was its retrospective design, which meant that only variables for which data were available in the medical records could be examined. The absence of any comparison with a group of patients who did not show recurrent readmission is another limitation that precluded a detailed statistical analysis. We have discussed the observed differences in the relative incidences in light of previously reported studies on risk factors for readmission; however, as a standalone study, this work cannot confirm such associations. We were also unable to evaluate the severity of symptoms or obtain current data clarifying how long a patient continued medication upon discharge into the community. Data on the access to community mental health services were not collected; such data are necessary to fully understand post-discharge factors. Despite these limitations, this study addresses a research gap and provides valuable information on different aspects of recurrent psychiatric readmission rates in Qatar. Our findings corroborate those of several international studies and add useful information to the global pool of data for this population. The results suggest that single and unemployed men are the most represented among readmitted patients; therefore, special attention should be paid to this group in discharge planning and follow-up. Another important clinical implication of this study is that compliance adherence should be given a high priority in patient education and follow-up, as most of the readmitted patients had poor or no compliance.
Further research is needed to understand the different aspects of this complex issue in more depth and to explore interventions that could reduce readmission rates. Other areas of investigation should include the effectiveness of pre-discharge factors, such as patient education, discharge planning, reconciliation of medication and scheduling a follow-up appointment, as well as post-discharge interventions such as access to community mental health services, follow-up telephone calls, communication with community mental health providers and home visits. Research is also needed on bridging interventions, such as transition coaches, patient-centred discharge instructions and continuity of clinical care between inpatient and outpatient settings. Greater referral of patients with limited social support and poor compliance with medication to community psychiatry centres may also be helpful.
In summary, this study identified several distinct demographic and clinical features of patients who had recurrent readmissions after psychiatric treatment. The readmission rate in our study was in line with internationally reported values. Patients in this study were relatively young, unemployed chronic patients with a substantial history of violence, recurrent readmissions and psychotic spectrum disorder (or more than one diagnosis). Psychotic spectrum disorder and mood disorder were the most common diagnoses, whereas substance use disorder showed low frequency. However, no specific patterns were observed in the length of hospital stay in the last admission or the duration of illness. More men than women were in the recurrently readmitted patients. Further studies are needed to analyse predictors for recurrent admissions. Psychiatric services and patient care practices should be tailored to focus on populations that are more prone to the risk of recurrent readmission.
Footnotes
Acknowledgement
We are sincerely grateful to our colleagues who helped to collect the data analysed in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.