
Abstract
Spontaneous cerebrospinal fluid hypovolemia (SCFH) is an uncommon entity in neurosurgical practice. Without early recognition and management, some patients with SCFH can develop chronic subdural hematoma (CSDH). Generally, management of patients with SCFH without CSDH is relatively straightforward. However, this circumstance becomes more complicated in patients with concurrent CSDH. Treatment measures simply based on the respective management principles of SCFH and CSDH are insufficient or even disastrous. Our previous study showed that reinforced restriction of physical activity was a promising strategy in managing CSDH in the general population. We applied this strategy in three consecutive patients with SCFH and massive CSDH. All of the patients experienced complete resolution of CSDH. This study not only enriches the basic theory of formation and progression of CSDH, but also demonstrates that reinforced restriction of physical activity could be treated as an alternative or adjuvant management of CSDH secondary to SCFH.
Keywords
Introduction
Spontaneous cerebrospinal fluid hypovolemia (SCFH) or spontaneous intracranial hypotension (SIH), which is characterized by orthostatic headache and collapse of the ventricular system, is an uncommon entity in neurosurgical practice. 1 The widely accepted mechanism underlying SCFH is cerebrospinal fluid (CSF) leakage at any site along the spinal dura mater. Without early recognition and management of SCFH, some patients with SCFH can develop chronic subdural hematoma (CSDH). 2 The reported incidence of CSDH can be higher than 30% in patients with SCHF.3,4 Generally, management of SCFH in patients without CSDH is relatively straightforward, for which intravenous hydration, bed rest, and an epidural blood patch are effective measures.1,2,4 However, this condition becomes more complicated in patients with concurrent CSDH. In patients with massive CSDH, evacuation of the CSDH and management of SCFH should be considered simultaneously. A surgical procedure is not without risk. According to previous reports, evacuation of the CSDH might cause fatal outcomes.5,6
In our recent prospective study, we showed that after reinforced restriction of physical activity all of the patients with CSDH experienced spontaneous resolution. 7 Therefore, we hypothesized that physical activity plays an important role in formation and progression of CSDH. Additionally, reinforced restriction of physical activity could also be used in patients with CSDH secondary to SCFH. In this study, we report three patients with SCFH-associated massive CSDH who experienced spontaneous resolution of the CSDH after reinforced restriction of physical activity.
Case report
Case 1
A 49-year-old man was admitted with an orthostatic headache for 1 month. He denied a history of head trauma and any defined chronic disease. No history of administration of antiplatelet or anticoagulation agents was reported. He was alert and correctly obeyed commands. A physical examination of the neurological system was unremarkable. Head computed tomography (CT) on admission showed bilateral CSDH and collapse of the ventricular system (Figure 1a–c). Gadolinium-contrasted magnetic resonance imaging (MRI) showed diffuse pachymeningeal enhancement (Figure 1d).
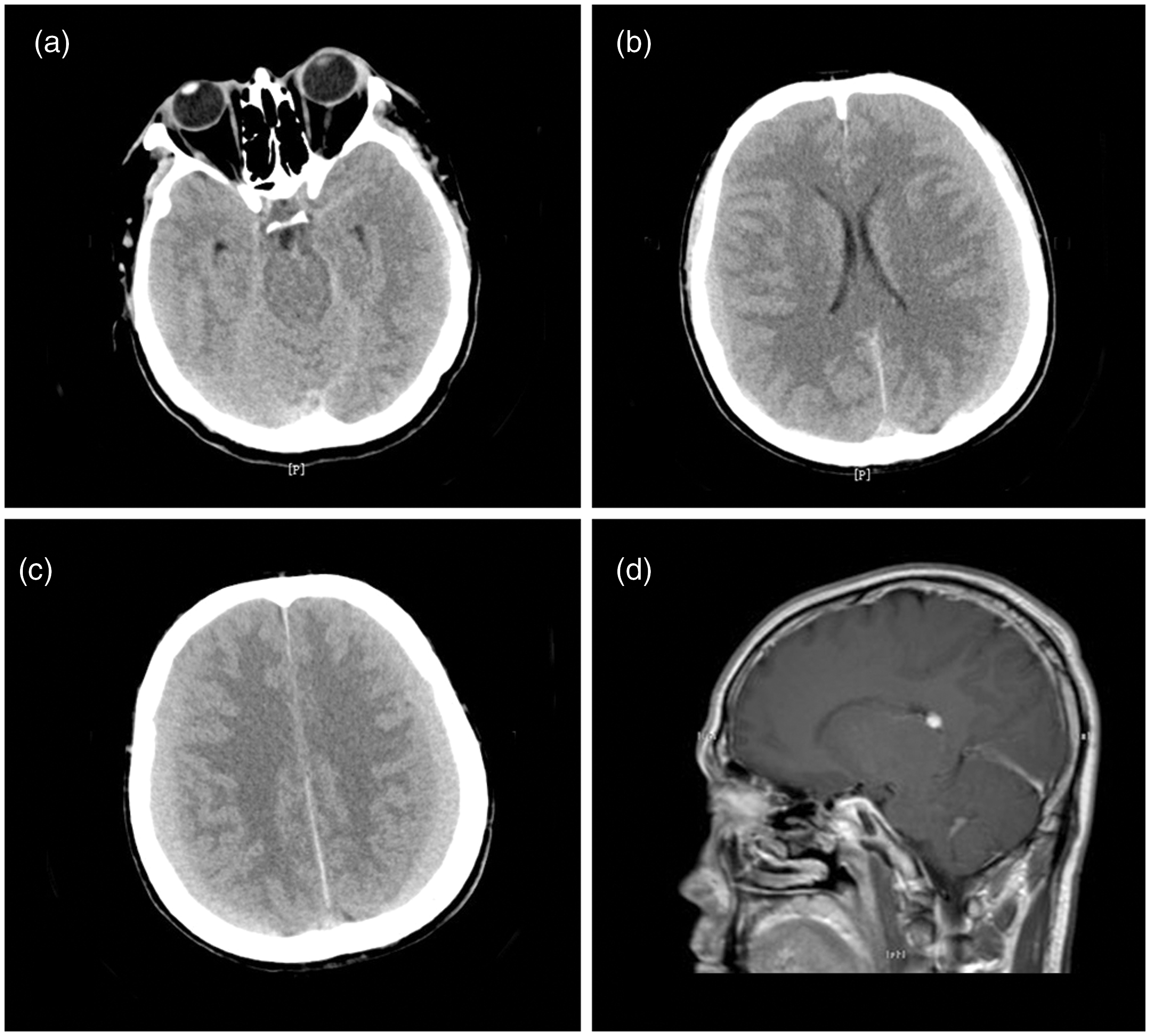
Head computed tomography of case 1 shows effacement of the ambient cistern (a), collapse of the lateral ventricles, and bilateral isodense chronic subdural hematoma (b, c). Sagittal view of gadolinium-contrasted magnetic resonance imaging shows diffuse pachymeningeal enhancement (d).
A diagnosis of CSDH secondary to SCFH was made. Further T2*-weighted MRI of the whole spine was performed but failed to show any sign of CSF leakage. The patient refused further myelography. Because his mental state was stable and no tendency of exacerbation was noticed, conservative treatment with reinforced restriction of physical activity 7 was proposed. He was discharged and regularly followed up at the outpatient department. CT performed 81 days after his first CT scan showed partial resolution of the CSDH and re-expansion of the ventricular system (Figure 2a, b). His symptom of the orthostatic headache had completely resolved and he reported no other complaint. Another CT scan was performed 103 later and showed complete resolution of the CSDH (Figure 2c, d). He was free of any previous symptoms and returned to normal daily work at a 1-year follow-up.

Computed tomography of case 1 shows partial resolution of the chronic subdural hematoma and re-expansion of the lateral ventricles and ambient cistern (a, b). Computed tomography shows complete resolution of the chronic subdural hematoma, normal lateral ventricles, and ambient cistern (c, d).
Case 2
A 53-year-old man was admitted for an orthostatic headache and diplopia that lasted for longer than 20 days. He denied a history of recent head trauma and any specific medication, and he was alert. A neurological examination showed incomplete abducens palsy of the right eye. Head CT performed at admission showed bilateral CSDH and effacement of the brain sulcus (Figure 3a, b). Further MRI showed brain sagging (Figure 3c). Opening pressure on lumbar puncture at the lateral decubitus position was 60 mmH2O. A diagnosis of CSDH secondary to SCFH was made on the basis of his history of present illness and head imaging. He was advised to have reinforced restriction of physical activity. During 3 days’ inpatient observation, he was stable in the neurological state and reported only a mild headache in the supine position. He was discharged and was followed up at the outpatient department. CT was performed 40 days later and showed partial resolution of the CSDH (Figure 3d). Another CT scan that was performed 63 days later showed complete resolution of the CSDH. He was free of any symptoms during a 1-year follow-up.

Computed tomography of case 2 shows bilateral isodense chronic subdural hematoma and effacement of the brain sulcus (a, b). Sagittal T2-weighted imaging on magnetic resonance imaging shows brain sagging (c). Computed tomography shows partial resolution of the chronic subdural hematoma (d).
Case 3
A 53-year-old man presented with a severe orthostatic headache for longer than 1 month. No history of recent head trauma or medication was reported. A physical examination was unremarkable, except for neck stiffness. Head CT showed bilateral CSDH, collapse of the ventricular system, and effacement of the basal cisterns (Figure 4a, b). MRI showed brain sagging and elongation of the brainstem (Figure 4c). He was diagnosed with CSDH secondary to SCFH. Because he was stable, reinforced restriction of physical activity was proposed for the initial management. He experienced an uneventful recovery. Performance of CT 104 days later showed complete resolution of the CSDH and re-expansion of the ventricular system (Figure 4d).
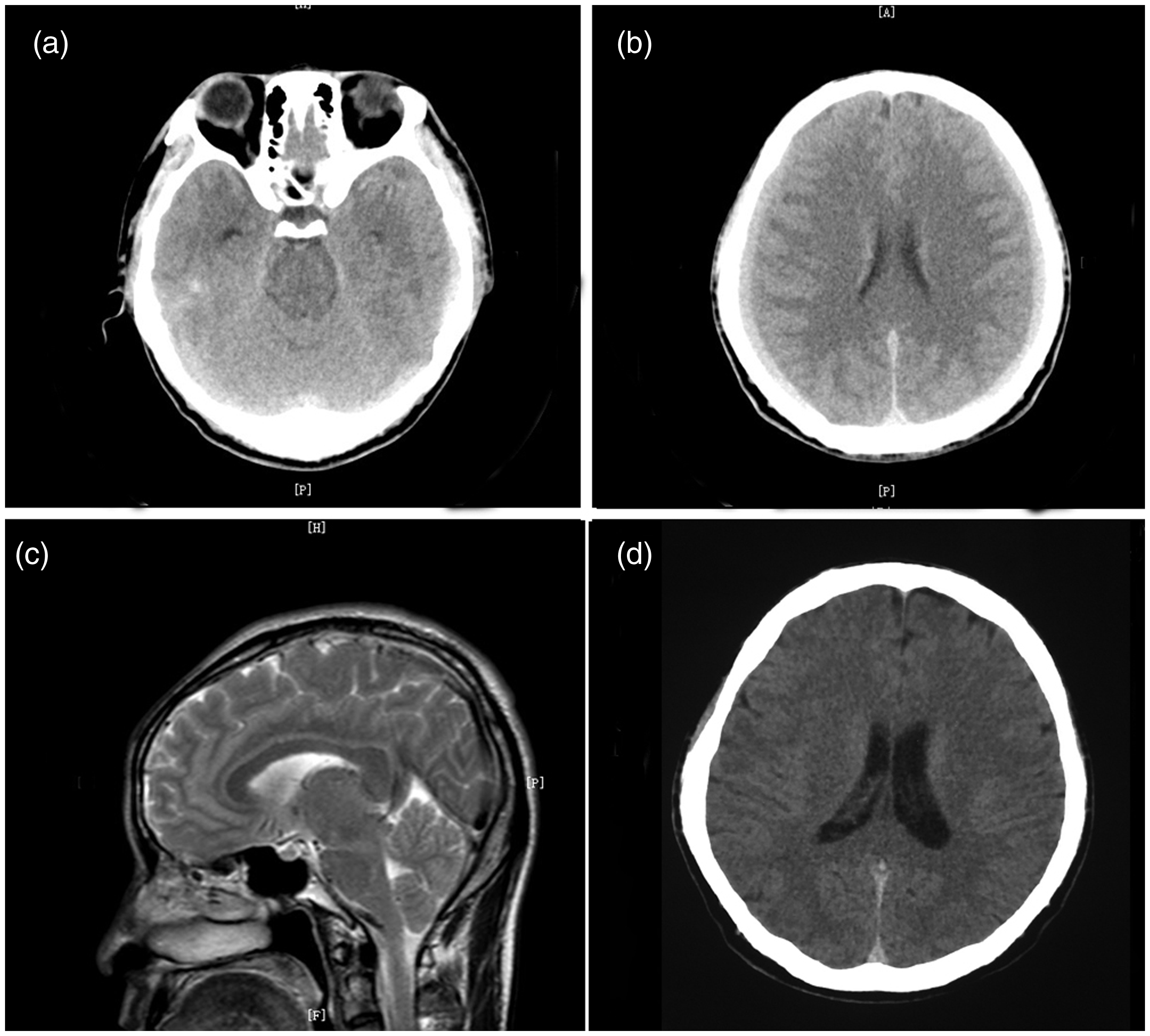
Computed tomography of case 3 shows effacement of the ambient cistern (a), collapse of the lateral ventricles, and bilateral isodense chronic subdural hematoma (b). Sagittal T2-weighted imaging on magnetic resonance imaging shows brain sagging (c). Computed tomography shows complete resolution of the CSDH (d).
Discussion
The pathophysiological mechanism of formation and progression of CSDH is not well understood at present. Recent evidence has shown that formation and progression of CSDH is a complex process that involves interaction of the inflammatory response, angiogenesis, and fibrinolysis. 8 Additionally, damage to the dural border cells plays a role as an initiator in this complex process. 8 However, all of the existing studies on the mechanism of CSDH were in patients secondary to trauma or undefined reasons. No specific study has investigated the underlying mechanism of CSDH formation in patients with SCFH. Therefore, management of CSDH in patients secondary to SCFH has not been based on the mechanism of CSDH in SCFH. However, we believe that management of CSDH should be based on the specific pathogenic mechanism because CSDH can result from a variety of factors.
SCFH is caused by occult spontaneous CSF leakage along the spinal dural mater. 1 The characteristic orthostatic headache and alterations in imaging investigations is a consequence of delayed recognition and management of CSF leakage in SCFH. Although the most common symptom of this entity is SIH, some authors believe that CSF hypovolemia might be more accurate in depicting the true nature.9,10 This notion is based on the following two facts: 1) a substantial proportion of patients with characteristic presentation of SIH regarding symptoms and imaging have normal CSF pressure; and 2) the characteristic alterations in imaging (collapse of the ventricular system, cisternal effacement, elongation of the brainstem, brain sagging, pachymeningeal enhancement, and subdural effusion) are due to depletion of CSF, but not to low intracranial pressure. We believe that CSF hypovolemia could more directly reflect the underlying mechanism of SIH. Substantial depletion of CSF compromises its buoyant effect on the brain, which subsequently leads to brain sagging. Persistent tractive force on the intracranial dura mater may injure the dural border cells, which activate a complex local cascade reaction of the inflammatory response, angiogenesis, and fibrinolysis. Delayed recognition and management ultimately lead to formation and progression of CSDH.
Generally, management of SCFH in patients without CSDH includes intravenous hydration, bed rest, and an epidural blood patch.3,4 An epidural blood patch has become the most effective or even standard procedure in patients with a defined source of spinal CSF leakage. However, management of SCFH in patients with massive CSDH is more complicated and challenging. Burr-hole drainage of CSDH, which is the most popular and straightforward surgical procedure in the general population, is not without risk in patients with SCFH. Some patients even experience fatal exacerbation after drainage of a CSDH.5,6 However, the rate of recurrence is relatively higher in patients with SCFH who undergo burr-hole drainage than in the general population.3,4,11
In our previous study, we showed the efficacy of reinforced restriction of physical activity on CSDH in the general population. 7 Generally, the criteria of reinforced restriction of physical activity include the following: a) avoiding any type of work that is routinely performed when they are diagnosed with CSDH; b) avoiding any type of physical exercise; c) walking no more than 1 km per 24 hours; and d) bed rest for no less than 10 hours per 24 hours. However, we believe that reinforced restriction of physical activity is restriction of physical activity in a specific time interval rather than a concrete rule. Until now, we have not achieved a consolidated consensus on the optimal extent of restriction of physical activity for patients with CSDH.
With reinforced restriction of physical activity, some stable patients could experience spontaneous resolution of the CSDH. According to our previous encouraging result, 7 we speculate that physical activity might play an important role in formation and progression of CSDH. We believe that this possibility is applicable to patients with SCFH. All of the current patients with massive CSDH experienced complete resolution and a favorable recovery with reinforced restriction of physical activity. Therefore, the current study not only provides an alternative option for managing CSDH secondary to SCFH, but also enriches the basic theory of formation and progression of CSDH. Additionally, reinforced restriction of physical activity could be used as an adjuvant management in stable patients with SCFH associated with massive CSDH.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics statement
Ethics approval was not required in our institution for this case report. Informed consent for participation in the study or use of medical data was obtained from the patient. Written consent was also obtained from the patient for publication of this manuscript and accompanying images.