
Abstract
Objective
To assess the prevalence, associated factors and cardiocerebral vascular prognosis of anaemia in patients undergoing haemodialysis.
Methods
This multicentre, retrospective, observational cohort study included patients on maintenance haemodialysis in South Guangdong, China. Anaemia in haemodialysis was defined as haemoglobin (Hb) <90 g/l. A proportion of patients were enrolled in a follow-up of the cardiocerebral vascular prognosis.
Results
A total of 1161 patients were enrolled and 938 were followed-up for cardiocerebral vascular events. Of 1161 patients, 250 (21.5%) had anaemia and 524 (45.1%) had an Hb level of 100–120 g/l. Adjusted multivariate logistic regression analysis demonstrated that frequency of dialysis ≤ twice weekly, hypoalbuminaemia and use of unfractionated heparin were independent factors associated with anaemia. Kaplan–Meier survival curve analysis for no myocardial infarction was 100%, 100%, 100% and 100% after 3, 6, 9 and 12 months, respectively, in patients with Hb < 90 g/l; compared with 97%, 95%, 93% and 93%, respectively, in patients with Hb ≥ 130 g/l. Adjusted Cox proportional hazards regression demonstrated that Hb ≥ 130 g/l was an independent risk factor for myocardial infarction.
Conclusion
Anaemia is highly prevalent among patients undergoing haemodialysis in South Guangdong and requires careful management.
Keywords
Introduction
Chronic kidney disease (CKD) is a global public health challenge that affects approximately 10% of the population worldwide, 1 including 120 million people in China. 2 Anaemia is a common complication of CKD, even in patients with CKD stage 3. 3 The prevalence of anaemia is higher in patients with CKD stages 4 and 5, with a nearly 10- and 50-fold risk, respectively. 3
According to data from the Dialysis Outcomes and Practice Patterns Study (DOPPS), 56.4% of patients in China met the targeted haemoglobin (Hb) level of 100–120 g/l, which was a lower proportion than that in Japan (89.2%) and North America (94.1%); and 21% of patients in China had Hb < 90 g/l, compared with 10% in Japan and 3% in North America. 4 Such findings in China are thought to reflect the low Hb levels in patients initiated on dialysis, with mean levels of 82 g/l reported in Beijing, 77 g/l in Shanghai and 73 g/l in Guangzhou. 5
The common correlative factors of anaemia in patients on haemodialysis include relative erythropoietin deficiency, impairment of intestinal iron absorption and release, recurrent blood loss, reduced erythrocyte survival duration, accumulation of uraemic toxins, microinflammation and hyperparathyroidism. 6 , 7 Several strategies for increasing the Hb level in patients on haemodialysis have been recommended, including optimal intravenous iron dosing, rational use of erythropoiesis-stimulating agents (ESAs), 8 improvement of dialysis adequacy by application of short daily haemodialysis and haemodiafiltration 9 , 10 and intensive treatment of hyperparathyroidism. 11 The management of anaemia in patients on haemodialysis is thought to be comprehensive.
Anaemia in CKD is associated with increased risks of death and complications. 12 A prior observational study demonstrated a strong association between low Hb level and increased risk of mortality in patients on dialysis. 13 However, the 2007 Kidney Disease Outcomes Quality Initiative (KDOQI) Clinical Practice Guideline recommended that the selected Hb target should generally be in the range of 110–120 g/l in dialysis and nondialysis patients with CKD receiving ESA therapy, but be no greater than 130 g/l (moderately strong evidence). 14 Research has demonstrated that greater ESA and iron use were associated with a decreased mortality risk in patients with a lower haematocrit level, in whom mortality rates are the highest. 15 In patients with a higher haematocrit level, although overall mortality was lower, these agents appeared to elevate mortality risk. 15 The Q-cohort study revealed that a low Hb level was reported to be associated with a high risk of haemorrhagic stroke, but not of ischaemic stroke. 16
Only sparse data were available on the prevalence of anaemia and anaemia monitoring for more than 1000 patients undergoing haemodialysis in Guangdong Province, China. Little is known about the relationship between different Hb levels and cardiocerebral vascular prognosis in the population of this region. This multicentre, retrospective, observational, cohort study assessed the prevalence, associated risk factors and cardiocerebral vascular prognosis of anaemia among patients on chronic haemodialysis in South Guangdong, China.
Patients and methods
Study population and design
This multicentre, retrospective, observational, cohort study recruited all consecutive adult patients undergoing maintenance haemodialysis between July 2017 and October 2017 in ten medical centres in South Guangdong, China. The inclusion criteria were as follows: (i) all adult patients undergoing maintenance haemodialysis in the ten medical centres; (ii) a dialysis frequency of twice or thrice weekly; (iii) a time on dialysis ≥3 months. The exclusion criteria were as follows: (i) history of haemoglobinopathy (thalassemia, pure red cell aplasia, myelodysplastic syndromes); (ii) malignant tumours; (iii) dysfunctional uterine bleeding. The observational follow-up duration was 12 months up to October 2018 during which the cardiocerebral vascular events, defined as myocardial infarction, cerebral infarction and cerebral haemorrhage, were recorded.
All ten participating centres followed the Blood Purification Standard Operating Procedure of Guangdong, China; and had passed the medical quality training and tests of the Guangdong Medical Association. The study was conducted in accordance with the principles of Good Epidemiology Practices and the Declaration of Helsinki. All the patients provided written informed consent for haemodialysis treatment. All patient details were de-identified.
Data collection
All demographic data as well as dialysis and biological parameters from the electronic medical records of each centre were collected using Epidata Entry 3.1.1203.2006 and verified by two secretaries from the central centre.
Dialysis parameters included the following: vascular access (arteriovenous fistulas/grafts [AVFs/AVGs] and deep vein catheterization [DVC]), dialyser type (high-flux and low-flux dialysers), anticoagulants (low-molecular-weight heparin [LMWH] and unfractionated heparin [UFH]), interdialytic weight gain and ultrafiltration rate (UFR; mean ultrafiltration volume [UFV] divided by dry weight), dialysis dose (Kt/v = –Ln(blood urea nitrogen [BUN] after dialysis[mmol/l]/BUN pre-dialysis[mmol/l]–0.008×dialysis time[h])+(4–3.5×BUN after dialysis/BUN pre-dialysis)×UFV([l]/dry weight[kg]) 17 and concomitant medication (iron supplement, doses of ESA). Pre- and post-dialysis arterial pressure and inter-dialysis weight gain and UFV were calculated as the mean of the recorded values during three separate dialyses.
Biological parameters (serum creatinine, uric acid, albumin, cholesterol, calcium, phosphate, parathyroid hormone, ferritin, and transferrin saturation [TSAT]) had been measured after an overnight fast before dialysis. The values of all the above parameters, medications, bleeding events during dialysis within 1 month preceding the time of each patient’s inclusion in the study were recorded. Anaemia in CKD patients on haemodialysis was defined as an Hb level < 90 g/l; and in these patients, the Hb target should be in the range of 110–120 g/l but not be greater than 130 g/l. 14 As a consequence, the Hb level, as a continuous quantitative variable, was analysed using four quartiles: Hb < 90 g/l (anaemia group), 90 ≤ Hb < 110 g/l, 110 ≤ Hb < 130 g/l (normal Hb [NHb] group) and Hb ≥ 130 g/l.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA). Quantitative variables with a normal distribution and homogeneity of variance are presented as mean ± SD and analysed using one-way analysis of variance (ANOVA). Variables that were not normally distributed or had non-homogeneity of variance are presented as median (interquartile range [IQR], Q25–Q75) and analysed using the Kruskal–Wallis test. Qualitative variables are presented as frequencies and analysed using the χ2-test (nominal variables) or Kruskal–Wallis test (ordinal variables). For further multiple comparisons, Bonferroni’s test was used for quantitative variables with a normal distribution and homogeneity of variance and nominal qualitative variables; while the Mann–Whitney U-test was used for quantitative variables that were not normally distributed or had non-homogeneity of variance and ordinal qualitative variables, with an Hb level 110 ≤ Hb < 130 g/l as reference.
A logistic regression model was used for multivariate analysis to identify the associated factors for anaemia in patients on haemodialysis. The incidence of cardiocerebral vascular adverse events were analysed using the Kaplan–Meier method and compared with the Log-rank test. A Cox proportional hazards regression model was used for multivariate analysis to identify the independent risk factors for prognosis.
All P-values were two-sided. A P-value < 0.05 was considered statistically significant in the ANOVA, Kruskal–Wallis and χ2-test, while P < 0.0167 was considered statistically significant in the Bonferroni and Mann–Whitney U-test.
Results
Of the total of 1172 patients on chronic haemodialysis that were enrolled in this study, 11 were excluded; three had thalassaemia, one had a history of pure red cell aplasia and seven had a malignant tumour. Thus, 1161 patients were included in the analysis. As shown in Table 1, the mean ± SD age of the study participants was 53.54 ± 14.68 years, 60.6% (703 of 1161 patients) were male, 47.5% (552 of 1161 patients) had primary glomerulonephritis as the primary cause of kidney failure and 17.9% (208 of 1161 patients) had diabetic nephropathy. The median time on dialysis was 31 months (IQR, 15–61 months). The demographic, clinical and laboratory characteristics according to the Hb level are shown in Tables 1 and 2. The mean ± SD Hb level was 104.11 ± 19.02 g/l (range, 35–160 g/l). Among these 1161 patients, 250 (21.5%) patients had anaemia (Hb < 90 g/l), 524 (45.1%) had an Hb level of 100–120 g/l and 264 (22.7%) had an Hb level of 110–120 g/l. The proportions of patients with an Hb < 90 g/l, 90 ≤ Hb< 110 g/l, 110 ≤ Hb < 130 g/l, and Hb ≥ 130 g/l were 21.5% (250 of 1161 patients), 38.0% (441 of 1161 patients), 32.6% (379 of 1161 patients) and 7.8% (91 of 1161 patients), respectively.
Demographic, clinical and dialysis parameters for patients (n = 1161) undergoing haemodialysis stratified according to their haemoglobin (Hb) levels.
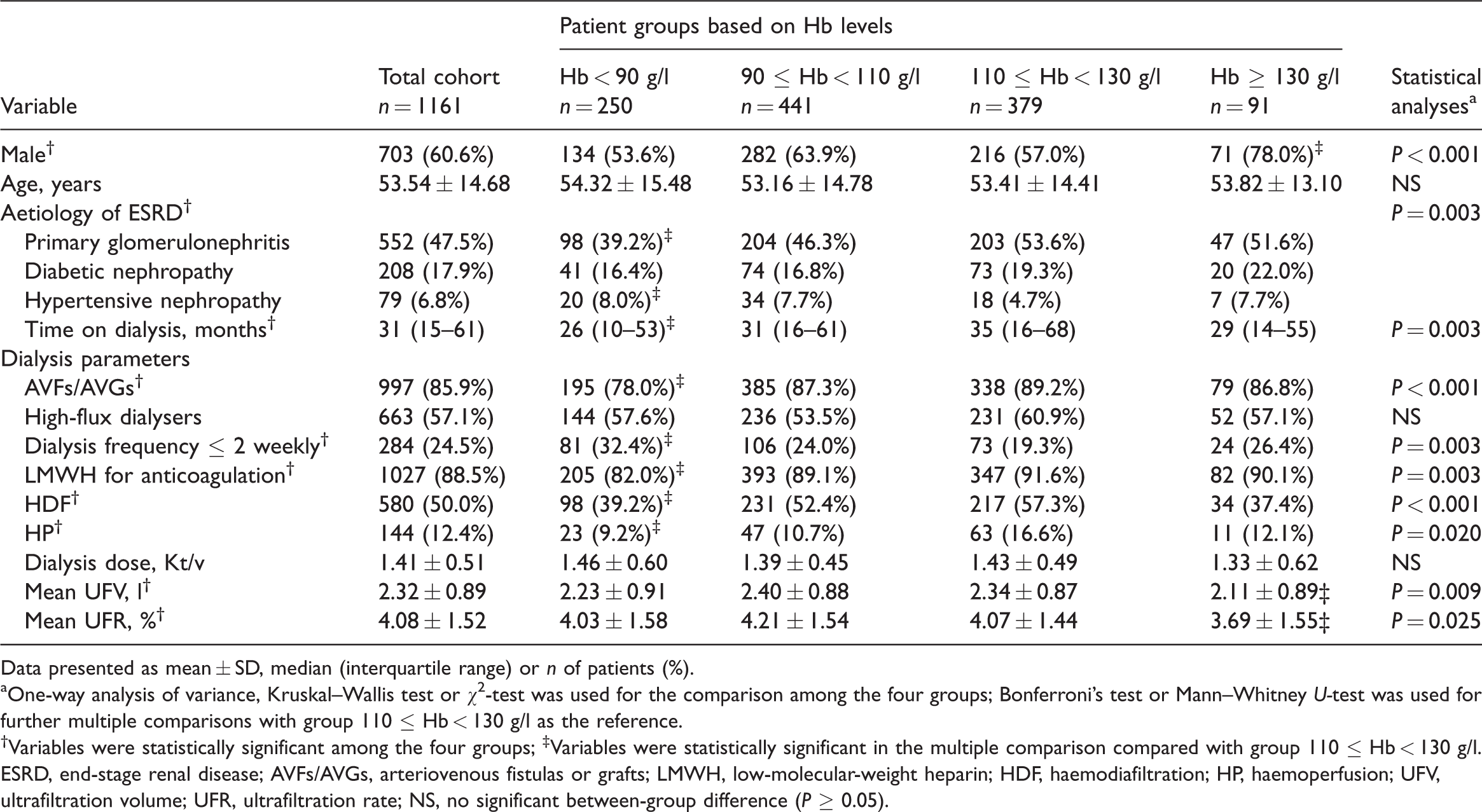
Data presented as mean ± SD, median (interquartile range) or n of patients (%).
aOne-way analysis of variance, Kruskal–Wallis test or χ2-test was used for the comparison among the four groups; Bonferroni’s test or Mann–Whitney U-test was used for further multiple comparisons with group 110 ≤ Hb < 130 g/l as the reference.
†Variables were statistically significant among the four groups; ‡Variables were statistically significant in the multiple comparison compared with group 110 ≤ Hb < 130 g/l.
ESRD, end-stage renal disease; AVFs/AVGs, arteriovenous fistulas or grafts; LMWH, low-molecular-weight heparin; HDF, haemodiafiltration; HP, haemoperfusion; UFV, ultrafiltration volume; UFR, ultrafiltration rate; NS, no significant between-group difference (P ≥ 0.05).
Laboratory and medication data for patients (n = 1161) undergoing haemodialysis stratified according to their haemoglobin (Hb) levels.

Data presented as mean ± SD, median (interquartile range) or n of patients (%).
aOne-way analysis of variance, Kruskal–Wallis test or χ2-test was used for the comparison among the four groups; Bonferroni’s test or Mann–Whitney U-test was used for further multiple comparisons with group 110 ≤ Hb < 130 g/l as the reference.
†Variables were statistically significant among the four groups; ‡Variables were statistically significant in the multiple comparison compared with group 110 ≤ Hb < 130 g/l.
ESA, erythropoiesis-stimulating agents; NS, no significant between-group difference (P ≥ 0.05).
Compared with the NHb group (110 ≤ Hb < 130 g/l), the anaemia group (Hb < 90 g/l) had a significantly higher proportion of patients with hypertensive nephropathy as the primary renal disease (8.0% [20 of 250 patients] versus 4.7% [18 of 379 patients], P = 0.003), a significantly shorter duration of dialysis (26 months [IQR, 10–53 months] versus 35 months [IQR, 16–68 months], P = 0.003), significantly more dialysis frequency ≤ twice weekly (32.4% [81 of 250 patients] versus 19.3% [73 of 379 patients], P = 0.003); and significantly less frequent use of AVFs/AVGs, LMWH, haemodiafiltration and haemoperfusion therapy (P < 0.05 for all comparisons) (Table 1). No significant differences were found between these two groups in sex, age, high-flux dialyser use, dialysis dose (Kt/v), UFV or UFR.
Compared with the NHb group (110 ≤ Hb < 130 g/l), the anaemia group (Hb < 90 g/l) had significantly lower levels of serum creatinine (P < 0.001), serum albumin (P < 0.001), serum triglyceride (P < 0.001) and serum calcium (P < 0.001) (Table 2). No significant differences were found in serum phosphorus and immunoreactive parathyroid hormone levels. Compared with the NHb group (110 ≤ Hb < 130 g/l), the anaemia group (Hb < 90 g/l) had significantly higher serum ferritin level (P = 0.007), but significantly lower TSAT level (P < 0.001). Regarding medication use, patients in the anaemia group (Hb < 90 g/l) used iron supplementation and ESA more significantly frequently than those in the NHb group (110 ≤ Hb < 130 g/l) (P < 0.001 for all comparisons), while the use of calcitriol and calcium was significantly less (P < 0.05 for both comparisons). Eight of 1161 (0.7%) and 12 of 1161 (1.0%) patients were diagnosed with gastrointestinal bleeding and cerebral haemorrhage, respectively, within 1 month preceding the recorded date of the biological data at baseline.
As presented in Table 3, the adjusted multivariate logistic regression analysis indicated that frequency of dialysis ≤ twice weekly (odds ratio [OR] 1.721; 95% confidence interval [CI] 1.201, 2.466; P = 0.003), hypoalbuminaemia (OR 2.112; 95% CI 1.463, 3.049; P < 0.001) and use of UFH (OR 1.822; 95% CI 1.104, 3.006; P = 0.019) were independent factors associated with anaemia in patients on haemodialysis.
Univariate and multivariate logistic regression analyses of the variables that were independently associated with anaemia in patients (n = 1161) undergoing haemodialysis.

aAll variables with a confirmed P-value < 0.05, age and time on dialysis were included in the multivariate logistic regression model.
bAll variables with a confirmed P-value < 0.05, age, time on dialysis, iron supplementation and erythropoiesis-stimulating agent doses were included in the multivariate logistic regression model.
cYes reference to No.
dDialysis ≤ twice weekly reference to dialysis ≥ thrice weekly.
eUFH reference to low-molecular-weight heparin.
OR, odds ratio; CI, confidence interval; AVFs/AVGs, arteriovenous fistulas or grafts; UFH, unfractionated heparin; HDF, haemodiafiltration.
Among the 1161 patients in the study at baseline, 938 eligible patients were enrolled in the cardiocerebral vascular prognostic follow-up research. Patients presented with time on dialysis < 3 months (n = 28), dialysis frequency of once weekly (n = 18), drop-out from the research medical centres (n = 142), kidney transplant (n = 30) or accidental death (n = 5) were excluded. After a median follow-up time of 12 months (IQR, 9–12 months), 19 of 938 patients (2.0%) had experienced new-onset myocardial infarction; 32 of 938 patients (3.4%) had experienced a cerebral infarction; and 13 of 938 patients (1.4%) had been diagnosed with new-onset cerebral haemorrhage (Table 4).
New-onset cardiocerebral vascular events during a median 12-month follow-up in patients (n = 938) undergoing haemodialysis stratified according to their haemoglobin (Hb) levels.

Data presented as n of patients (%).
a χ2-test was used for the comparison among the four groups; Mann–Whitney U-test was used for further multiple comparisons with group 90 ≤ Hb < 110 g/l as the reference.
†Variables were statistically significant among the four groups; ‡Variables were statistically significant in the multiple comparison compared with group 90 ≤ Hb < 110 g/l.
Kaplan–Meier survival curve analysis for no myocardial infarction was 100%, 100%, 100% and 100% after 3, 6, 9 and 12 months, respectively, in patients with Hb < 90 g/l; compared with 97%, 95%, 93% and 93%, respectively, in patients with Hb ≥130 g/l (P = 0.004) (Figure 1). No significant differences were demonstrated in survival of cerebral infarction or cerebral haemorrhage among the four groups with different haemoglobin levels (data not shown).

Kaplan–Meier survival curve analysis for no myocardial infarction during follow-up in patients (n = 938) undergoing haemodialysis stratified according to their haemoglobin (Hb) levels. The colour version of this figure is available at: http://imr.sagepub.com.
Adjusting for sex, age and time on dialysis, Cox proportional hazards regression model demonstrated that Hb ≥ 130 g/l (reference to Hb < 110 g/l, relative risk [RR] 10.565; 95% CI 2.478, 45.045; P = 0.001) and serum triglyceride (per 1 mmol/l increase, RR 1.217; 95% CI 1.047, 1.414; P = 0.010) were independent risk factors for myocardial infarction (Table 5).
Cox proportional hazards regression model analyses of the variables that were independently associated with myocardial infarction in patients (n = 938) undergoing haemodialysis.

aAll variables with a confirmed P-value < 0.05 were included in the multivariate Cox regression model.
bAll variables with a confirmed P-value < 0.05, age and time on dialysis were included in the multivariate Cox regression model.
cHb ≥ 130 g/l reference to Hb < 110 g/l.
RR, relative risk; CI, confidence interval; Hb, haemoglobin; TG, triglyceride.
Discussion
This current study investigated the prevalence of anaemia in 1161 patients receiving chronic haemodialysis in Southern Guangdong, China. Among these 1161 patients, 250 (21.5%) patients had anaemia (Hb < 90 g/l), 524 (45.1%) had an Hb level of 100–120 g/l and 264 (22.7%) had an Hb level of 110–120 g/l. While these preliminary results were consistent with the DOPPS data, 4 they show that the majority of patients on haemodialysis did not meet the recommended Hb target. These findings suggest that ongoing monitoring is crucial to improve anaemia management in patients receiving chronic haemodialysis.
This preliminary descriptive analysis showed that patients with anaemia presented a higher proportion of patients with hypertensive nephropathy as the primary renal disease, shorter duration of dialysis, less frequent use of AVFs/AVGs for dialysis access, less dialysis frequency per week, less haemodiafiltration or haemoperfusion therapy and less use of LMWH for anticoagulation compared with patients with normal Hb levels. The clinical parameters indicated that patients with anaemia had lower levels of serum creatinine, serum albumin, serum triglyceride and TSAT level, but a higher serum ferritin level and more iron supplementation and ESA therapy. After adjusting for age, sex, time on dialysis, iron supplementation and ESA doses, the current analysis found that frequency of dialysis ≤ twice weekly, hypoalbuminaemia and use of UFH for anticoagulation were independently associated with anaemia in patients undergoing haemodialysis. Based on the results above, we found out four characteristics in this population.
Based on the results shown above, this current study identified four characteristics in this patient population. First, patients with anaemia were more likely to have hypertensive nephropathy as their primary renal disease, which is thought of as a silent renal disease without obvious proteinuria, macrohaematuria or oedema that needs regular monitoring. The shorter time on dialysis and less frequent use of AVFs/AVGs for access suggested an urgent need for haemodialysis, which might be due to delayed referral to a nephrologist. Despite the widespread promotion of planned-start dialysis therapy for patients with advanced CKD, 18 , 19 some patients require acute dialysis to be initiated via a temporary DVC due to a life-threatening uremic emergency. In these patients, haemodialysis or peritoneal dialysis would be selected as a long-term dialysis modality following stabilization of their condition. Given the late referral for hospitalization, patients would likely have co-morbidities, such as severe anaemia and malnutrition. All the above suggest a lack of healthcare awareness in people in South Guangdong and more health education is required in the general population, especially in terms of kidney protection.
Secondly, patients with anaemia in the current study received dialysis at a lower frequency per week and less haemodiafiltration or haemoperfusion therapy compared with patients with normal Hb levels. Adjusted multivariate logistic regression analysis indicated that frequency of dialysis ≤ twice weekly was independently associated with anaemia in patients undergoing haemodialysis. Regular dialysis at a rate of thrice weekly is needed to ensure uraemic toxin and fluid clearance, with the appropriate haemodiafiltration or haemoperfusion therapy to enhance toxin clearance. These results indicated that the adequacy of haemodialysis plays an important role in Hb level improvement. Strategies have been proposed to increase the Hb level of patients on haemodialysis, including short daily haemodialysis, haemodiafiltration and intensive treatment of hyperparathyroidism.9–11 Short daily haemodialysis had been demonstrated to be associated with an improvement of hyperphosphataemia, secondary hyperparathyroidism, fluid management, left ventricular hypertrophy, blood pressure control, restless legs syndrome and sleep disturbances. 8 ,20–22 A recent study also found that short daily haemodialysis might improve nutritional status, which would promote anaemia improvement, compared with conventional haemodialysis in Chinese patients undergoing maintenance haemodialysis. 23 However, other factors, such as economic burdens, availability of caregivers and societal requirements, should be considered as possible reasons for many patients opting out of short daily haemodialysis. In our opinion, an improvement of dialysis adequacy, including a dialysis frequency of thrice weekly, appropriate use of haemodiafiltration or haemoperfusion, and intensive treatment of hyperparathyroidism, would help patients to achieve their target Hb level.
Thirdly, patients with anaemia in the current study had lower levels of serum creatinine, serum albumin and serum triglyceride compared with patients with normal Hb levels. Adjusted multivariate logistic regression analysis indicated that hypoalbuminaemia was an independent factor associated with anaemia in patients on haemodialysis. It is well known that Hb level is closely related to nutritional status. 24 Nutritional status in haemodialysis patients remains an important part of the management of haemodialysis. The recommended target of albumin in patients undergoing haemodialysis is 40 g/l. 25 However, an inappropriate diet may result in hyperphosphataemia, another troublesome complication. Although KDOQI guidance suggests that protein intake in patients undergoing maintenance haemodialysis should be 1.2 g/kg per day, research has demonstrated that a low protein intake (0.8 g/kg per day), low phosphorus intake (500 mg/day) and compound α-keto acid therapy effectively reduces serum phosphorus levels in patients undergoing maintenance haemodialysis while the nutritional status remained stable. 26 , 27 It will be important in the future to determine which type of diet is the most suitable for patients undergoing haemodialysis in order to improve their nutritional status.
Patients with anaemia in the current study had were less likely to receive LMWH for anticoagulation compared with patients with normal Hb levels. Adjusted multivariate logistic regression analysis indicated that the use of UFH was an independent factor associated with anaemia in patients on haemodialysis. Anticoagulation therapy is an important aspect of haemodialysis. UFH is the most common anticoagulation therapy used during haemodialysis in the United States due to its proven history, relative ease of use, safety and low cost. 28 However, the European Best Practice Guidelines for haemodialysis recommend the use of LMWH for extracorporeal circuit anticoagulation. 29 In northern China, the rates of LMWH use increased from 26.5% in 2007 to 42.1% in 2012. 30
According to a previous study, the risks of using UFH for anticoagulation during long-term haemodialysis included its short half-life, requiring continuous infusion and/or repeated boluses, heparin-induced thrombocytopenia, hypertriglyceridaemia, hyperkalaemia, bone mineral disease, anaphylaxis and bleeding due to the binding of UFH and antithrombin, which would inhibit both factor Xa and thrombin. 31 Recently, it has been reported that low-dose heparinization did not compromise dialysis adequacy and permitted ESA dose reduction for decreased rates of bleeding from the vascular access site at dialysis termination and occult bleeding from the gastrointestinal tract. 32 In a study from the 1990s, the authors reported that UFH might impact the susceptibility to ESAs. 33 Maybe microinflammation caused by anaphylaxis and hyperparathyroidism due to bone mineral disease, which are related to UFH use, would compromise the susceptibility to ESAs and erythropoiesis. Furthermore, another study found that lower doses of ESAs were required in patients receiving LMWH during haemodialysis. 34 These results suggest that LMWH might improve the susceptibility towards ESAs and even the balance of iron, thereby promoting Hb level improvement. In fact, the current analysis demonstrated that patients in the anaemia group, with a higher proportion of UFH use, had a higher level of ferritin and a lower level of TSAT, which implied sufficient iron storage but scant iron availability, and more frequently used iron supplements and ESAs.
Anaemia is a potential nontraditional risk factor for cardiovascular disease and it is primarily a risk factor for adverse outcomes in those who also have CKD. 35 In contrast, this current study demonstrated that patients with Hb ≥ 130 g/l had a higher risk of myocardial infarction. Adjusting for sex, age at presentation, and duration of dialysis, Cox proportional hazards regression model indicated that Hb ≥ 130 g/l (reference to Hb < 110 g/l) was one of the independent risk factors for myocardial infarction. There were no differences in cerebral vascular prognosis in patients with different Hb levels.
The target haemoglobin level in patients undergoing haemodialysis is 100–120 g/l and should not exceed 130 g/l. 14 Results from the ‘Trial to Reduce Cardiovascular Events with Aranesp Therapy’ indicated that rapid increases in Hb level should probably be avoided and the temptation to increase ESA doses to very high levels in an attempt to reach a target Hb level greater than 120–130 g/l had not demonstrated a clinical benefit in terms of mortality, morbidity or quality of life improvement. 36 Another prospective, observational, multicentre study demonstrated that cardiocerebral vascular disease, infection and hospitalization were higher among patients that were treated with high weekly doses of intravenous iron compared with no intravenous iron. 37 A retrospective descriptive study in patients undergoing peritoneal dialysis demonstrated that those that maintained high Hb values (≥110 g/l) were more likely to develop recurrent cardiovascular events than patients with relatively low Hb values (<110 g/l). 38 Close attention needs to be paid to striking a balance between providing positive therapy for anaemia and achieving the appropriate target Hb level in this group of patients.
Although existing studies have demonstrated that anaemia in patients undergoing haemodialysis is related to erythropoietin deficiency, impairment of intestinal iron absorption and release, recurrent blood loss, microinflammation, hyperparathyroidism and dialysis deficiency, 6 , 7 there were several new findings from this current study. Patients with anaemia undergoing chronic haemodialysis from South Guangdong had delayed-start, low-frequency dialysis therapy and worse nutritional status. Interestingly, the study also found that the use of UFH for anticoagulation was an independent risk factor for anaemia in these patients. In a study from the 1990s, the authors reported that UFH might impact the susceptibility to ESAs, but no further confirmation of this finding was undertaken. 33 Nonetheless, investigating whether the use of LMWH would improve the susceptibility to ESAs, iron balance and microinflammatory status should be weighed against its cost. This research group plans to investigate the relationship between UFH, LMWH and Hb levels in patients on haemodialysis in the future.
Meanwhile, according to the target Hb level in the 2007 KDOQI guidelines, this current study demonstrated the relationship between Hb ≥130 g/l and myocardial infarction in this patient population. It should be noted that as a retrospective study, it only focused on the Hb levels at baseline. More research regarding the Hb levels over time, Hb level fluctuations during follow-up and vascular events after a longer follow-up period should be undertaken.
This study had several limitations. Due to its multicentre, retrospective, cohort study design, there were time deviations for several variables such as dialysis parameters, laboratory findings, medication doses and complication recordings. Therefore, a prospective cohort study with long-term follow-up or randomized controlled clinical trials will be required to validate the conclusions from this preliminary study.
In conclusion, this current retrospective cohort study found that 21.5% of patients on haemodialysis in South Guangdong had anaemia. Hypoalbuminaemia, frequency of dialysis ≤ twice weekly and use of UFH for anticoagulation were identified as independent risk factors for anaemia. The selection of anticoagulants in this population may require greater attention, in addition to the adequacy of the dialysis and the patients’ nutritional status. Patients with Hb ≥ 130 g/l were at an increased risk of myocardial infarction. Clinicians need to pay close attention to achieving a balance between providing positive therapy for anaemia and maintaining the appropriate target Hb level in this group of patients.
Footnotes
Acknowledgements
We would like to thank the members of the Southern Guangdong: Improving Outcome of Kidney Disease (SOGOOD) group: Guohui Liu (Department of Nephrology, Dongguan People’s Hospital, Guangdong, China); Yuping Chen (Department of Nephrology, The First people’s Hospital of Zhaoqing, Guangdong, China); Guoliang Xiong (Department of Nephrology, Shenzhen Traditional Chinese Medicine Hospital, Guangdong, China); Wen Zhao (Department of Nephrology, The Second People’s Hospital of Futian District Shenzhen, Guangdong, China); Dong Chen (Department of Nephrology, Baoan Central Hospital of Shenzhen, Guangdong, China); Xingming Tang (Haemopurification Department, Tungwah Hospital of Sun Yat-sen University, Dongguan, Guangdong, China); Zhen Ma (Department of Nephrology, Guangzhou Hospital of Integrated Traditional and West Medicine, Guangdong, China); Xianrui Dou (Department of Nephrology, Shunde Hospital of Southern Medical University, Guangdong, China).
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Nature Science Foundation of China (no. 81470953).